UROLOGY
UROLOGY
Download as docx, pdf, or txt
You might also like
- Mcqs in UrologyDocument501 pagesMcqs in UrologyMuhammad AbdulWahidKarim Musafir100% (1)
- 01 Hartmann Global Physical Climatology 2nd - Ed Páginas 7 29Document23 pages01 Hartmann Global Physical Climatology 2nd - Ed Páginas 7 29ElizabethCastañedaHernandez100% (2)
- MCQs For The FRCS (Urol) and Postgraduate Urology ExaminationsDocument241 pagesMCQs For The FRCS (Urol) and Postgraduate Urology ExaminationsHaryo Prakoso Adhi P100% (1)
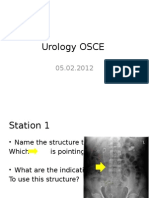
- Urology OSCEDocument9 pagesUrology OSCEJihad Anad83% (6)
- Chap 1 Frcs UrologyDocument39 pagesChap 1 Frcs Urologydr.nm.nsariNo ratings yet
- Urology MCQs For Posgraduate Exam PDFDocument62 pagesUrology MCQs For Posgraduate Exam PDFsiddavaram srideep100% (4)
- Saralea E. Chazan-Profiles of Play - Assessing and Observing Structure and Process in Play Therapy (2002) PDFDocument226 pagesSaralea E. Chazan-Profiles of Play - Assessing and Observing Structure and Process in Play Therapy (2002) PDFALTERINDONESIA100% (4)
- Viva Practice The FRCS (Urol) and Postgraduate Urology Examinations 2018Document79 pagesViva Practice The FRCS (Urol) and Postgraduate Urology Examinations 2018Sufi KhanNo ratings yet
- UROLOGY OSCE Skills English NT Version 2Document1 pageUROLOGY OSCE Skills English NT Version 2HardiTariqHammaNo ratings yet
- General Chemistry 1 Activity Sheet Quarter 2 - MELC 5 Week 3Document11 pagesGeneral Chemistry 1 Activity Sheet Quarter 2 - MELC 5 Week 3Melyn Kaye LedesmaNo ratings yet
- Blandy's UrologyFrom EverandBlandy's UrologyOmar M. AboumarzoukNo ratings yet
- Urology Essay QuestionsDocument2 pagesUrology Essay QuestionsPeter Abikoye100% (1)
- Urology Complete Qbank PDFDocument58 pagesUrology Complete Qbank PDFPanda Panda100% (1)
- Answer For Urology MCQDocument1 pageAnswer For Urology MCQJihad AnadNo ratings yet
- Cambridge Urology MCQDocument37 pagesCambridge Urology MCQManju86% (14)
- Meta Medicine Free EbookDocument37 pagesMeta Medicine Free Ebookgregmeanwell1791100% (13)
- The PESTLE and SWOT AnalysisDocument13 pagesThe PESTLE and SWOT Analysiskoko lambNo ratings yet
- Urology Quiz PDFDocument7 pagesUrology Quiz PDFParsaant Singh100% (1)
- Urology 2Document57 pagesUrology 2Ostaz100% (1)
- Urology OSCEDocument10 pagesUrology OSCEHardiTariqHammaNo ratings yet
- Urology DNB Old QuestionsDocument8 pagesUrology DNB Old QuestionssjulurisNo ratings yet
- 23 TransplantationDocument15 pages23 TransplantationHaseeb IslamNo ratings yet
- 40 Qs Uro AnsweredDocument6 pages40 Qs Uro AnsweredDr-Sulaiman Bani Abdel-rahmanNo ratings yet
- Urology Quiz 10 MCQ AnswerDocument2 pagesUrology Quiz 10 MCQ Answeruroquiz50% (4)
- Urology Grey ManualDocument115 pagesUrology Grey ManualdmshossainNo ratings yet
- UrologyDocument5 pagesUrologynice videosNo ratings yet
- UrologyQuiz6FollowupMCQ and AnswersDocument2 pagesUrologyQuiz6FollowupMCQ and AnswersUrologyQuiz83% (6)
- Urology Sample MCQ Exam eDocument5 pagesUrology Sample MCQ Exam eDALIA100% (2)
- 017 UrologyDocument544 pages017 UrologyNashaat H. Alshawabkeh100% (2)
- UrologyDocument35 pagesUrologymiansk100% (1)
- Urology Slides: DR - JihadDocument4 pagesUrology Slides: DR - JihadJihad Anad100% (1)
- Urology OralDocument2 pagesUrology OralCorina TeteleaNo ratings yet
- Investigations in UrologyDocument19 pagesInvestigations in UrologyMohammed AadeelNo ratings yet
- Genito-Urinary Tract 37Document6 pagesGenito-Urinary Tract 37Hasan A AsFourNo ratings yet
- Urology Quiz 9 MCQ AnswerDocument2 pagesUrology Quiz 9 MCQ Answeruroquiz67% (3)
- MCQ AtaglanceDocument34 pagesMCQ AtaglanceSaied Galal67% (3)
- Lecture Notes Urology Pages 271 277Document7 pagesLecture Notes Urology Pages 271 277Beso Davitashvili0% (1)
- MCQ Uro1Document1 pageMCQ Uro1Kamal El-Ghorory67% (3)
- 400L 2021 UROLOGY MCQsDocument5 pages400L 2021 UROLOGY MCQsApata OmotolaNo ratings yet
- Exam Osce 3Document37 pagesExam Osce 3momo100% (1)
- UntitledDocument56 pagesUntitledmoges beletachaw100% (2)
- Medical Facts and Mcq's Urology MCQDocument14 pagesMedical Facts and Mcq's Urology MCQSmart Urosurgeon100% (2)
- UrologyQuiz8FollowupMCQ and AnswersDocument2 pagesUrologyQuiz8FollowupMCQ and Answersuroquiz100% (2)
- UrologyQuiz2 FollowupMCQ and AnswersDocument1 pageUrologyQuiz2 FollowupMCQ and AnswersUrologyQuizNo ratings yet
- TOPIC NAME-GP Urology MCQsDocument9 pagesTOPIC NAME-GP Urology MCQsAsif Newaz100% (2)
- MCQDocument24 pagesMCQHUSAMNo ratings yet
- Nims MCQ PaperDocument42 pagesNims MCQ PaperShankar Deshmukh67% (3)
- Uro-Final MCQDocument45 pagesUro-Final MCQع كيف كيفك Dhaif-saeedNo ratings yet
- Aua 2012 PDFDocument39 pagesAua 2012 PDFMohsen100% (1)
- Radiology in UrologyDocument39 pagesRadiology in UrologyUgan SinghNo ratings yet
- NEET-SS UrologyDocument59 pagesNEET-SS Urologyadi100% (1)
- 17 Urological InfectionsDocument18 pages17 Urological InfectionsntadudulNo ratings yet
- UrologyDocument8 pagesUrologyAbd Alrahman Hebi100% (1)
- Urology MCQDocument16 pagesUrology MCQChristian Jara83% (6)
- Latihan Soal MCQ UrologiDocument43 pagesLatihan Soal MCQ Urologidytul100% (1)
- Bladder Cancer 7Document44 pagesBladder Cancer 7Awais Ayub100% (1)
- Urology DossierDocument166 pagesUrology DossierPeter100% (1)
- CMC Urology Master - 2019Document240 pagesCMC Urology Master - 2019Sheshang Kamath100% (2)
- Urology Final Exam 2020-2021Document13 pagesUrology Final Exam 2020-2021nice videosNo ratings yet
- UrologyDocument13 pagesUrologyrikasusanti101001201100% (1)
- All ExamsDocument679 pagesAll ExamsYasir Saani100% (2)
- Answered Surgery Department Mcqs Specialities Esp DR NotesDocument70 pagesAnswered Surgery Department Mcqs Specialities Esp DR Notesعبد الله عبداللهNo ratings yet
- TRAUMADocument7 pagesTRAUMAgan choon huiNo ratings yet
- BREASTDocument17 pagesBREASTgan choon huiNo ratings yet
- Attom TrialDocument2 pagesAttom Trialgan choon huiNo ratings yet
- Atlas TrialDocument12 pagesAtlas Trialgan choon huiNo ratings yet
- Complications During Labor and DeliveryDocument27 pagesComplications During Labor and DeliveryMA. JYRELL BONITONo ratings yet
- Behavioral Management TheoryDocument25 pagesBehavioral Management TheoryGilbey Clark Libres100% (1)
- I Belong To A Kindergarten Class.: Daily Lesson PlanDocument10 pagesI Belong To A Kindergarten Class.: Daily Lesson PlanmikeNo ratings yet
- Sedimentation Technique Foreyt 2005 For Quantitative Diagnosis of Fasciolahepatica EggsDocument4 pagesSedimentation Technique Foreyt 2005 For Quantitative Diagnosis of Fasciolahepatica EggsarshadjewanNo ratings yet
- Chapter 9 Privacy, Security, and EthicsDocument21 pagesChapter 9 Privacy, Security, and EthicstayyabashahhxNo ratings yet
- Tobias Hübinette & Catrin Lundström - Sweden After The Recent ElectionDocument12 pagesTobias Hübinette & Catrin Lundström - Sweden After The Recent ElectionPashaAliNo ratings yet
- Project Finance PolicyDocument2 pagesProject Finance PolicyGarcia PangouNo ratings yet
- DCAS Proposal For The UNECE's 192nd SessionDocument79 pagesDCAS Proposal For The UNECE's 192nd SessionMaria MeranoNo ratings yet
- SAP - Create A New Material ArtDocument2 pagesSAP - Create A New Material Artedmondo77No ratings yet
- Iso 12151-3Document1 pageIso 12151-3AkmalNo ratings yet
- RhabdomyosarcomaDocument12 pagesRhabdomyosarcomaAnonymous 8QktfX9sZ6No ratings yet
- Arts10 q4 Week4 v2Document12 pagesArts10 q4 Week4 v2Ryan Dave GarciaNo ratings yet
- PERT Complete ExersicesDocument18 pagesPERT Complete ExersicesUmair MansoorNo ratings yet
- Periods of Indian Art: Lesson 1Document28 pagesPeriods of Indian Art: Lesson 1Christal Dela CruzNo ratings yet
- CPAR 12 Module 1 Quarter 2Document2 pagesCPAR 12 Module 1 Quarter 2vaynediesel7No ratings yet
- CIGRE+IEEE+Tutorial+2012+part+4+HSGS+DS+ES Kosakada For CIGREwebpage PDFDocument59 pagesCIGRE+IEEE+Tutorial+2012+part+4+HSGS+DS+ES Kosakada For CIGREwebpage PDFmorrissubhashNo ratings yet
- Cambridge International AS Level: 8021/22 English General PaperDocument8 pagesCambridge International AS Level: 8021/22 English General PaperNikhil JainNo ratings yet
- Mobility Aids Vehicles BizHouse - UkDocument3 pagesMobility Aids Vehicles BizHouse - UkAlex BekeNo ratings yet
- Changeling Infusion & Tale Craft CardsDocument6 pagesChangeling Infusion & Tale Craft CardsCharles PimentelNo ratings yet
- Web of LiesDocument140 pagesWeb of Liesmamacita puercoNo ratings yet
- Coaching: An International Journal of Theory, Research and PracticeDocument5 pagesCoaching: An International Journal of Theory, Research and PracticeDonatoNo ratings yet
- SOAL Dan KJ TRYOUT PPG 2024Document14 pagesSOAL Dan KJ TRYOUT PPG 2024agamadiguna78No ratings yet
- Dell EMC PowerStore - Data Reduction Efficiency - Dell USDocument3 pagesDell EMC PowerStore - Data Reduction Efficiency - Dell USRa YuthNo ratings yet
- (Michael J. LaRosa, Germán R. Mejía) An Atlas An PDFDocument182 pages(Michael J. LaRosa, Germán R. Mejía) An Atlas An PDFFederNo ratings yet
- SAS University Edition: ® Free Software To Expand or Advance Your Career With High-Demand Analytical SkillsDocument4 pagesSAS University Edition: ® Free Software To Expand or Advance Your Career With High-Demand Analytical SkillsTim AlvaranNo ratings yet