
Out 10
Uploaded by
hikmat pramajatiOut 10
Uploaded by
hikmat pramajatiKnowledge Levels and Training Needs of Disaster
Medicine among Health Professionals, Medical Students,
and Local Residents in Shanghai, China
Tong Su1., Xue Han2., Fei Chen1., Yan Du1., Hongwei Zhang1, Jianhua Yin1, Xiaojie Tan1,
Wenjun Chang1, Yibo Ding1, Yifang Han1, Guangwen Cao1*
1 Department of Epidemiology, Second Military Medical University, Shanghai, China, 2 Department of Chronic Diseases, Center for Disease Control and Prevention of
Yangpu District, Shanghai, China
Abstract
Background: Disaster is a serious public health issue. Health professionals and community residents are main players in
disaster responses but their knowledge levels of disaster medicine are not readily available. This study aimed to evaluate
knowledge levels and training needs of disaster medicine among potential disaster responders and presented a necessity to
popularize disaster medicine education.
Methods: A self-reporting questionnaire survey on knowledge level and training needs of disaster medicine was conducted
in Shanghai, China, in 2012. A total of randomly selected 547 health professionals, 456 medical students, and 1,526 local
residents provided intact information. The total response rate was 93.7%.
Results: Overall, 1.3% of these participants have received systematic disaster medicine training. News media (87.1%) was the
most common channel to acquire disaster medicine knowledge. Although health professionals were more knowledgeable
than community residents, their knowledge structure of disaster medicine was not intact. Medical teachers were more
knowledgeable than medical practitioners and health administrators (p = 0.002). Clinicians performed better than public
health physicians (p,0.001), whereas public health students performed better than clinical medical students (p,0.001). In
community residents, education background significantly affected the knowledge level on disaster medicine (p,0.001).
Training needs of disaster medicine were generally high among the surveyed. ‘Lecture’ and ‘practical training’ were preferred
teaching methods. The selected key and interested contents on disaster medicine training were similar between health
professionals and medical students, while the priorities chosen by local residents were quite different from health
professionals and medical students (p,0.001).
Conclusions: Traditional clinical-oriented medical education might lead to a huge gap between the knowledge level on
disaster medicine and the current needs of disaster preparedness. Continuing medical education and public education
plans on disaster medicine via media should be practice-oriented, and selectively applied to different populations and take
the knowledge levels and training needs into consideration.
Citation: Su T, Han X, Chen F, Du Y, Zhang H, et al. (2013) Knowledge Levels and Training Needs of Disaster Medicine among Health Professionals, Medical
Students, and Local Residents in Shanghai, China. PLoS ONE 8(6): e67041. doi:10.1371/journal.pone.0067041
Editor: Edgardo Szyld, Icahn School of Medicine at Mount Sinai, United States of America
Received January 27, 2013; Accepted May 14, 2013; Published June 24, 2013
Copyright: ß 2013 Su et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was supported by the Education Research Foundation of Shanghai, China (No. A1016 to GC). The funder had no role in study design, data
collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: gcao@smmu.edu.cn
. These authors contributed equally to this work.
Introduction health professionals from on-call health agencies such as military
medical systems and Centers for Disease Control and Prevention
Over the past decade, the intensity and frequency of natural and (CDC) [6]. Hence, community residents and health professionals
man-made disasters have been noticeably increasing all over the as the key components of first responders should be sufficiently
world. Hurricane, earthquake, flood, outbreaks of infectious trained to perform timely and effective medical rescue [7]. Disaster
diseases, nuclear leakage, oil spills, and other disasters in recent medicine training, an integrated part of efficient disaster
years have caused huge economic losses, serious environmental preparedness, is vital for community residents to perform timely
disruption and lasting psychological impairment to the survivors self-rescue and mutual-aid and also for health professionals to
[1–5]. Community residents are the very ones directly affected by develop comprehensive skills [8]. Since the ‘9.119 terrorist attack,
disasters. Therefore, self-rescue and mutual-aid are essential to
many countries have put emphasis on disaster medicine training
form the first defense line. Disaster relief and assistance are mainly
and have sponsored various researches focusing on a wide range of
carried out by medical rescue teams, which are constituted of
PLOS ONE | www.plosone.org 1 June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
disaster medicine, including description and assessment of the among the investigators and three rounds of discussion with
current disaster medicine training programs in order to improve external experts, final version of the questionnaire was made of
the efficiency of disaster rescue. However, these researches on three sections. The first section included demographic information
disaster medicine have mainly been conducted in developed such as age, gender, educational level, medical profession, and
countries, while data from developing countries are scarce [9–14]. disaster rescue experience. The second section contained 16
From a global perspective, disaster frequently attacks developing multiple-choice questions (Q1–Q16) as a knowledge test covering
countries with weak public health infrastructure and often results various aspects of disaster medicine. In this section, participants
in severe consequences. In China, the severe acute respiratory could get one score for each correctly answered question and zero
syndrome (SARS) in 2002–2003 resulted in 5,327 cases and 343 for an incorrect answer. The full score was 16. The third section
deaths [15]. The devastating earthquake in Sichuan, China, in had 5 multiple-choice questions regarding the training needs of
2008 caused more than 69,000 deaths, 18,341 missing and disaster medicine. The first questionnaire is presented as
374,176 wounded persons [16]. However, disaster medicine has Questionnaire S1.
not been included either in the undergraduate curriculum of Based on this questionnaire, we designed the second question-
medical schools or in the continuing medical education in China. naire for community residents (Questionnaire S2). The second
In the past decades, Chinese medical education system has questionnaire had 11 multiple-choice questions (q1–q11) as a
experienced flexuous reforms [17–19]. Traditional medical knowledge test. Eight questions were included in both question-
education and assessment criteria have been largely clinically naires due to their importance in disaster medicine (Table S1).
oriented, while disaster medicine has been long neglected [20]. Before each survey, trained research assistants would give
Recently, efforts have been made to implement disaster medicine detailed instructions. The participants were then asked to finish
education in China. The current program of disaster medicine the questionnaire independently.
education focuses on developing particular small scale training
programs, such as short-term training course of disaster nursing for Ethics Statement
undergraduates, psychosocial training program for mental health Informed consent was initially distributed to every candidate
workers, and emergency preparedness training program for public study subjects to help them make a fully voluntary decision on
health staff [21–24]. However, current knowledge status and participating or declining. Participants who provided their written
training needs of main players on disaster medicine were informed consent were included in this study. The study protocol
unknown. To the best of our knowledge, only one study surveyed conformed to the 1975 Declaration of Helsinki and was approved
the disaster medicine education needs of health professionals who by the ethics committee of Second Military Medical University.
participated in the earthquake rescue, but their related knowledge
was not evaluated [20]. Statistical Analysis
In this study, we evaluated the knowledge levels and training Descriptive statistics were conducted for demographic charac-
needs in populations that are most likely to be involved in disaster teristics. Differences in categorical variables were determined using
rescue. These data are essential in developing proper medical the Chi-square test. Analysis of variance (ANOVA) was used to
training programs of disaster medicine. compare the total scores on average among different participants.
Student-Newman-Keuls (SNK) test was used to correct for
Methods multiple comparisons. Multivariate linear regression was used to
analyze the factors contributing independently to the knowledge
Participants score. A beta coefficient was calculated to indicate the effect of
Three groups of participants in Shanghai, China, were enrolled each independent variable on the score. All tests were two-sided
in this cross-sectional epidemiological study: health professionals, and conducted using SPSS Version 16.0 (SPSS, Chicago, IL). A p
medical students, and community residents. A stratified cluster value of ,0.05 was defined as statistically significant.
random sampling strategy was used to select health professionals
and medical students. A total of 600 health professionals were
Results
composed of medical practitioners, medical teachers, and health
administrators. The medical practitioners were clinicians, public Demographic Characteristics of the Study Participants
health physicians, nurses, and medical technicians from two A total of 547 (91.2%) health professionals, 456 (91.2%) medical
comprehensive tertiary hospitals and three CDCs. The medical students, and 1,526 (95.4%) community residents provided
teachers and 500 medical students were selected from 2 medical complete information. Of the 2,529 participants, 1,315 (52.0%)
schools. Health administrators were from the Municipal Health were men and 2,093 (82.8%) were younger than 50 years. Table 1
Bureau and District Health Bureaus. A multi-stage sampling shows the demographic characteristics. Most of the health
method was used to select 1,600 community residents. We first professionals had a bachelor’s degree or higher in contrast to
randomly selected 5 communities in the Yangpu District. In each community residents (74.6% vs. 23.4%). Health professionals were
community, we randomly selected 27, 80, 65, 58, 58 and 32 composed of 380 (69.5%) medical practitioners, 65 (11.9%)
residents (320 residents per community) at the age of ,20 years, medical teachers, and 102 (18.6%) health administrators. Of the
20–30 years, 30–40 years, 40–50 years, 50–60 years and .60 380 medical practitioners, 147 were clinicians, 134 were public
years, respectively, according to the 2010 census data of age health physicians, 77 were nurses and the remaining 22 were
composition in Shanghai. medical technicians. The professional titles of health professionals
were research assistant (14.0%), senior research assistant (45.3%),
Questionnaire and Epidemiological Survey assistant professor (33.1%), associate professor (5.1%), and full
A structured questionnaire for health professionals/medical professor (1.8%). Of medical students, 236 (62.7%) majored in
students was designed by three investigators (TS, HZ, and GC) clinical medicine and 170 (37.3%) majored in public health.
based on the university examination data bank of emergency Among community residents, 52.0% had no stable employment or
medicine, preventive medicine, and health management, as well as retired. Of all participants, 197 (7.8%) had disaster relief
published literatures [11,20]. After two rounds of discussion experience and 33 (1.3%) had ever received systematic training
PLOS ONE | www.plosone.org 2 June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
Table 1. Demographic characteristics of study participants (N = 2,529).
Health professionals Medical students Community residents
Characteristics n % n % n %
Total 547 100 456 100 1,526 100
Gender
Male 203 37.1 395 86.6 717 47.0
Female 344 62.9 61 13.4 809 53.0
Age (years)
,30 250 45.7 456 100 544 35.6
30,50 257 47.0 – – 586 38.4
.50 40 7.3 – – 396 26.0
Educational level
Junior college or lower 139 25.4 – – 1,169 76.6
Bachelor 182 33.3 407 89.3 326 21.4
Master 163 29.8 43 9.4 31 2.0
Doctorate or oversea training 63 11.5 6 1.3 – –
Profession
Medical practitioner 380 69.5 286* 62.7
Medical teacher 65 11.9 – –
Health administrator 102 18.6 170** 37.3
Employee – – – – 446 29.2
civil servant or teacher – – – – 286 18.7
Others – – – – 794 52.0
Disaster relief experience
Ever 47 8.6 24 5.3 126 8.3
Never 500 91.4 432 94.7 1,400 91.7
Systematic training of disaster medicine
Ever 25 4.6 9 2.0 – –
Never 522 95.4 447 98.0 – –
Self-estimation of disaster medicine knowledge
Well 31 5.7 6 1.3 290 19.0
Moderate 344 62.9 252 55.3 1,069 70.1
Little 172 31.4 198 43.4 167 10.9
Channels of acquiring information about disaster
medicine#
Newspaper/magazine/Internet 172 31.4 89 19.5 847 55.5
TV/radio 144 26.3 95 20.8 422 27.7
Lecture/seminar 121 22.1 60 13.2 227 14.9
School education 79 14.4 70 15.4 84 5.5
Communication with others 50 9.1 58 12.7 307 20.1
*Students that major in clinical medicine,
**Students that major in public health management.
#
One or more answers were allowed.
doi:10.1371/journal.pone.0067041.t001
of disaster medicine. For all 2,529 participants, most of them questions were correctly answered by .50% of the professionals
(87.1%) had low or moderate self-estimated knowledge concerning and students except Q14, Q15, and Q16. Average total score of
disaster medicine, and media (newspaper, magazine, internet, and the knowledge test was 11.00 (95% CI = 10.80–11.21) for health
TV/radio) was the most common channel to acquire knowledge professionals and 11.07 (10.86–11.27) for medical students
on disaster medicine. (p = 0.661) (Figure 1A). Although the score of the two populations
was not significantly different, there were significant differences in
Knowledge Levels correctly answering individual questions: Q3, Q4, Q9, Q12, and
Table 2 depicts the correct answer rates to the 16 questions Q13 (Figure 2A).
(Q1–Q16) in the knowledge test using the first questionnaire. The
PLOS ONE | www.plosone.org 3 June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
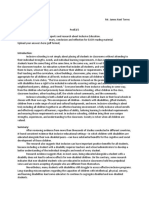
Figure 1. Comparison of the total score on average of disaster medicine knowledge test. A. Health professionals and medical students: no
significant difference (p = 0.661); B. Three groups of health professionals: total score on average of medical teachers was significantly higher than that
of medical practitioners (p = 0.010) and health administrators (p = 0.001); C. Medical students of two majors: total score on average of public health
students was significantly higher than clinical medicine students (p,0.001). D. Community residents of different educational levels: total score on
average of those with high education background was significantly higher than those without (p,0.001).
doi:10.1371/journal.pone.0067041.g001
In health professionals, the score was 10.97 (10.73–11.21), 11.89 in public health students (11.54, 95% CI = 11.28–11.80) was
(11.33–12.45), and 10.57 (10.10–11.04) for medical practitioners, higher than that in clinical medicine students (10.79, 10.51–11.07)
medical teachers, and health administrators, respectively (p,0.001) (Figure 1C). The rates of correctly answering 8
(p = 0.002 for the comparison of three groups) (Figure 1B). For questions (Q3, Q4, Q5, Q6, Q7, Q8, Q13, and Q15) were
pairwise comparison, SNK test showed that medical teachers’ significantly different between the students of 2 majors (p,0.05)
average score was significantly higher than medical practitioners’ (Table 2).
(p = 0.010) and health administrators’ (p = 0.001), while there was Table 3 shows the rate of right responses to the 11 questions
no statistically significant difference between medical practitioners (q1–q11) in community residents. The questions were correctly
and health administrators (p.0.05). The rates of correctly answered by .50% of community residents except q4 and q5.
answering 9 questions (Q2, Q4, Q5, Q9, Q10, Q11, Q12, Q13, After stratified by educational level, the score of well-educated
and Q16) were significantly different among medical practitioners, (bachelor or higher) group (7.42, 7.20–7.65) was significantly
medical teachers, and health administrators (p,0.05) (Table 2). higher than that of poor-educated (junior college or lower) group
For example, in answering Q5, medical teachers did better than (6.91, 6.80–7.03) (p,0.001) (Figure 1D). The rates of correct
medical practitioners (p = 0.004) and health administrators answers to 7 questions (q2, q4, q5, q7, q8, q9, and q10) were
(p,0.001). Moreover, the knowledge level was also significantly significantly different between the two groups (p,0.05).
different among clinicians, public health physicians, nurses, and We compared the rates of correctly answering the 8 common
medical technicians, especially in correctly answering 5 questions questions in both questionnaires (Table S1) between health
(Table S2). Clinicians performed better than public health professionals and community residents. The rates were generally
physicians (p,0.001) (Figure S1). In medical students, the score
PLOS ONE | www.plosone.org 4 June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
Figure 2. The rates of correctly answering the key questions concerning disaster medicine between different populations. A. Health
professionals vs. medical students: p,0.05 for Q3 ‘self-rescue measures in an earthquake’, Q4 ‘triage and treatment priority’, Q9 ‘concept of first aid ABC’,
Q12 ‘tourniquet hemostasis’, and Q13 ‘skills of psychological assistance in post-disaster relief’; B. Health professionals vs. community residents: p,0.001
for q4 ‘Cardiopulmonary resuscitation procedure’, q5 ‘Difference between remote and urban rescue’, q8 ‘Self-rescue measures in an earthquake’, q9
‘Location of temporary toilets during disaster rescue’, q10 ‘Skills of psychological assistance in post-disaster relief’, and q11 ‘Epidemic prevention strategies
after a disaster’ and p,0.05 for q6 ‘Fracture fixation and transport’ and q7 ‘Self-rescue measures in a high-rise fire’.
doi:10.1371/journal.pone.0067041.g002
lower in community residents than in health professionals (57.8% (b = 20.193, p,0.001), in health professionals. Educational level
vs. 72.4%) except q5 (Figure 2B). was the unique factor significantly associated with an increased
Multivariate linear regression analysis indicated that education- score in community residents (b = 0.214, p = 0.001). Public health
al level (b = 0.204, p,0.001) and professional title (b = 0.142, major was the factor significantly associated with an increased
p = 0.008) were significantly associated with an increased knowl- score in medical students (b = 0.661, p = 0.002).
edge score, whereas age was inversely related to the score
PLOS ONE | www.plosone.org 5 June 2013 | Volume 8 | Issue 6 | e67041
Table 2. Number (%) of health professionals and medical students correctly answering the 16 questions in knowledge test section.
Health professionals Medical students
Clinical
Disaster Medicine-related Medical Medical medicine Public health
Questions Total practitioners teachers Health administrators p value Total students students p value
Q1 Concept of on-site treatment 523 (95.6) 364 (95.8) 64 (98.5) 95 (93.1) 0.250 431 (94.5) 267 (93.4) 164 (96.5) 0.158
PLOS ONE | www.plosone.org
Q2 Self-rescue measures in a high-rise fire 509 (93.1) 352 (92.6) 65 (100.0) 92 (90.2) 0.044 432 (94.7) 268 (93.7) 164 (96.5) 0.201
Q3 Self-rescue measures in an earthquake 476 (87.0) 334 (87.9) 59 (90.8) 83 (81.4) 0.139 374 (82.0) 222 (77.6) 152 (89.4) 0.002
Q4 Triage and treatment priority 461 (84.3) 311 (81.8) 60 (92.3) 90 (88.2) 0.048 411 (90.1) 251 (87.8) 160 (94.1) 0.028
Q5 Medical evacuation after an earthquake 414 (75.7) 290 (76.3) 60 (92.3) 64 (62.7) ,0.001 355 (77.9) 207 (72.4) 148 (87.1) ,0.001
Q6 Concept of disaster preparedness 447 (81.7) 303 (79.7) 59 (90.8) 85 (83.3) 0.093 392 (86.0) 237 (82.9) 155 (91.2) 0.014
Q7 Epidemic prevention strategies after a 444 (81.2) 305 (80.3) 51 (78.5) 88 (86.3) 0.324 379 (83.1) 227 (79.4) 152 (89.4) 0.006
disaster
Q8 Location of temporary toilets during 391 (71.5) 262 (68.9) 51 (78.5) 78 (76.5) 0.136 340 (74.6) 203 (71.0) 137 (80.6) 0.023
disaster rescue
Q9 Concept of first aid ABC (airway, 417 (76.2) 301 (79.2) 51 (78.5) 65 (63.7) 0.004 276 (60.5) 168 (58.7) 108 (63.5) 0.312
breathing and circulation)
Q10 Fracture fixation and transport 399 (72.9) 278 (73.2) 38 (58.5) 83 (81.4) 0.005 324 (71.1) 205 (71.7) 119 (70.0) 0.702
Q11 Cardiopulmonary resuscitation 388 (70.9) 283 (74.5) 49 (75.4) 56 (54.9) ,0.001 334 (73.2) 204 (71.3) 130 (76.5) 0.230
6
procedure
Q12 Tourniquet hemostasis 312 (57.0) 208 (54.7) 47 (72.3) 57 (55.9) 0.029 343 (75.2) 217 (75.9) 126 (74.1) 0.674
Q13 Skills of psychological assistance in post-391 (71.5) 265 (69.7) 55 (84.6) 71 (69.6) 0.044 277 (60.7) 157 (54.9) 120 (70.6) 0.001
disaster relief
Q14 Diagnosis of post-traumatic stress 201 (36.7) 141 (37.1) 29 (44.6) 31 (30.4) 0.172 163 (35.7) 104 (36.4) 59 (34.7) 0.721
disorder (PTSD)
Q15 Difference between remote area and 169 (30.9) 122 (32.1) 18 (27.7) 29 (28.4) 0.650 132 (28.9) 94 (32.9) 38 (22.4) 0.017
urban rescue
Q16 Population vulnerability assessment 77 (14.1) 49 (12.9) 17 (26.2) 11 (10.8) 0.010 84 (18.4) 55 (19.2) 29 (17.1) 0.563
doi:10.1371/journal.pone.0067041.t002
June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
Knowledge and Training Needs of Disaster Medicine
Table 3. Number (%) of community residents correctly answering the 11 questions in knowledge test section.
High educated Low educated
Disaster Medicine-related Questions Total, N = 1,526 residents, N = 357 residents, N = 1,169 p value
q1 Emergency call numbers 1,447 (94.8) 345 (96.6) 1,102 (94.3) 0.077
q2 Position of exit passageway 862 (56.5) 229 (64.1) 633 (54.1) 0.001
q3 Self-rescue measures in a nuclear leak 1373 (90.0) 315 (88.2) 1,058 (90.5) 0.211
q4 Cardiopulmonary resuscitation procedure 563 (36.9) 107 (30.0) 456 (39.0) 0.002
q5 Difference between remote area and urban rescue 645 (42.3) 185 (51.8) 460 (39.3) ,0.001
q6 Fracture fixation and transport 1,031 (67.6) 248 (69.5) 783 (67.0) 0.380
q7 Self-rescue measures in a high-rise fire 1,355 (88.8) 330 (92.4) 1,025 (87.7) 0.013
q8 Self-rescue measures in an earthquake 1,038 (68.0) 272 (76.2) 766 (65.5) ,0.001
q9 Location of temporary toilets during disaster rescue 792 (51.9) 213 (59.7) 579 (49.5) 0.001
q10 Skills of psychological assistance in post-disaster relief 763 (50.0) 203 (56.9) 560 (47.9) 0.003
q11 Epidemic prevention strategies after a disaster 863 (56.6) 203 (56.9) 660 (56.5) 0.893
doi:10.1371/journal.pone.0067041.t003
Training Needs selected ‘basic principles of disaster rescue’ (74.0%), ‘treatment principles
Table 4 depicts the training needs of health professionals and and first-aid skills’ (69.8%), and ‘psychological relief’ (64.4%) as the
medical students. The overall opinions on teaching method, course most interested contents, while community residents selected ‘basic
arrangement, and teaching material were consistent among the principles of disaster rescue’ (47.9%) and specific disaster events such as
two groups. More than half of these participants selected ‘lecture’, ‘earthquakes’ (40.9%) and ‘fire disaster’ (40.8%).
‘practical training’, and ‘disaster movies or videos’ as preferred teaching
methods. Most participants chose ‘required course for public health Discussion
professional’ as the major training course, and preferred using
‘national unified textbook’ as standard teaching material. However, In this study, we evaluated the current knowledge levels and
medical teachers considered that ‘practical training’ and ‘disaster training needs of disaster medicine among health professionals,
movies or videos’ were not appropriate for teaching disaster medicine, medical students, and community residents in Shanghai, China. In
in contrast to medical practitioners and health administrators. general, our results reflected a high vulnerability of our
Most health administrators believed that disaster medicine training populations when facing disaster. The knowledge level of disaster
should be a required training subject not only for public health medicine was not satisfactory in health professionals except
professionals but also for clinicians. medical teachers. Although the majority of the health professionals
Table 5 shows disaster medicine training needs of community received formal medical education, few of them have ever received
residents. The majority (88.5%) selected ‘need to learn disaster systematic training of disaster medicine (Table 1). For health
medicine’ and ‘need of disaster medicine course for children’. About half of professionals and medical students, less accurate responses to Q14,
community residents selected ‘lecture’ and ‘practical training’ as Q15, and Q16 (Table 2) indicate the low levels of knowledge on
preferred teaching methods. More than 70% of community disaster psychology and disaster administration. The two compo-
residents selected ‘willing to participate in disaster simulation drill nents have been long neglected and should be added to disaster
regularly’ and believed that ‘community volunteer team for disaster relief medicine training and specially addressed to these involved in
should be set up and willing to participate volunteer team’. Compared to psychological relief and administrative tasks. Lack of knowledge
community residents with lower educational level, those with regarding PTSD is an issue needs to be particularly addressed.
higher education background considered that ‘systemic study’ was Because of the cultural perception in the Chinese society,
more appropriate for teaching (54.3% vs. 43.6%, p,0.001). psychological health hasn’t been widely accepted as a critical
Figure 3 presents the key contents concerning disaster medicine component in traditional medical and public health education.
training prioritized by health professionals, medical students, and Even though there is a rising awareness of its indispensible
community residents. More than 50% of health professionals and importance in recent years [1], relevant educational program and
medical students selected the contents of ‘first aid skills’, ‘epidemic public health campaign are still lagging behind. In health
prevention and control’, ‘psychological problems in post-disaster relief’, and professionals, the significant differences among different profes-
‘principles of disaster disposal’ as important contents; while most sions (Figure 1) were mainly presented in their answers to the 9
community residents chose ‘first aid skills’ and ‘basic concepts of disaster questions covering 4 aspects: self-help and first-aid skills, triage and
medicine’ as important contents. Significant differences existed evacuation, psychological relief, and population vulnerability
among subgroups within each group of participants. For example, assessment. Health administrators did not show their proficiency
compared to medical practitioners, medical teachers considered in disaster administration and disaster rescue organization, for
that ‘triage and evacuation’ was less important (32.2% vs. 50.8%, they poorly answered the related questions such as Q5. Leadership
p = 0.022) (Table S3). training programs could effectively improve the emergency-
Twenty-five items covering most aspects of disaster medicine handling capability of health administrators who might be
were provided for the selection of interested training contents involved in disaster rescue [25,26]. Moreover, there were
(Table S4). Figure 4 presents the most interested contents of significant differences in knowledge levels among 4 specialties
disaster medicine training prioritized by health professionals, (clinicians, public health physicians, nurses, and medical techni-
medical students, and community residents. Health professionals cians) of medical practitioners. Clinicians showed higher knowl-
PLOS ONE | www.plosone.org 7 June 2013 | Volume 8 | Issue 6 | e67041
Table 4. Training needs of health professionals and medical students (number, %).
Health professionals Medical students
Medical Medical Health Clinical medicine Public health
Training Needs Total practitioners teachers administrators p value Total students students p value
Teaching method
Lecture 431 (78.8) 292 (76.8) 54 (83.1) 85 (83.3) 0.242 294 (64.5) 184 (64.3) 110 (64.7) 0.936
PLOS ONE | www.plosone.org
Practical training 329 (60.1) 240 (63.2) 25 (38.5) 64 (62.7) 0.001 250 (54.8) 139 (48.6) 111 (65.3) 0.001
Disaster movies or videos 304 (55.6) 230 (60.5) 21 (32.3) 53 (52.0) ,0.001 311 (68.2) 202 (70.6) 109 (64.1) 0.149
Systemic study 257 (47.0) 183 (48.2) 30 (46.2) 44 (43.1) 0.659 174 (38.2) 100 (35.0) 74 (43.5) 0.069
Academic report 229 (41.9) 166 (43.7) 28 (43.1) 35 (34.3) 0.229 110 (24.1) 67 (23.4) 43 (25.3) 0.652
Course arrangement
Required course for public health 295 (53.9) 198 (52.1) 36 (55.4) 61 (59.8) 0.371 187 (41.0) 93 (32.5) 94 (55.3) 0.000
professional
Selective course for clinician 206 (37.7) 150 (39.5) 20 (30.8) 36 (35.3) 0.352 181 (39.7) 119 (41.6) 62 (36.5) 0.278
Required course for clinician 183 (33.5) 121 (31.8) 15 (23.1) 47 (46.1) 0.004 108 (23.7) 67 (23.4) 41 (24.1) 0.867
Selective course for public health 160 (29.3) 126 (33.2) 11 (16.9) 23 (22.5) 0.007 103 (22.6) 56 (19.6) 47 (27.6) 0.046
professional
Informal course 102 (18.6) 71 (18.7) 18 (27.7) 13 (12.7) 0.054 110 (24.1) 75 (26.2) 35 (20.6) 0.174
8
Teaching materials
National unified textbook 421 (77.0) 292 (76.8) 43 (66.2) 86 (84.3) 0.025 209 (45.8) 132 (46.2) 77 (45.3) 0.859
Foreign teaching materials 145 (26.5) 99 (26.1) 19 (29.2) 27 (26.5) 0.866 150 (32.9) 95 (33.2) 55 (32.4) 0.849
Military teaching materials 131 (23.9) 86 (22.6) 21 (32.3) 24 (23.5) 0.239 156 (34.2) 92 (32.2) 64 (37.6) 0.233
Handouts for internal use 73 (13.3) 59 (15.5) 7 (10.8) 7 (6.9) 0.060 100 (21.9) 60 (21.0) 40 (23.5) 0.524
Other 22 (4.0) 14 (3.7) 4 (6.2) 4 (3.9) 0.644 14 (3.1) 8 (2.8) 6 (3.5) 0.661
doi:10.1371/journal.pone.0067041.t004
June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
Knowledge and Training Needs of Disaster Medicine
Table 5. Training needs of community residents and their differences between the 2 educational level groups (number, %).
Training Needs Total, N = 1,526 High-educated, N = 357 Low-educated, N = 1,169 p value
Need to learn disaster medicine
Yes 1,350 (88.5) 329 (92.2) 1,021 (87.3) 0.013
No or does not matter 176 (11.5) 28 (7.8) 148 (12.7)
Teaching method
Lecture 1,121 (73.5) 286 (80.1) 835 (71.4) 0.001
Practical training 775 (50.8) 175 (49.0) 600 (51.3) 0.446
Systemic study 704 (46.1) 194 (54.3) 510 (43.6) ,0.001
Disaster movies or videos 661 (43.3) 158 (44.3) 503 (43.0) 0.682
Academic report 152 (10.0) 32 (9.0) 120 (10.3) 0.427
Need of disaster medicine course for children
Yes 1,339 (87.7) 318 (89.1) 1,021 (87.3) 0.211
No 66 (4.3) 18 (5.0) 48 (4.1)
Does not matter 121 (7.9) 21 (5.9) 100 (8.6)
Organize disaster simulation drill in community
Willing to participate regularly 1,073 (70.3) 283 (73.7) 810 (69.3) 0.044
Willing to participate occasionally 309 (20.2) 74 (20.7) 235 (20.1)
Not willing to participate 16 (1.4) 3 (0.8) 19 (1.2)
Does not matter 125 (8.2) 17 (4.8) 108 (9.2)
Community volunteer team for disaster relief
Should be set up, and willing to participate 1,199 (78.6) 304 (85.2) 895 (76.6) 0.002
Should be set up, but not willing to participate 147 (9.6) 23 (6.4) 124 (10.6)
Should not be set up, and not willing to participate 32 (2.1) 9 (2.5) 23 (2.0)
Does not matter 148 (9.7) 21 (5.9) 127 (10.9)
doi:10.1371/journal.pone.0067041.t005
Figure 3. Key contents concerning disaster medicine training prioritized by health professionals, medical students, and community
residents.
doi:10.1371/journal.pone.0067041.g003
PLOS ONE | www.plosone.org 9 June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
Figure 4. Interested contents concerning disaster medicine training prioritized by health professionals, medical students, and
community residents.
doi:10.1371/journal.pone.0067041.g004
edge level than other specialties, even on the aspect of epidemic likely to have frequent access to modern media such as the internet
prevention and control (Table S2 and Figure S1), which is one of and thus gain ‘exposure’ to updated information on disaster
the major tasks of public health physicians. The differences in the medicine.
knowledge level indicate that the medical education in China had Community residents displayed very poor knowledge and skills
been largely clinically oriented; and little attention has been paid of disaster medicine. Not surprisingly, community residents
to public health preparedness, especially disaster preparedness. generally lacked specialty knowledge such as ‘cardiopulmonary
Future training plans should clearly define the roles of public resuscitation procedure’ and ‘difference between remote and urban rescue’
health physicians and health administrators in disaster rescue and (Table 3 and Figure 2B). An important finding is that community
enhance their capabilities to meet up-to-date requirements [27]. residents with higher education background had higher knowledge
The main reason of the lack of disaster medicine knowledge for level of disaster medicine than those without (Figure 1D). Thus, it
health professionals might be that disaster medicine has rarely is urgent to tailor community training programs for the residents
been included in medical school curriculum and continuing with different education background and popularize disaster
medical education, and no appropriate public health programs medicine education via modern media.
focusing on disaster preparedness. Surprisingly, public health This study also pointed out the training needs of disaster
students showed a higher knowledge level than clinical medicine medicine. Most participants selected ‘lecture’ and ‘practical training’ as
students (p,0.001) (Figure 1C). After the SARS outbreak, the preferred teaching methods. Most health professionals and
importance of public health preparedness has been emphasized medical students suggested that disaster medicine should be a
with a curriculum restructure for public health major students. In ‘required course for public health professional’ and asked for a ‘national
addition to the traditional courses such as epidemiology, training unified textbook’ as standardized teaching material. Most community
programs for public health preparedness such as health manage- residents believed ‘need to learn disaster medicine’ and ‘need of disaster
ment has been added as the main courses for public health major medicine course for children’, and selected ‘willing to participate in disaster
in some medical schools. However, disaster medicine is being simulation drill regularly’ and ‘community volunteer team for disaster relief
developed as a training course in only a couple of medical schools should be set up, and willing to participate volunteer team’ (Table 4,
in China. Our results indicate that future public health physicians Table 5). These results indicate that the training needs of disaster
are expected to perform better in disaster rescue. Interestingly, the medicine is very high in Chinese society and disaster medicine
knowledge level of health professionals was inversely related to trainings should be executed as indispensable courses for health
age, which is in contrast to the general belief that older professionals, medical students, and community residents. Mean-
professionals have more experiences and therefore more knowl- while, the three groups of participants selected some different key
edgeable. One possible explanation is that the young are more and interested contents for disaster medicine training (Figure 3 and
PLOS ONE | www.plosone.org 10 June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
Figure 4). This reflects that distinct perception of disaster Supporting Information
determines the different needs of disaster medicine training in
different populations. Similar differences in several items of the Figure S1 Comparisons of the total scores on average
training needs were also presented among the subgroups of study and rates of correctly answering 5 important questions
participants. Training programs such as disaster simulation and among clinicians, public health physicians, nurses, and
disaster exercise have proven to be effective and can rapidly medical technicians. A. Comparison of average scores; B.
deliver core elements of disaster medicine and improve the Comparison of correct answer rates.
knowledge level and ability of disaster response [10,28,29]. (TIF)
Therefore, future continuing disaster medicine education should Figure S2 Suggested diagram of disaster medicine
focus on developing practice-oriented and core elements-high- training (Shanghai model).
lighted training courses. Except the high-level interests in ‘basic (TIF)
principles of disaster relief’, there were some differences of interested
contents among different populations, indicating future training Table S1 List of the same questions in two questionnaires.
program design should consider both core elements and interests, (DOC)
and customize to different needs. As medical teachers were more Table S2 Comparisons of correctly answering the 16 disaster
knowledgeable in disaster medicine than other populations medicine-related questions among 4 specialties of medical
surveyed (Figure 1B), they should play a leading role in disaster practitioners.
medicine training. Based on these data, we suggest a diagram flow (DOC)
of disaster medicine training as the Shanghai model in Figure S2.
The present survey was conducted in Shanghai, one of the areas Table S3 Key contents of disaster medicine training prioritized
with well developed economy and affluent medical resources in by different study populations.
China. After further evaluation, the Shanghai model of disaster (DOC)
medicine training suggested in this study should be validated and
Table S4 Interested contents of disaster medicine training
generalizable to other developing areas where the problem of
prioritized by different study populations.
unmatched economic development and disaster medicine educa-
(DOC)
tion also exist. These data also provide useful evidence to help
developing disaster medicine training plans in other developing Questionnaire S1 Questionnaire for health profession-
world. als and medical students.
The current study had limitations. Our community participants (DOC)
were from one district (Yangpu) in Shanghai chosen by cluster
Questionnaire S2 Questionnaire for community resi-
sampling. Sample sizes may influence results if comparing
dents.
subgroups within clusters. Furthermore, other groups of disaster
(DOC)
first responders such as firefighters and military personnel were not
included in the current survey. Future studies focusing on these
special groups will provide valuable information for disaster Acknowledgments
preparedness. We thank Jian Mei (Municipal Centers for Disease Control and Prevention
In conclusion, this large epidemiological study provided of Shanghai), Hong Wu (Municipal Health Bureau of Shanghai) and
important data concerning knowledge level and training needs Shuhua Li (District Center for Disease Control and Prevention of
among the populations that would be involved in disaster rescue or Hongkou, Shanghai) for their great help in the epidemiological survey.
affected by disasters. From a health education perspective, disaster
training programs are urgently needed, with specific emphasis on Author Contributions
certain contents, such as psychological relief and administrative
Conceived and designed the experiments: GC TS HZ XH. Performed the
skills. Our study enables a more comprehensive evaluation of experiments: TS FC XH Y. Ding JY XT WC YH. Analyzed the data: TS
current disaster preparedness situation and facilitates designing Y. Du HZ. Contributed reagents/materials/analysis tools: TS XH FC Y.
future disaster medicine training programs in China and other Du JY XT WC YH. Wrote the paper: TS Y. Du GC. Obtained permission
developing countries. for the field survey: GC. Obtained funding: GC.
References
1. Zhang Z, Wang W, Shi Z, Wang L, Zhang J (2012) Mental health problems 7. Huntington MK, Gavagan TF (2011) Disaster medicine training in family
among the survivors in the hard-hit areas of the Yushu earthquake. PLoS One 7: medicine: a review of the evidence. Fam Med 43: 13–20.
e46449. 8. Hsu EB, Thomas TL, Bass EB, Whyne D, Kelen GD, et al. (2006) Healthcare
2. Pietrzak RH, Tracy M, Galea S, Kilpatrick DG, Ruggiero KJ, et al. (2012) worker competencies for disaster training. BMC Med Educ 6: 19.
Resilience in the face of disaster: prevalence and longitudinal course of mental 9. Haraoka T, Ojima T, Murata C, Hayasaka S (2012) Factors influencing
disorders following hurricane Ike. PLoS One 7: e38964. collaborative activities between non-professional disaster volunteers and victims
3. Usami M, Iwadare Y, Kodaira M, Watanabe K, Aoki M, et al. (2012) of earthquake disasters. PLoS One 7: e47203.
Relationships between traumatic symptoms and environmental damage 10. Scott LA, Carson DS, Greenwell IB (2010) Disaster 101: a novel approach to
conditions among children 8 months after the 2011 Japan earthquake and disaster medicine training for health professionals. J Emerg Med 39: 220–226.
tsunami. PLoS One 7: e50721. 11. Kaiser HE, Barnett DJ, Hsu EB, Kirsch TD, James JJ, et al. (2009) Perspectives
4. White HK, Hsing PY, Cho W, Shank TM, Cordes EE, et al. (2012) Impact of of future physicians on disaster medicine and public health preparedness:
the deepwater horizon oil spill on a deep-water coral community in the Gulf of challenges of building a capable and sustainable auxiliary medical workforce.
Mexico. Proc Natl Acad Sci U S A 109: 20303–20308. Disaster Med Public Health Prep 3: 210–216.
5. Xu G, Ying Y, Liu Y, Chang W, Ni H, et al. (2012) Incidences, types, and 12. Pfenninger EG, Domres BD, Stahl W, Bauer A, Houser CM, et al. (2010)
influencing factors of snow disaster-associated injuries in Ningbo, China, 2008. Medical student disaster medicine education: the development of an educational
Disaster Med Public Health Prep 6: 363–369. resource. Int J Emerg Med 3: 9–20.
6. You C, Chen X, Yao L (2009) How China responded to the May 2008 13. Kaji AH, Coates W, Fung CC (2010) A disaster medicine curriculum for medical
earthquake during the emergency and rescue period. J Public Health Policy 30: students. Teach Learn Med 22: 116–122.
379–393; discussion 393–374. 14. Delooz H, Debacker M, Moens G, Johannik K (2007) European survey on
training objectives in disaster medicine. Eur J Emerg Med 14: 25–31.
PLOS ONE | www.plosone.org 11 June 2013 | Volume 8 | Issue 6 | e67041
Knowledge and Training Needs of Disaster Medicine
15. Feng D, de Vlas SJ, Fang LQ, Han XN, Zhao WJ, et al. (2009) The SARS 23. Ng C, Ma H, Raphael B, Yu X, Fraser J, et al. (2009) China-Australia training
epidemic in mainland China: bringing together all epidemiological data. Trop on psychosocial crisis intervention: response to the earthquake disaster in
Med Int Health 14 Suppl 1: 4–13. Sichuan. Australas Psychiatry 17: 51–55.
16. Qiu J, Liu GD, Wang SX, Zhang XZ, Zhang L, et al. (2010) Analysis of injuries 24. Wang C, Wei S, Xiang H, Xu Y, Han S, et al. (2008) Evaluating the
and treatment of 3,401 inpatients in 2008 Wenchuan earthquake–based on effectiveness of an emergency preparedness training programme for public
Chinese Trauma Databank. Chin J Traumatol 13: 297–303. health staff in China. Public Health 122: 471–477.
17. Lam TP, Wan XH, Ip MS (2006) Current perspectives on medical education in 25. Wang C, Wei S, Xiang H, Wu J, Xu Y, et al. (2008) Development and
China. Med Educ 40: 940–949. evaluation of a leadership training program for public health emergency
18. Gao T, Shiwaku K, Fukushima T, Isobe A, Yamane Y (1999) Medical education response: results from a Chinese study. BMC Public Health 8: 377.
in China for the 21st century. Med Educ 33: 768–773. 26. Woltring C, Constantine W, Schwarte L (2003) Does leadership training make a
19. Huang J (1992) Medical education and medical education research and difference? The CDC/UC Public Health Leadership Institute: 1991–1999.
development activities in modern China. Med Educ 26: 333–339. J Public Health Manag Pract 9: 103–122.
20. Huang B, Li J, Li Y, Zhang W, Pan F, et al. (2011) Need for continual education 27. Russell ML, McIntyre L (2009) An estimation of Canada’s public health
about disaster medicine for health professionals in China-a pilot study. BMC
physician workforce. Can J Public Health 100: 199–203.
Public Health 11: 89.
28. Summerhill EM, Mathew MC, Stipho S, Artenstein AW, Jagminas L, et al.
21. Chan SS, Chan WS, Cheng Y, Fung OW, Lai TK, et al. (2010) Development
(2008) A simulation-based biodefense and disaster preparedness curriculum for
and evaluation of an undergraduate training course for developing International
internal medicine residents. Med Teach 30: e145–151.
Council of Nurses disaster nursing competencies in China. J Nurs Scholarsh 42:
405–413. 29. Bartley BH, Stella JB, Walsh LD (2006) What a disaster?! Assessing utility of
22. Pang SM, Chan SS, Cheng Y (2009) Pilot training program for developing simulated disaster exercise and educational process for improving hospital
disaster nursing competencies among undergraduate students in China. Nurs preparedness. Prehosp Disaster Med 21: 249–255.
Health Sci 11: 367–373.
PLOS ONE | www.plosone.org 12 June 2013 | Volume 8 | Issue 6 | e67041
© 2013 Su et al. This is an open-access article distributed under the terms of
the Creative Commons Attribution License:
https://creativecommons.org/licenses/by/4.0/ (the “License”), which permits
unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited. Notwithstanding the ProQuest Terms
and Conditions, you may use this content in accordance with the terms of the
License.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good Life4/5 (6124)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You Are4/5 (1148)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On It4.5/5 (933)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space Race4/5 (954)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy Answers4.5/5 (361)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first Century3.5/5 (2283)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New America4.5/5 (278)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True Story3.5/5 (692)
- SHIC EF - Int - 9AB - ListeningAssessment - V4.0No ratings yetSHIC EF - Int - 9AB - ListeningAssessment - V4.03 pages
- Identify The Disaster Nursing Training ANo ratings yetIdentify The Disaster Nursing Training A10 pages
- Training Needs Assessment For Nurses in Sennar State, Sudan: Cross Sectional StudyNo ratings yetTraining Needs Assessment For Nurses in Sennar State, Sudan: Cross Sectional Study12 pages
- Educational Innovations: Lois Magnussen, Edd, AprnNo ratings yetEducational Innovations: Lois Magnussen, Edd, Aprn6 pages
- Towards Community-Based Landslide Preparedness in MalaysiaNo ratings yetTowards Community-Based Landslide Preparedness in Malaysia10 pages
- Hennessy-Hicks Training Needs Analysis Questionnaire and ManualNo ratings yetHennessy-Hicks Training Needs Analysis Questionnaire and Manual59 pages
- Larsen-Freeman On Teaching Methods and Approaches For Teaching English As A Foreign LanguageNo ratings yetLarsen-Freeman On Teaching Methods and Approaches For Teaching English As A Foreign Language15 pages
- Artificial Intelligence: Lab Manual # 06No ratings yetArtificial Intelligence: Lab Manual # 0610 pages
- Lesson 1 - Academic Reading and WritingNo ratings yetLesson 1 - Academic Reading and Writing15 pages
- 1st Quarter Examination Discipline & Ideas in The Social SciencesNo ratings yet1st Quarter Examination Discipline & Ideas in The Social Sciences1 page
- Bending Strength of High-Density Fibreboards (HDF) Manufactured From Wood of Hard Broadleaved SpeciesNo ratings yetBending Strength of High-Density Fibreboards (HDF) Manufactured From Wood of Hard Broadleaved Species14 pages
- Decision Making in Service Industries A Practical Approach 1st Edition Javier Faulin (Editor) - Explore the complete ebook content with the fastest download100% (1)Decision Making in Service Industries A Practical Approach 1st Edition Javier Faulin (Editor) - Explore the complete ebook content with the fastest download56 pages
- Seminar Presentation: Artificial Intelligence (AI)No ratings yetSeminar Presentation: Artificial Intelligence (AI)15 pages
- LABREPORT1 IS216 Ramos Samuya Sison Yadao TumambingNo ratings yetLABREPORT1 IS216 Ramos Samuya Sison Yadao Tumambing6 pages
- Why Facilitating Progress Is Key To Employee Engagement 1687790031No ratings yetWhy Facilitating Progress Is Key To Employee Engagement 168779003127 pages
- Action Plan: Enhance-School Improvement Plan (E-SIP) and School Report (SRC)100% (1)Action Plan: Enhance-School Improvement Plan (E-SIP) and School Report (SRC)2 pages














































































- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good Life
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You Are
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On It
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space Race
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy Answers
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic Future
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of Cancer
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy Living
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first Century
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New America
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True Story
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham Lincoln
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New Deal
- Training Needs Assessment For Nurses in Sennar State, Sudan: Cross Sectional StudyTraining Needs Assessment For Nurses in Sennar State, Sudan: Cross Sectional Study
- Educational Innovations: Lois Magnussen, Edd, AprnEducational Innovations: Lois Magnussen, Edd, Aprn
- Towards Community-Based Landslide Preparedness in MalaysiaTowards Community-Based Landslide Preparedness in Malaysia
- Hennessy-Hicks Training Needs Analysis Questionnaire and ManualHennessy-Hicks Training Needs Analysis Questionnaire and Manual
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New America
- Larsen-Freeman On Teaching Methods and Approaches For Teaching English As A Foreign LanguageLarsen-Freeman On Teaching Methods and Approaches For Teaching English As A Foreign Language
- 1st Quarter Examination Discipline & Ideas in The Social Sciences1st Quarter Examination Discipline & Ideas in The Social Sciences
- Bending Strength of High-Density Fibreboards (HDF) Manufactured From Wood of Hard Broadleaved SpeciesBending Strength of High-Density Fibreboards (HDF) Manufactured From Wood of Hard Broadleaved Species
- Decision Making in Service Industries A Practical Approach 1st Edition Javier Faulin (Editor) - Explore the complete ebook content with the fastest downloadDecision Making in Service Industries A Practical Approach 1st Edition Javier Faulin (Editor) - Explore the complete ebook content with the fastest download
- Seminar Presentation: Artificial Intelligence (AI)Seminar Presentation: Artificial Intelligence (AI)
- LABREPORT1 IS216 Ramos Samuya Sison Yadao TumambingLABREPORT1 IS216 Ramos Samuya Sison Yadao Tumambing
- Why Facilitating Progress Is Key To Employee Engagement 1687790031Why Facilitating Progress Is Key To Employee Engagement 1687790031
- Action Plan: Enhance-School Improvement Plan (E-SIP) and School Report (SRC)Action Plan: Enhance-School Improvement Plan (E-SIP) and School Report (SRC)