Midazolam For Status Epilepticus
Midazolam For Status Epilepticus
Download as pdf or txt
You might also like
- When To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsDocument9 pagesWhen To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsLexipol_Media_GroupNo ratings yet
- Life Saving DrugsDocument7 pagesLife Saving DrugsJozel Cuanico100% (3)
- Updated Marketing Project For MBADocument99 pagesUpdated Marketing Project For MBAadamodharNo ratings yet
- Pediatric PharmacotherapyDocument4 pagesPediatric PharmacotherapyOasis LimitedNo ratings yet
- Midazolam Hydrochloride Inj 45836CDocument4 pagesMidazolam Hydrochloride Inj 45836CjuanNo ratings yet
- Midasiz 1Document9 pagesMidasiz 1arghyadeepbose24No ratings yet
- Buletin HS Bil3.2020Document14 pagesBuletin HS Bil3.2020Shaharaman ShariNo ratings yet
- Bottomley 1990Document3 pagesBottomley 1990Benjamin W. ThomasNo ratings yet
- Midazolam Injection: New Zealand Data SheetDocument14 pagesMidazolam Injection: New Zealand Data SheetAlin AdelineNo ratings yet
- Pharmacological Methods of Behaviour ManagementDocument41 pagesPharmacological Methods of Behaviour ManagementSuma 123No ratings yet
- Status Epilepticus Pediatric DR - RPDocument4 pagesStatus Epilepticus Pediatric DR - RPAdnin NugrohoNo ratings yet
- Midazolam in j PfizerDocument26 pagesMidazolam in j PfizerbelloNo ratings yet
- Midazolam Drug AbuseDocument3 pagesMidazolam Drug AbuseandrianhoerulanwarNo ratings yet
- Knight (2013) Diazepam Use in Captive Botlenose DolphinsDocument4 pagesKnight (2013) Diazepam Use in Captive Botlenose DolphinsJustin Michael JeromeNo ratings yet
- RX in Pediatric DentistryDocument34 pagesRX in Pediatric DentistryMohammed AlhayaniNo ratings yet
- Efficacy and Safety of Intramuscular Midazolam Versus Rectal Diazepam in Controlling Status Epilepticus in ChildrenDocument6 pagesEfficacy and Safety of Intramuscular Midazolam Versus Rectal Diazepam in Controlling Status Epilepticus in ChildrenMadeNo ratings yet
- Rescue Treatment SeizuresDocument3 pagesRescue Treatment Seizureseko aNo ratings yet
- Oral Midazolam For Conscious Sedation of ChildrenDocument5 pagesOral Midazolam For Conscious Sedation of ChildrenRay KwanNo ratings yet
- Myasthenia Gravis: Association of British Neurologists' Management GuidelinesDocument14 pagesMyasthenia Gravis: Association of British Neurologists' Management Guidelinesafm26No ratings yet
- Clemency 2014Document6 pagesClemency 2014Syed Mohsin Ali ShahNo ratings yet
- Dexamethasone FDG Mar 14Document2 pagesDexamethasone FDG Mar 14salimskaini1990No ratings yet
- Pediatric Emergency Care Volume Issue 2017 Doi 10.1097PEC.000000000000111Document5 pagesPediatric Emergency Care Volume Issue 2017 Doi 10.1097PEC.000000000000111Syukri Be DeNo ratings yet
- Comparison of Intranasal Midazolam With Intravenous Diazepam For Treating Febrile Seizures in Children: Prospective Randomised StudyDocument4 pagesComparison of Intranasal Midazolam With Intravenous Diazepam For Treating Febrile Seizures in Children: Prospective Randomised StudyPutri Cyntia DewiNo ratings yet
- 445 FullDocument5 pages445 FullsiscaNo ratings yet
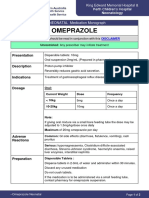
- Omeprazole 2018: Newborn Use OnlyDocument5 pagesOmeprazole 2018: Newborn Use OnlyHengky AntonNo ratings yet
- AHFS Drug InformationDocument10 pagesAHFS Drug InformationMika FebryatiNo ratings yet
- Treatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodDocument9 pagesTreatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodampalNo ratings yet
- Midazolam Review LaDocument11 pagesMidazolam Review LabellaNo ratings yet
- Midazolam 5mg in 1ml Injection - UK ReferenceDocument11 pagesMidazolam 5mg in 1ml Injection - UK ReferenceDilawar BakhtNo ratings yet
- pil.15365Document2 pagespil.15365nknkrabeaNo ratings yet
- Ijpd 22 303Document6 pagesIjpd 22 303bellaNo ratings yet
- HypersalivationDocument2 pagesHypersalivationosteoporosisclinicNo ratings yet
- PDFDocument9 pagesPDFRyan 21No ratings yet
- Intravenous Treatment of Migraine: Sait Ashina, Russell K. PortenoyDocument5 pagesIntravenous Treatment of Migraine: Sait Ashina, Russell K. PortenoyJess MelMedNo ratings yet
- Adjuvant Analgesics For Pain Management FINAL PARTDocument13 pagesAdjuvant Analgesics For Pain Management FINAL PARTbalamuruganNo ratings yet
- Antiepileptic Drugs and Liver Disease 2017Document14 pagesAntiepileptic Drugs and Liver Disease 2017Pablo Sebastián SaezNo ratings yet
- Pediatric DexmedetomidinDocument7 pagesPediatric DexmedetomidinLuis BachillerNo ratings yet
- RSI Post IntubationDocument8 pagesRSI Post IntubationshinjiNo ratings yet
- En A09v83n2s0 PDFDocument12 pagesEn A09v83n2s0 PDFRiriNo ratings yet
- Manejo de La Migraña PedDocument6 pagesManejo de La Migraña PedtatauribegNo ratings yet
- 983-Zoran Bojanic-DRUG INTERACTIONS WITH DIAZEPAM PDFDocument7 pages983-Zoran Bojanic-DRUG INTERACTIONS WITH DIAZEPAM PDFAnonymous JvptVyNsNo ratings yet
- BENZODIAZEPINESDocument20 pagesBENZODIAZEPINESHamza DossaNo ratings yet
- Use of Oral Midazolam Sedation in Pediatric Dentistry: A ReviewDocument13 pagesUse of Oral Midazolam Sedation in Pediatric Dentistry: A ReviewNicoll SQNo ratings yet
- DormitolDocument1 pageDormitolRamboNo ratings yet
- OmeprazoleDocument2 pagesOmeprazolephawphawphawNo ratings yet
- Mekanisme Aksi DiazepamDocument4 pagesMekanisme Aksi DiazepamWijaya Kusuma MaheruNo ratings yet
- 2 PDFDocument5 pages2 PDFMuhammad FachrurozieNo ratings yet
- ValiumDocument1 pageValiumJess MatiasNo ratings yet
- BNF - 76 - British - National - Formulary - Septem-357-358 PhenobarbtalDocument2 pagesBNF - 76 - British - National - Formulary - Septem-357-358 Phenobarbtalnur aisahNo ratings yet
- Pro Pre Medication in NeonatesDocument31 pagesPro Pre Medication in Neonateselizeushanindito8113No ratings yet
- Intranasal MidazolamDocument1 pageIntranasal MidazolamamithaNo ratings yet
- Ppa 7 027 PDFDocument9 pagesPpa 7 027 PDFbellaNo ratings yet
- MC HydroxyzineDocument3 pagesMC HydroxyzineCliff by the seaNo ratings yet
- Book 9Document3 pagesBook 9Gratiana TimisNo ratings yet
- Sedacion en PediatriaDocument5 pagesSedacion en PediatriaAlejandro Duque CalderonNo ratings yet
- Ref 1zzzaDocument5 pagesRef 1zzzaYudha FerriansyahNo ratings yet
- Oschman 2011Document6 pagesOschman 2011Cee AsmatNo ratings yet
- Ambulance Pocket BookDocument36 pagesAmbulance Pocket BooknapoleonmNo ratings yet
- Management of SE (Latest)Document34 pagesManagement of SE (Latest)dhinanadhiraNo ratings yet
- Pharmacological Behavior ManagementDocument45 pagesPharmacological Behavior Managementdeepesh jaiswalNo ratings yet
- Buccal Midazolam GuidelineDocument5 pagesBuccal Midazolam GuidelineAnwarrudin AsniNo ratings yet
- Top 100 Drugs Pocket Reference Guide (2023 Edition)From EverandTop 100 Drugs Pocket Reference Guide (2023 Edition)No ratings yet
- Malaria Treatment TableDocument9 pagesMalaria Treatment Tableاحمد عرفاتNo ratings yet
- Product ID Label NameDocument1,759 pagesProduct ID Label NameksoterixNo ratings yet
- Pharmacology NotesDocument2 pagesPharmacology Notessakuragi jakeNo ratings yet
- BMD225: Biomedical Pharmacology Workshop 3: Exercise 1Document3 pagesBMD225: Biomedical Pharmacology Workshop 3: Exercise 1Martina AllersNo ratings yet
- PHARMACOLOGY HAQs 2ND EdDocument27 pagesPHARMACOLOGY HAQs 2ND Edmbbsboy753No ratings yet
- List of Pharmaceutical Companies in Pune PDFDocument5 pagesList of Pharmaceutical Companies in Pune PDFMain Sanatani HunNo ratings yet
- Pharmacology Test 3 - Cardiovascular Drugs, Part I Flashcards - QuizletDocument10 pagesPharmacology Test 3 - Cardiovascular Drugs, Part I Flashcards - QuizletBhopesh Kadian0% (1)
- Semantic Project FFDocument11 pagesSemantic Project FFHabtamu AlebelNo ratings yet
- NDDSDocument9 pagesNDDSSaran VijayNo ratings yet
- Regulatory and Pharmacological Basis of Ayurvedic FormulationsDocument349 pagesRegulatory and Pharmacological Basis of Ayurvedic FormulationsS100% (1)
- Tugas Anestesi Muscle RelaxanDocument29 pagesTugas Anestesi Muscle RelaxanAiny NataliaNo ratings yet
- Careers 1Document110 pagesCareers 1Rajesh AnthonyNo ratings yet
- Lipid Lowering Agents IDocument14 pagesLipid Lowering Agents IRALPH ELVIN MACANLALAYNo ratings yet
- Pulmonary PharmacologyDocument8 pagesPulmonary PharmacologyJunam DisimbanNo ratings yet
- The Sedative/Hypnotics: Durmishkhan Akhsabadze, MDDocument79 pagesThe Sedative/Hypnotics: Durmishkhan Akhsabadze, MDminakshi bossNo ratings yet
- Drugs For The Treatment of AidsDocument17 pagesDrugs For The Treatment of AidsEdgar David SigarlakiNo ratings yet
- No Nama Obat Kemasan No - Batch Harga FEB MAR April MEI JUN JUL JML Rata2Document15 pagesNo Nama Obat Kemasan No - Batch Harga FEB MAR April MEI JUN JUL JML Rata2hermansyah liaNo ratings yet
- Optimalisasi Peran Apoteker Dalam Pelayanan Klinis (Apt. L. Endang Budiarti)Document37 pagesOptimalisasi Peran Apoteker Dalam Pelayanan Klinis (Apt. L. Endang Budiarti)Dimas RfNo ratings yet
- Medici Di Makati CollegeDocument3 pagesMedici Di Makati CollegeMaria Garcia Pimentel Vanguardia IINo ratings yet
- Mpharm - pc1 - Syall BY JNTUK - 1Document10 pagesMpharm - pc1 - Syall BY JNTUK - 1Sri SriNo ratings yet
- Section 2.0 Active Ingredients: (S) - MethopreneDocument71 pagesSection 2.0 Active Ingredients: (S) - Methopreneakhilkhattar1No ratings yet
- Wa0004Document2 pagesWa0004tymommunhemoNo ratings yet
- CP 2Document24 pagesCP 2Bandameedi RamuNo ratings yet
- Sites and Key ContactsDocument13 pagesSites and Key Contactssketcher315No ratings yet
- PEBC Qualifying Exam References and Resources ListDocument5 pagesPEBC Qualifying Exam References and Resources ListAnkit ShahNo ratings yet
- The Role of Dispensers in The Rational Use of DrugsDocument19 pagesThe Role of Dispensers in The Rational Use of DrugsAci Lusiana100% (1)
- New Product Priority List For Development - Oct 2020Document46 pagesNew Product Priority List For Development - Oct 2020GaFf ArNo ratings yet
- DiureticDocument40 pagesDiuretichoneyworksNo ratings yet