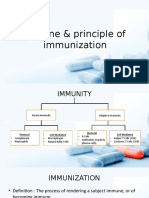
Immunization
Immunization
Download as pdf or txt
You might also like
- The Fitness ChefDocument342 pagesThe Fitness ChefIulia Florina Sima100% (8)
- ImmunityDocument46 pagesImmunityLalyn Balasbas100% (2)
- ABB Recloser Brochure 1VAL2601-TG Rev GDocument32 pagesABB Recloser Brochure 1VAL2601-TG Rev Gyana_harsana100% (1)
- Methyl SalicylateDocument10 pagesMethyl Salicylatekab56067% (3)
- ImmunizationDocument30 pagesImmunizationAhmed Ali100% (1)
- Vaccination ImmunizationDocument54 pagesVaccination Immunizationraja iramNo ratings yet
- Materi ImunisasiDocument49 pagesMateri ImunisasiChoco ChipNo ratings yet
- ImmunizationDocument46 pagesImmunizationfataoabudu93No ratings yet
- ImmunizationDocument23 pagesImmunizationAisha Haruna Ya’uNo ratings yet
- ImD-Med L4 (Immunization)Document33 pagesImD-Med L4 (Immunization)VancopNo ratings yet
- 4 - Immune VaccinationDocument59 pages4 - Immune Vaccinationmhmdmhyaldynh2No ratings yet
- Lecture - Immunization and VaccinesDocument40 pagesLecture - Immunization and Vaccinesrockyrawat01012003No ratings yet
- ImmunizationDocument54 pagesImmunizationkarl abiaadNo ratings yet
- Imunizarea Si Vaccinologia: ImunitateaDocument13 pagesImunizarea Si Vaccinologia: ImunitateaLoredana CîrlanNo ratings yet
- CCMP - Vaccination in ChildrenDocument49 pagesCCMP - Vaccination in ChildrenSnehal PatilNo ratings yet
- Immunity EPIDocument37 pagesImmunity EPIluttomiayvonneNo ratings yet
- VaccinationDocument28 pagesVaccinationM AQIB ASLAMNo ratings yet
- ImmunizationDocument53 pagesImmunizationMATHS By AbdulrahmanNo ratings yet
- Immunity & Principles of VaccinationDocument27 pagesImmunity & Principles of VaccinationAniruddha RoyNo ratings yet
- Vaksin Dan SeraDocument54 pagesVaksin Dan SeraFuriNo ratings yet
- Immunity & Principles of VaccinationDocument27 pagesImmunity & Principles of VaccinationReynaldiSanjayaNo ratings yet
- Immunology 13Document32 pagesImmunology 13letskeep0No ratings yet
- Acquired ImmunityDocument22 pagesAcquired ImmunityWilliam C ChishaNo ratings yet
- CHN Immunization NotesDocument9 pagesCHN Immunization NotesJustin AncogNo ratings yet
- ImmunizationDocument49 pagesImmunizationyosephNo ratings yet
- VaccinationDocument55 pagesVaccinationEbaNo ratings yet
- IMMUNIZATIONDocument24 pagesIMMUNIZATIONNurul AfifahNo ratings yet
- Chapter 12 Basic ImmunologyDocument39 pagesChapter 12 Basic ImmunologyTofik100% (1)
- Chapter # 79 - ImmunoprophylaxisDocument12 pagesChapter # 79 - Immunoprophylaxismuhammadjunaid2910No ratings yet
- ImmunizationDocument24 pagesImmunizationAhmed Azeez100% (1)
- Vaccine 2022Document10 pagesVaccine 2022aagrawalNo ratings yet
- Immuno ProphylaxisDocument25 pagesImmuno Prophylaxisقاسم اليوسفيNo ratings yet
- Unit 11 ImmunizationDocument45 pagesUnit 11 ImmunizationBikash Kandel100% (1)
- 5.14 Immunoprophylaxis ImmunotherapyDocument60 pages5.14 Immunoprophylaxis ImmunotherapyAlberto MayorgaNo ratings yet
- ImmunityDocument47 pagesImmunityraghad.21No ratings yet
- MDSC 3313 Immunisations Immunotherapy 2023Document41 pagesMDSC 3313 Immunisations Immunotherapy 2023Shandev IndoiNo ratings yet
- Vaccination_lecture_2019_v3Document45 pagesVaccination_lecture_2019_v3zakyzezoNo ratings yet
- Split PDF 030224 7.37.42Document11 pagesSplit PDF 030224 7.37.42ayushi693shindeNo ratings yet
- LMMU MICRO 2010 - Vaccinology 2024Document27 pagesLMMU MICRO 2010 - Vaccinology 2024mctime35No ratings yet
- Immunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityDocument35 pagesImmunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityadystiNo ratings yet
- Unza NRS 3110 - VaccinologyDocument27 pagesUnza NRS 3110 - VaccinologyTabitha Lumbwe PhiriNo ratings yet
- Immunoprophylaxis 2023513822500Document37 pagesImmunoprophylaxis 2023513822500mmkum122jaoNo ratings yet
- Vaccination ImmunizationDocument38 pagesVaccination ImmunizationtdisnahNo ratings yet
- Lecture 9 - Immunizing AgentsDocument48 pagesLecture 9 - Immunizing Agentsmanha hanzalNo ratings yet
- Immunization: Presenter: Ahmad Tahir Siti Nurul Farahah Supervised By: DR MuhaireenDocument40 pagesImmunization: Presenter: Ahmad Tahir Siti Nurul Farahah Supervised By: DR MuhaireenNadia SalwaniNo ratings yet
- Vaccine & Principle of ImmunizationDocument23 pagesVaccine & Principle of ImmunizationSindhu Babu100% (1)
- Principles of VaccinationDocument21 pagesPrinciples of VaccinationAlexandru ComanNo ratings yet
- Adult ImmunizationDocument48 pagesAdult ImmunizationMangesh JadhavNo ratings yet
- Vaccine Cold Chain Aefi Immunization CardDocument109 pagesVaccine Cold Chain Aefi Immunization Carddhruv kathuriaNo ratings yet
- Vaccines Science PharmaDocument30 pagesVaccines Science PharmaGanesh V GaonkarNo ratings yet
- Vaccination 2Document15 pagesVaccination 2mandeepkaur045No ratings yet
- MPH 1St Semester: SHM 502 Essentials of Public Health-Lecture Five Compiled and Facilitated by Shaoor Iqbal MSC - MPHDocument33 pagesMPH 1St Semester: SHM 502 Essentials of Public Health-Lecture Five Compiled and Facilitated by Shaoor Iqbal MSC - MPHamin khanNo ratings yet
- VaccinesDocument37 pagesVaccinesIqra fiazNo ratings yet
- VaccinationDocument35 pagesVaccinationmuneebazmat1123No ratings yet
- Immunization 1Document99 pagesImmunization 1shahaman1948No ratings yet
- Bio PrevDocument20 pagesBio PrevkemalNo ratings yet
- IT 2 - Imunisasi Anak - YLIDocument111 pagesIT 2 - Imunisasi Anak - YLIsamuel_hilda100% (1)
- Vaccine CDCDocument40 pagesVaccine CDCnasibdinNo ratings yet
- Pediatric - VaccinationDocument4 pagesPediatric - VaccinationKhaldoun AlmomaniNo ratings yet
- Lecture 3.2 - VaccinesDocument29 pagesLecture 3.2 - VaccinesQaphela MinenhleNo ratings yet
- Vaccination: How Millions of Lives Have Been Saved - Perhaps YoursFrom EverandVaccination: How Millions of Lives Have Been Saved - Perhaps YoursNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- Uv Disinfection of Some of The Fruit Juices: Provided by Dspace@Iztech Institutional RepositoryDocument95 pagesUv Disinfection of Some of The Fruit Juices: Provided by Dspace@Iztech Institutional RepositoryHafsah ShoaibNo ratings yet
- 2019 Bte 014 (Hafsahshoaib)Document10 pages2019 Bte 014 (Hafsahshoaib)Hafsah ShoaibNo ratings yet
- 2019 Bte 014 (Microbial)Document7 pages2019 Bte 014 (Microbial)Hafsah ShoaibNo ratings yet
- PharmacogeneticsDocument18 pagesPharmacogeneticsHafsah ShoaibNo ratings yet
- Carcinogenesis and Cell CycleDocument46 pagesCarcinogenesis and Cell CycleHafsah ShoaibNo ratings yet
- Carcinogenesis - Arno HelmbergDocument4 pagesCarcinogenesis - Arno HelmbergHafsah ShoaibNo ratings yet
- Lec1 Cancer Molecular Basis DrMokhtarDocument42 pagesLec1 Cancer Molecular Basis DrMokhtarHafsah ShoaibNo ratings yet
- Lab 5a The Literature of EcologyDocument3 pagesLab 5a The Literature of EcologyHafsah ShoaibNo ratings yet
- Purlins Analysis and DesignDocument6 pagesPurlins Analysis and DesignJestoni Gonzales TortolaNo ratings yet
- Shakespeares Julius Caesar in A Latin TR PDFDocument70 pagesShakespeares Julius Caesar in A Latin TR PDFporcelaindoctorNo ratings yet
- 2B201-324E - D - Aquilion3264 Trouble ShootingDocument37 pages2B201-324E - D - Aquilion3264 Trouble ShootingEmmanuel Virtudazo100% (1)
- AmulyaDocument6 pagesAmulyaJaya ChandranNo ratings yet
- Ebook: Applications of EDEM For SteelmakingDocument13 pagesEbook: Applications of EDEM For SteelmakingSergio DiazNo ratings yet
- A Railtrack Case StudyDocument8 pagesA Railtrack Case StudyPrabubroto JaunandarNo ratings yet
- ExamView - Chapter - 01-02Document9 pagesExamView - Chapter - 01-02José Yorki Rodríguez RodríguezNo ratings yet
- Full Video Production Handbook Fourth Edition Gerald Millerson C.Eng Miee Msmpte Ebook All ChaptersDocument70 pagesFull Video Production Handbook Fourth Edition Gerald Millerson C.Eng Miee Msmpte Ebook All Chapterstchatochazz100% (12)
- Electrical System Sheet (ESS) : Submission DeadlineDocument21 pagesElectrical System Sheet (ESS) : Submission DeadlineSaransh PandeyNo ratings yet
- Sample C.V.Document4 pagesSample C.V.Fatema ShabbirNo ratings yet
- Unit Plan For WeeblyDocument21 pagesUnit Plan For Weeblyapi-452290042No ratings yet
- Cat Pneumatic Tools: The Power To Get The Job DoneDocument4 pagesCat Pneumatic Tools: The Power To Get The Job DoneJean Jacques ouandaNo ratings yet
- "Free Radicals", Contain at Least One Unpaired Electron, A Clear Violation of The Octet RuleDocument9 pages"Free Radicals", Contain at Least One Unpaired Electron, A Clear Violation of The Octet RuleUsman GhaniNo ratings yet
- Inanna Hyper-LuminalDocument49 pagesInanna Hyper-LuminalMaria Eugenia SusNo ratings yet
- DLP SCIENCE YEAR 3 - ANIMALS CHARACTERISTICS - Print - QuizizzDocument9 pagesDLP SCIENCE YEAR 3 - ANIMALS CHARACTERISTICS - Print - QuizizzpiriyachandranNo ratings yet
- Humble Homemade Hifi - CalpamosDocument15 pagesHumble Homemade Hifi - CalpamoshsNo ratings yet
- Wide Band AntennasDocument8 pagesWide Band AntennasDmk ChaitanyaNo ratings yet
- Adaptation Lesson PlanDocument32 pagesAdaptation Lesson PlanCrystal PennypackerNo ratings yet
- The Tempest Story PDFDocument86 pagesThe Tempest Story PDFK.RoweNo ratings yet
- PLC Technician Handbook 2022 EditionFDocument90 pagesPLC Technician Handbook 2022 EditionFpegadashankarNo ratings yet
- Wastewater Flow & Preliminary Treatment of Wastewater (Chapter 6)Document2 pagesWastewater Flow & Preliminary Treatment of Wastewater (Chapter 6)Kimberly Shawn Nicole SantosNo ratings yet
- CH18 Oxidation-Reduction ReactionsDocument2 pagesCH18 Oxidation-Reduction ReactionsCarlos Mella-RijoNo ratings yet
- Provided by Research Papers in EconomicsDocument46 pagesProvided by Research Papers in Economicssojogil742No ratings yet
- Ultimate Guide To Summer by Rochester MagazineDocument32 pagesUltimate Guide To Summer by Rochester MagazinePostBulltinDocsNo ratings yet
- MSDS - Stanbio TrigliseridaDocument4 pagesMSDS - Stanbio TrigliseridaDoni Eka Prasetiyo100% (1)
- Manual de Operação e Manutenção SY500HDocument364 pagesManual de Operação e Manutenção SY500HArthur DangeloNo ratings yet
- 10 1 1 866 5972 PDFDocument15 pages10 1 1 866 5972 PDFLinh NguyenNo ratings yet