
FrmPatientViewAllReport - 2023-04-06T211159.013 PDF
FrmPatientViewAllReport - 2023-04-06T211159.013 PDF
Uploaded by
amir.khann4411Copyright:
Available Formats
FrmPatientViewAllReport - 2023-04-06T211159.013 PDF
FrmPatientViewAllReport - 2023-04-06T211159.013 PDF
Uploaded by
amir.khann4411Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
FrmPatientViewAllReport - 2023-04-06T211159.013 PDF
FrmPatientViewAllReport - 2023-04-06T211159.013 PDF
Uploaded by
amir.khann4411Copyright:
Available Formats
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113
Referring Doctor : SELF
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
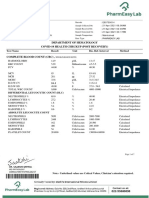
HAEMATOLOGY
HEALTHKIND ACTIVE
Complete Blood Count (CBC)
Haemoglobin (Hb) 16.0 13 - 17 gm/dL
Sample: Whole Blood EDTA
Method: Photometric measurement
Total WBC Count / TLC 8.8 4 - 10 thou/µL
Sample: Whole Blood EDTA
Method: Impedance
RBC Count 5.3 4.5 - 5.5 million/µL
Sample: Whole Blood EDTA
Method: Impedance
PCV / Hematocrit 48.6 40 - 50 %
Sample: Whole Blood EDTA
Method: Impedance
MCV 91.9 83 - 101 fL
Sample: Whole Blood EDTA
Method: Calculated
MCH 30.2 27 - 32 pg
Sample: Whole Blood EDTA
Method: Calculated
MCHC 32.9 31.5 - 34.5 g/dL
Sample: Whole Blood EDTA
Method: Calculated
RDW (Red Cell Distribution Width) 11.7 L 11.8 - 15.6 %
Sample: Whole Blood EDTA
Method: Calculated
DLC (Differential Leucocyte Count)
Method: Flowcytometry/Microscopy
Neutrophils 55 40 - 80 %
Sample: Whole Blood EDTA
Method: VCS Technology & Microscopy
160223106531 Mr. AMIR KHAN
Page No: 1 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583114, 995583113
Referring Doctor : SELF
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
Lymphocytes 37 20 - 40 %
Sample: Whole Blood EDTA
Method: VCS Technology & Microscopy
Eosinophils 05 1-6 %
Sample: Whole Blood EDTA
Method: VCS Technology & Microscopy
Monocytes 02 2 - 10 %
Sample: Whole Blood EDTA
Method: VCS Technology & Microscopy
Basophils 01 0-2 %
Sample: Whole Blood EDTA
Method: VCS Technology & Microscopy
Absolute Neutrophil Count 4840 2000 - 7000 /µL
Sample: Whole Blood EDTA
Absolute Lymphocyte Count 3256 H 1000 - 3000 /µL
Sample: Whole Blood EDTA
Absolute Eosinophil Count 440 20 - 500 /µL
Sample: Whole Blood EDTA
Absolute Monocyte Count 176 L 200 - 1000 /µL
Sample: Whole Blood EDTA
Absolute Basophil Count 88 20 - 100 /µL
Sample: Whole Blood EDTA
Platelet Count 150 150 - 410 thou/µL
Sample: Whole Blood EDTA
Method: Impedance
MPV (Mean Platelet Volume) 12.4 H 6.8 - 10.9 fL
Sample: Whole Blood EDTA
Method: Calculated
Sample: Whole Blood EDTA
Fasting Plasma Glucose 131 H 74 - 106 mg/dl
Sample: Fluoride Plasma - F
Method: Hexokinase
160223106531 Mr. AMIR KHAN
Page No: 2 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113, 995583114,
Referring Doctor : SELF 995583115
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
HbA1C (Glycosylated Hemoglobin)
HbA1c 6.0 H Non Diabetic : < 5.7 % %
Sample: Whole Blood EDTA Prediabetic Range : 5.7 - 6.4 %
Method: High Perfomance Liquid Chromatography (HPLC) Diabetic Range : >= 6.5 %
Goal of Therapy :<7.0 %
Action suggested :>8.0 %
Mean Plasma Glucose 125.5 H < 116 mg/dL
Sample: Whole Blood EDTA
Method: Calculated
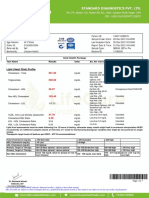
Lipid Profile
Total Cholesterol 171 No risk : < 200 mg/dL
Sample: Serum Moderate risk : 200–239
Method: Spectrophotometery High risk : =240
Triglycerides 193 Desirable : < 150 mg/dL
Sample: Serum Borderline High : 150 - 199
Method: Spectrophotometry High : 200 - 499
Very High : >/= 500
LDL Cholesterol (Calculated) 85 Optimal : <100 mg/dL
Sample: Serum Near Optimal : 100 - 129
Method: Calculated Borderline High : 130 - 160
High : 161 - 189
Very High : >/=190
HDL Cholesterol 47 Low : < 40 mg/dl
Sample: Serum Optimal : 40 - 60
Method: Spectrophometry High : > 60
Non HDL Cholesterol 124 < 130 mg/dL
Sample: Serum
VLDL Cholesterol 38.6 H Desirable 10 - 35 mg/dL
Sample: Serum
Method: Calculated
Total Cholesterol / HDL Ratio 3.64 Low Risk : 3.3 - 4.4
Sample: Serum
Method: Calculated
160223106531 Mr. AMIR KHAN
Page No: 3 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113, 995583114,
Referring Doctor : SELF 995583115
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
Average Risk : 4.5 - 7.0
Moderate Risk : 7.1 - 11.0
High Risk : > 11.0
LDL / HDL Ratio 1.8 0.5 - 3
Sample: Serum
Method: Calculated
Low Risk : 0.5 - 3.0
Moderate Risk : 3.1 - 6.0
High Risk : > 6.0
Liver Function Test (LFT)
Bilirubin Total 0.5 <1.1 mg/dL
Sample: Serum
Method: Spectrophotometery
Bilirubin Direct 0.2 <0.2 mg/dL
Sample: Serum
Method: Spectrophotometery
Serum Bilirubin (Indirect) 0.30 < 0.90 mg/dL
Sample: Serum
Method: Calculated
SGOT / AST 21 <37 U/L
Sample: Serum
Method: Spectrophotometery
SGPT / ALT 36 <41 U/L
Sample: Serum
Method: Spectrophotometery
AST / ALT Ratio 0.58
Sample: Serum
Method: Calculated
Alkaline Phosphatase (ALP) 93 <128 U/L
Sample: Serum
Method: Spectrophotometery
Total Protein 6.9 6.4 - 8.3 g/dL
Sample: Serum
Method: Spectrophotometry
160223106531 Mr. AMIR KHAN
Page No: 4 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113, 995583114,
Referring Doctor : SELF 995583115
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
Albumin 4.8 3.97 - 4.94 g/dL
Sample: Serum
Method: Spectrophotometery
Globulin 2.1 1.9 - 3.7 g/dL
Sample: Serum
Method: Calculated
Albumin/Globulin (A/G) Ratio 2.3 H 1 - 2.1 g/dL
Sample: Serum
Method: Calculated
Gamma-Glutamyl Transferase (GGT) 33 <71 U/L
Sample: Serum
Method: Spectrophotometery
Kidney Function Test
Blood Urea Nitrogen (BUN) 8.76 L 8.87 - 20.5 mg/dL
Sample: Serum
Method: Spectrophotometry-Urease / GLDH
Urea 18.75 17 - 43 mg/dL
Sample: Serum
Method: Spectrophotometery
Creatinine 0.92 0.7 - 1.3 mg/dL
Sample: Serum
Method: Spectrophotometry
BUN Creatinine Ratio 10 10 - 20
Sample: Serum
Method: Calculated
Uric Acid 6.2 3.4 - 7 mg/dL
Sample: Serum
Method: Spectrophotometery
Sodium 142 136 - 145 mmol/L
Sample: Serum
Method: ISE
Potassium 4.4 3.5 - 5.1 mmol/L
Sample: Serum
Method: ISE
160223106531 Mr. AMIR KHAN
Page No: 5 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113, 995583114,
Referring Doctor : SELF 995583115
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
Chloride 103 97 - 107 mmol/L
Sample: Serum
Method: ISE
Calcium 9.6 8.6 - 10 mg/dL
Sample: Serum
Method: Spectrophotometery
Phosphorus 3.4 2.6 - 4.5 mg/dL
Sample: Serum
Method: Spectrophotometry-Phosphomolybdate Reduction
Thyroid Profile Total
Total T3 (Triiodothyronine) 0.76 L 0.8 - 2 ng/mL
Sample: Serum
Method: ECLIA
Total T4 (Thyroxine) 4.85 L 5.1 - 14.1 µg/dL
Sample: Serum
Method: ECLIA
TSH 3rd Generation 3.260 0.27 - 4.2 µIU/mL
Sample: Serum
Method: ECLIA
Complete Blood Count (CBC)
Clinical Significance :
CBC comprises of estimation of the cellular componenets of blood including RBCs, WBCs and Platelets. Mean corpuscular volume (MCV) is a
measure of the size of the average RBC, MCH is a measure of the hemoglobin cointent of the average RBC and MCHC is the hemoglobin
concentration per RBC. The red cell distribution width (RDW) is a measure of the degree of variation in RBC size (anisocytosis) and is helpful in
distinguishing between some anemias. CBC examination is used as a screening tool to confirm a hematologic disorder, to establish or rule out a
diagnosis, to detect an unsuspected hematologic disorder, or to monitor effects of radiation or chemotherapy. Abnormal results may be due to a
primary disorder of the cell-producing organs or an underlying disease. Results should be interpreted in conjunction with the patient's clinical picture
and appropriate additional testing performed.
HbA1C (Glycosylated Hemoglobin)
160223106531 Mr. AMIR KHAN
Page No: 6 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113, 995583114,
Referring Doctor : SELF 995583115
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
Clinical Significance :
Hemoglobin A1c (HbA1c) level reflects the mean glucose concentration over the previous period (approximately 8-12 weeks) and provides a much
better indication of long-term glycemic control than blood and urinary glucose determinations. American Diabetes Association (ADA) include the use
of HbA1c to diagnose diabetes, using a cutpoint of 6.5%. The ADA recommends measurement of HbA1c 3-4 times per year for type 1 and poorly
controlled type 2 diabetic patients, and 2 times per year for well-controlled type 2 diabetic patients) to assess whether a patient's metabolic control
has remained continuously within the target range. Falsely low HbA1c results may be seen in conditions that shorten erythrocyte life span. and may
not reflect glycemic control in these cases accurately.
Lipid Profile
Proposed LDL-C goals in very high risk and extreme risk group patients by the Lipid Association of India.
Very High Risk group(VHRG) Extreme Risk group
Category A Category B
LDL-C goal of <50 mg/dl LDL-C goal of <50 mg/dl LDL-C goal of ≤30 mg/dl
(recommended)
LDL-C goal of ≤30 mg/dl (optional)
High-risk conditions CAD with ≥1 of following:
Any one of following:
CAD with ≥1 of following: 1. Diabetes + polyvascular disease/≥2
1. ASCVD (CAD/PAD/TIA or stroke) 2. major ASCVD risk factors∗/target
2. Homozygous familial 1. Diabetes without target organ organ
3. hypercholesterolemia damage/≤1 major 3. damage
4. Diabetes with ≥2 major ASCVD risk 2. ASCVD risk factors 4. Recurrent ACS (within 12 months)
factors∗/target organ damage 3. Familial hypercholesterolemia 5. despite on LDL-C goal
4. ≥3 major ASCVD risk factors 6. Homozygous familial
5. CKD stage 3B and 4 7. Hypercholesterolemia
6. ≥2 major ASCVD risk factors with
≥1 moderate
7. non-conventional risk factor#
8. Lp(a) ≥50 mg/dl
9. Coronary calcium score ≥300 HU
160223106531 Mr. AMIR KHAN
Page No: 7 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113, 995583114,
Referring Doctor : SELF 995583115
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
10. Extreme of a single risk factor
11. PAD
12. H/o TIA or stroke
13. Non-stenotic carotid plaque
The LDL-C goal of ≤30 mg/dl must be pursued after detailed risk-benefit discussion between physician and patient.
Clinical judgment to be used in decision making if the patient has disease/risk factors not covered in the table, eg. peripheral arterial disease or
cerebrovascular disease.
∗Major ASCVD risk factors: 1. Age- male ≥45 years, female ≥55 years, 2. Family h/o premature CAD- male <55 years, female <65 years, 3.
Smoking/tobacco use, 4. Systemic hypertension, 5.Low HDL (males <40 mg/dl and females <50 mg/dl).
#Moderate non-conventional risk factors: 1. Coronary calcium score 100–299 HU, 2. Increased carotid intima-media thickness, 3. Lp(a) ≥20–49
Uric Acid
Clinical Significance :
Uric acid is the final product of purine metabolism. Serum uric acid levels are raised in case of increased purine synthesis, inherited metabolic disorder,
excess dietary purine intake, increased nucleic acid turnover, malignancy and cytotoxic drugs. Decreased levels are seen in chronic renal failure, severe
hepatocellular disease with reduced purine synthesis, defective renal tubular reabsorption, overtreatment of hyperuricemia with allopurinol, as well as
some cancer therapies.
Total T3 (Triiodothyronine)
Clinical Significance :
Thyroid hormones, T3 and T4, which are secreted by the thyroid gland, regulate a number of developmental, metabolic, and neural activities throughout
the body. The thyroid gland synthesizes 2 hormones - T3 and T4. T3 production in the thyroid gland constitutes approximately 20% of the total
circulating T3, 80% being produced by peripheral conversion from T4. T3 is more potent biologically. Total T3 comprises of Free T3 and bound T3.
Bound T3 remains bound to carrier proteins like thyroid-binding globulin, prealbumin, and albumin). Only the free forms are metabolically active. In
hyperthyroidism, both T4 and T3 levels are usually elevated, but in some rare cases, only T3 elevation is also seen. In hypothyroidism T4 and T3
levels are both low. T3 levels are frequently low in sick or hospitalized euthyroid patients.
Total T4 (Thyroxine)
160223106531 Mr. AMIR KHAN
Page No: 8 of 9
Client Processed By
S A Health Care Centre (Rampur) Pathkind Diagnostic Pvt. Ltd.
Pahadi Gate Road, Near Masjid Jhabbu Kha, Talab Mulla Aeram Ki Gali, Plot No 7, Commercial Yojna, Himgiri,
Rampur, Uttar Pradesh - 244901, C-8171613742 Kanth Road , Moradabad - 244001
Name : Mr. AMIR KHAN Billing Date : 06/04/2023 13:50:28
Age : 46 Yrs Sample Collected on : 06/04/2023 13:51:59
Sex : Male Sample Received on : 06/04/2023 14:21:38
P. ID No. : P1602200038382 Report Released on : 06/04/2023 15:16:46
Accession No : 160223106531 Barcode No. : 995583113, 995583114,
Referring Doctor : SELF 995583115
Referred By : Ref no. :
Report Status - Final
Test Name Result Biological Ref. Interval Unit
Clinical Significance :
Total T4 is synthesized in the thyroid gland. About 0.05% of circulating T4 is in the free or biologically active form. The remainder is bound to
thyroxine-binding globulin (TBG), prealbumin, and albumin. High levels of T4 (and FT4) causes hyperthroidism and low levels lead to
hypothyroidism.
TSH 3rd Generation
Clinical Significance :
TSH levels are elevated in primary hyporthyroidism and low in primary hyperthyroidism. Evaluation of TSH is useful in the differential diagnosis of
primary from secondary and tertiary hypothyroidism. In primary hypothyroidism, TSH levels are elevated, while in secondary and tertiary
hypothyroidism, TSH levels are low or normal. High TSH level in the presence of normal FT4 is called subclinical hypothyroidism and low TSH with
normal FT4 is called subclinical hyperthyroidism. Sick, hospitalized patients may have falsely low or transiently elevated TSH. Significant diurnal
variation is also seen in TSH levels.
** End of Report**
Dr. Deepti Varshney
MBBS,MD (Pathology)
Lab Head
160223106531 Mr. AMIR KHAN
Page No: 9 of 9
You might also like
- Laboratory Test Report: Test Name Result Biological Reference Interval Serum Status: TriglyceridesNo ratings yetLaboratory Test Report: Test Name Result Biological Reference Interval Serum Status: Triglycerides1 page
- L89 - Muzaffar Nagar Cc3 Shop No. 11, Near Dr. Dharampal Singh Sadar Bazar Muzaffarnagar 251001No ratings yetL89 - Muzaffar Nagar Cc3 Shop No. 11, Near Dr. Dharampal Singh Sadar Bazar Muzaffarnagar 2510014 pages
- Department of Hematology Covid-19 Health Checkup (Post Recovery)No ratings yetDepartment of Hematology Covid-19 Health Checkup (Post Recovery)8 pages
- Department of Hematology Comprehensive Full Body Checkup With Vitamin D & B12 Test Name Result Unit Bio. Ref. IntervalNo ratings yetDepartment of Hematology Comprehensive Full Body Checkup With Vitamin D & B12 Test Name Result Unit Bio. Ref. Interval13 pages
- Himani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFNo ratings yetHimani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDF16 pages
- Department of Haematology Test Name Result Unit Bio. Ref. Range MethodNo ratings yetDepartment of Haematology Test Name Result Unit Bio. Ref. Range Method5 pages
- LABORATORY and PATHOLOGY Online Report: Patient InformationNo ratings yetLABORATORY and PATHOLOGY Online Report: Patient Information3 pages
- S03 - Lpl-Preet Vihar C-49, Main Vikas Marg, Preet Vihar, New DELHI-110092 DelhiNo ratings yetS03 - Lpl-Preet Vihar C-49, Main Vikas Marg, Preet Vihar, New DELHI-110092 Delhi4 pages
- Report - HYD31C19101036472842 - 2023 - 10 - 19 - R - L DummyNo ratings yetReport - HYD31C19101036472842 - 2023 - 10 - 19 - R - L Dummy11 pages
- Interpretation: LPL - PSC Paschim Vihar Ii GF, B 1 /10, Paschim ViharNo ratings yetInterpretation: LPL - PSC Paschim Vihar Ii GF, B 1 /10, Paschim Vihar3 pages
- L96 - Mahadev Collection Centre F-135, P C Colony, Kankarbagh PatnaNo ratings yetL96 - Mahadev Collection Centre F-135, P C Colony, Kankarbagh Patna4 pages
- Patient Name Mr. B K Jha Uhid Lab No Sample Date Receiving Date 29/12/2021 12:19PMNo ratings yetPatient Name Mr. B K Jha Uhid Lab No Sample Date Receiving Date 29/12/2021 12:19PM7 pages
- S53 - Syed Kashif Ghani-Fpsc Zakir NagarNo ratings yetS53 - Syed Kashif Ghani-Fpsc Zakir Nagar2 pages
- Mr. Devendra Gupta: Gold Health Package Test Name Results Units100% (1)Mr. Devendra Gupta: Gold Health Package Test Name Results Units7 pages
- A10 - Rohtak Lab Home Visit 1267, Chotu Ram Chowk, Opp Nilli Kothi, Civil Road RohtakNo ratings yetA10 - Rohtak Lab Home Visit 1267, Chotu Ram Chowk, Opp Nilli Kothi, Civil Road Rohtak2 pages
- S51 - Aarogya Patho Lab Vim - 512 Sailashree Vihar, Chandrasekharpur, Bhubaneswar - 751024No ratings yetS51 - Aarogya Patho Lab Vim - 512 Sailashree Vihar, Chandrasekharpur, Bhubaneswar - 75102410 pages
- Dhrivesh: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval Method100% (1)Dhrivesh: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval Method18 pages
- Department of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalNo ratings yetDepartment of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. Interval11 pages
- LPL - Paschim Vhr-Iv Dr. Umesh Mittal, House No - 233, Block A-5 Delhi100% (1)LPL - Paschim Vhr-Iv Dr. Umesh Mittal, House No - 233, Block A-5 Delhi1 page
- Laboratory Test Report: Mrs. V Valli Kumari 81 Years Female100% (1)Laboratory Test Report: Mrs. V Valli Kumari 81 Years Female2 pages
- Haematology Haematology Haematology HaematologyNo ratings yetHaematology Haematology Haematology Haematology5 pages


























































- Laboratory Test Report: Test Name Result Biological Reference Interval Serum Status: TriglyceridesLaboratory Test Report: Test Name Result Biological Reference Interval Serum Status: Triglycerides
- L89 - Muzaffar Nagar Cc3 Shop No. 11, Near Dr. Dharampal Singh Sadar Bazar Muzaffarnagar 251001L89 - Muzaffar Nagar Cc3 Shop No. 11, Near Dr. Dharampal Singh Sadar Bazar Muzaffarnagar 251001
- Department of Hematology Covid-19 Health Checkup (Post Recovery)Department of Hematology Covid-19 Health Checkup (Post Recovery)
- Department of Hematology Comprehensive Full Body Checkup With Vitamin D & B12 Test Name Result Unit Bio. Ref. IntervalDepartment of Hematology Comprehensive Full Body Checkup With Vitamin D & B12 Test Name Result Unit Bio. Ref. Interval
- Himani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDFHimani Singhal 56024602023 04 19 10 55 14 598 1 6 452 133264571589922492 PDF
- Department of Haematology Test Name Result Unit Bio. Ref. Range MethodDepartment of Haematology Test Name Result Unit Bio. Ref. Range Method
- LABORATORY and PATHOLOGY Online Report: Patient InformationLABORATORY and PATHOLOGY Online Report: Patient Information
- S03 - Lpl-Preet Vihar C-49, Main Vikas Marg, Preet Vihar, New DELHI-110092 DelhiS03 - Lpl-Preet Vihar C-49, Main Vikas Marg, Preet Vihar, New DELHI-110092 Delhi
- Report - HYD31C19101036472842 - 2023 - 10 - 19 - R - L DummyReport - HYD31C19101036472842 - 2023 - 10 - 19 - R - L Dummy
- Interpretation: LPL - PSC Paschim Vihar Ii GF, B 1 /10, Paschim ViharInterpretation: LPL - PSC Paschim Vihar Ii GF, B 1 /10, Paschim Vihar
- L96 - Mahadev Collection Centre F-135, P C Colony, Kankarbagh PatnaL96 - Mahadev Collection Centre F-135, P C Colony, Kankarbagh Patna
- Patient Name Mr. B K Jha Uhid Lab No Sample Date Receiving Date 29/12/2021 12:19PMPatient Name Mr. B K Jha Uhid Lab No Sample Date Receiving Date 29/12/2021 12:19PM
- Mr. Devendra Gupta: Gold Health Package Test Name Results UnitsMr. Devendra Gupta: Gold Health Package Test Name Results Units
- A10 - Rohtak Lab Home Visit 1267, Chotu Ram Chowk, Opp Nilli Kothi, Civil Road RohtakA10 - Rohtak Lab Home Visit 1267, Chotu Ram Chowk, Opp Nilli Kothi, Civil Road Rohtak
- S51 - Aarogya Patho Lab Vim - 512 Sailashree Vihar, Chandrasekharpur, Bhubaneswar - 751024S51 - Aarogya Patho Lab Vim - 512 Sailashree Vihar, Chandrasekharpur, Bhubaneswar - 751024
- Dhrivesh: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval MethodDhrivesh: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval Method
- Department of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalDepartment of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. Interval
- LPL - Paschim Vhr-Iv Dr. Umesh Mittal, House No - 233, Block A-5 DelhiLPL - Paschim Vhr-Iv Dr. Umesh Mittal, House No - 233, Block A-5 Delhi
- Laboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleLaboratory Test Report: Mrs. V Valli Kumari 81 Years Female