Shang2012 PDF
Shang2012 PDF
Download as pdf or txt
You might also like
- Asbestos Awareness Quiz #1: AnswersDocument2 pagesAsbestos Awareness Quiz #1: AnswersMichael NcubeNo ratings yet
- Bush-Francis Catatonia Rating ScaleDocument2 pagesBush-Francis Catatonia Rating ScalePsiquiatria Pratica100% (1)
- PEDS HESI RN Case Studies With Practice TestDocument41 pagesPEDS HESI RN Case Studies With Practice Testbngraham4100% (6)
- High Prevalence of Subclinical Left Ventricular Dysfunction in Patients With Psoriatic ArthritisDocument8 pagesHigh Prevalence of Subclinical Left Ventricular Dysfunction in Patients With Psoriatic ArthritisEmanuel NavarreteNo ratings yet
- 2153 8174 25 3 108Document11 pages2153 8174 25 3 108PhyoNyeinChanNo ratings yet
- Cetin 2016Document10 pagesCetin 2016Della Puspita SariNo ratings yet
- Article 7Document5 pagesArticle 7Kamal SaleemNo ratings yet
- Epoc InglesDocument5 pagesEpoc InglesKaren MinoNo ratings yet
- Clinchem 2013 203778 FullDocument9 pagesClinchem 2013 203778 FullHarnadi WonogiriNo ratings yet
- Eci 12222Document9 pagesEci 12222Andikaputra Brahma WidiantoroNo ratings yet
- Impaired Left Ventricular Apical Rotation Is Associated With Disease Activity of Psoriatic ArthritisDocument8 pagesImpaired Left Ventricular Apical Rotation Is Associated With Disease Activity of Psoriatic ArthritisEmanuel NavarreteNo ratings yet
- International Journal of Scientific Research: General MedicineDocument4 pagesInternational Journal of Scientific Research: General MedicineTriple ANo ratings yet
- Anemia in Young Patients With Ischaemic Stroke2015Document6 pagesAnemia in Young Patients With Ischaemic Stroke2015Nicolas RodriguezNo ratings yet
- Saddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismDocument3 pagesSaddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismIJAR JOURNALNo ratings yet
- 8931 26614 2 PB PDFDocument7 pages8931 26614 2 PB PDFMaferNo ratings yet
- Acs 33 241Document9 pagesAcs 33 241Ratna AyieNo ratings yet
- The Burden of Major Adverse Cardiac Events and Antiplatelet Prevention in Patients With Coronary or Peripheral Arterial DiseaseDocument10 pagesThe Burden of Major Adverse Cardiac Events and Antiplatelet Prevention in Patients With Coronary or Peripheral Arterial DiseaseGavrilaNo ratings yet
- Prevalence of Spasticity After Aneurysmal Subarachnoid HaemorrhageDocument5 pagesPrevalence of Spasticity After Aneurysmal Subarachnoid HaemorrhageJorgie Drew MonroeNo ratings yet
- Nikhil Thesis AbstractDocument28 pagesNikhil Thesis AbstractNikhil KalasareNo ratings yet
- Journal 4Document7 pagesJournal 4Denys PutraNo ratings yet
- Angiographic Profile and Treadmill Test RelationshDocument9 pagesAngiographic Profile and Treadmill Test RelationshRajesh SoaNo ratings yet
- Cambios en El EKG Predictores de Edema Pulmonar Neurogénico en Hemorragia SubaracnoideaDocument4 pagesCambios en El EKG Predictores de Edema Pulmonar Neurogénico en Hemorragia SubaracnoideaCristina Duran GarcíaNo ratings yet
- Bilateral Pulmonary Embolism Mimicking Acute Chest Syndrome in A Patient With Sickle Cell Disease: Acase Report and Review of The LiteratureDocument4 pagesBilateral Pulmonary Embolism Mimicking Acute Chest Syndrome in A Patient With Sickle Cell Disease: Acase Report and Review of The LiteratureIJAR JOURNALNo ratings yet
- Damman Et Al 2009 Increased Central Venous Pressure Is Associated With Impaired Renal Function and Mortality in A BroadDocument7 pagesDamman Et Al 2009 Increased Central Venous Pressure Is Associated With Impaired Renal Function and Mortality in A BroadDaniela Andrea Abarca ErazoNo ratings yet
- Effect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisDocument7 pagesEffect of Right Ventricular Function and Pulmonary Pressures On Heart Failure PrognosisMatthew MckenzieNo ratings yet
- AnatolJCardiol 15 8 640 647Document8 pagesAnatolJCardiol 15 8 640 647Pangestu DhikaNo ratings yet
- Diagnostic Approach To Peripheral Arterial DiseaseDocument11 pagesDiagnostic Approach To Peripheral Arterial DiseaseDanielaFernándezDeCastroFontalvoNo ratings yet
- Population-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsDocument11 pagesPopulation-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsIrina NeamtuNo ratings yet
- The Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsDocument5 pagesThe Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsSaskiaaNo ratings yet
- JAH3 6 E007564Document10 pagesJAH3 6 E007564NITACORDEIRONo ratings yet
- Acute Pulmonary Oedema Clinical Characteristics, Prognostic Factors, and In-Hospital ManagementDocument10 pagesAcute Pulmonary Oedema Clinical Characteristics, Prognostic Factors, and In-Hospital ManagementaegonblackNo ratings yet
- Ectopic BeatsDocument5 pagesEctopic Beatssysy_luizaNo ratings yet
- Okello2017 Article RheumaticHeartDiseaseInUgandaPDocument10 pagesOkello2017 Article RheumaticHeartDiseaseInUgandaPyosefinNo ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- Badertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeDocument11 pagesBadertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeNJEBARIKANUYE EugèneNo ratings yet
- Oh y Park - 2023 - Role of Echocardiography in Acute Pulmonary EmboliDocument15 pagesOh y Park - 2023 - Role of Echocardiography in Acute Pulmonary EmboliMa Mercedes CruzNo ratings yet
- CSM 3 2 46 52Document7 pagesCSM 3 2 46 52Santoso 9JimmyNo ratings yet
- MPV SciDocument6 pagesMPV SciMikael AngelooNo ratings yet
- Wesner - Anesthesia For Lower Extremity BypassDocument17 pagesWesner - Anesthesia For Lower Extremity BypassIbet Enriquez PalaciosNo ratings yet
- Angina Contemporary Diagnosis and ManagementDocument12 pagesAngina Contemporary Diagnosis and Managementalejandro montesNo ratings yet
- Carotid Plaque Score and Intima Media Thickness As Predictors of Stroke and Mortality in Hypertensive Patients, 2013Document8 pagesCarotid Plaque Score and Intima Media Thickness As Predictors of Stroke and Mortality in Hypertensive Patients, 2013CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- 10 1016@j Jstrokecerebrovasdis 2017 05 011Document8 pages10 1016@j Jstrokecerebrovasdis 2017 05 011nellieauthorNo ratings yet
- Non Obstructive Versus Obstructive Coronary ArteryDocument7 pagesNon Obstructive Versus Obstructive Coronary ArteryAndreea LeonteNo ratings yet
- European J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificDocument11 pagesEuropean J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificVlad RusuNo ratings yet
- AOMS Art 27239-10Document7 pagesAOMS Art 27239-10re septian IlhamsyahNo ratings yet
- The Relationship Between PlasmaDocument8 pagesThe Relationship Between PlasmacyneuronNo ratings yet
- Diastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseaseDocument6 pagesDiastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseasehanifahrafaNo ratings yet
- MINOCA Agewall 2017Document11 pagesMINOCA Agewall 2017mate ellaNo ratings yet
- Liver Stiffness As Measured by Transient Elastography - 2021 - American Heart JDocument6 pagesLiver Stiffness As Measured by Transient Elastography - 2021 - American Heart JGarret BarriNo ratings yet
- Timing CirurgicoDocument7 pagesTiming CirurgicomarceloNo ratings yet
- Circulation 1975 Burggraf 146 56Document12 pagesCirculation 1975 Burggraf 146 56Zikri Putra Lan LubisNo ratings yet
- EFNS Congress Vienna Semax AbstractDocument60 pagesEFNS Congress Vienna Semax AbstractnontjeNo ratings yet
- Use of Neutrophil Count in Early Diagnosis and Risk Stratification of AMIDocument9 pagesUse of Neutrophil Count in Early Diagnosis and Risk Stratification of AMIratihNo ratings yet
- PE and CHFDocument9 pagesPE and CHFKu Li ChengNo ratings yet
- 10 16899-jcm 853237-1486847Document5 pages10 16899-jcm 853237-1486847rdelgado3No ratings yet
- Dilemmas in The Diagnosis and Management of Antiphospholipid SyndromeDocument15 pagesDilemmas in The Diagnosis and Management of Antiphospholipid Syndromeanna531No ratings yet
- On-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyDocument8 pagesOn-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyGono GenieNo ratings yet
- Euro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralDocument9 pagesEuro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralIvan MihailovicNo ratings yet
- Jurnal HipertensiDocument5 pagesJurnal HipertensiRanhie Pen'ned CendhirhieNo ratings yet
- Abstrak INAECHODocument21 pagesAbstrak INAECHOAgung Angga KesumaNo ratings yet
- Coronary Vasomotion AbnormalitiesFrom EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaNo ratings yet
- Clinical Cases in Chronic Thromboembolic Pulmonary HypertensionFrom EverandClinical Cases in Chronic Thromboembolic Pulmonary HypertensionWilliam R. AugerNo ratings yet
- Case Scenario Drug Study - VicenteDocument4 pagesCase Scenario Drug Study - VicenteLouraine VicenteNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanCarl Andre ReyesNo ratings yet
- Approach To HeadacheDocument49 pagesApproach To Headachegea pandhita sNo ratings yet
- Aricol Cancer PancreaticDocument10 pagesAricol Cancer PancreaticBuliga ClaudiaNo ratings yet
- Extra Edge Info: SurgeryDocument3 pagesExtra Edge Info: SurgeryskNo ratings yet
- Diseases of The Pulp: Made by Isha ParikhDocument23 pagesDiseases of The Pulp: Made by Isha ParikhDevarshi ThakkarNo ratings yet
- Basic First Aid 0808Document72 pagesBasic First Aid 0808BS AnilKumarNo ratings yet
- Fitt 2Document12 pagesFitt 2glldr26No ratings yet
- Intermittent Fasting Facts and Myths: Metabolic Benefits of Intermittent FastingDocument4 pagesIntermittent Fasting Facts and Myths: Metabolic Benefits of Intermittent FastingIJAR JOURNALNo ratings yet
- Nosocomial Infection. BPTDocument44 pagesNosocomial Infection. BPTAanchal GuptaNo ratings yet
- Bach Flower RemediesDocument11 pagesBach Flower Remedieskrasivaad100% (4)
- Northwell Direct - Respirator Medical Evaluation QuestionnaireDocument5 pagesNorthwell Direct - Respirator Medical Evaluation QuestionnaireFaithNo ratings yet
- Coarse in The WardDocument41 pagesCoarse in The WardPandesal with EggNo ratings yet
- Case 2-Part 1-Kalvakota ManinithyaDocument3 pagesCase 2-Part 1-Kalvakota ManinithyamaninithyaNo ratings yet
- 1.11 Anti-Seizure Epilepsy (Seizures) Drugs - Rani Qasem 2015-2016Document27 pages1.11 Anti-Seizure Epilepsy (Seizures) Drugs - Rani Qasem 2015-2016Faisal FahadNo ratings yet
- PEDIATRICSDocument51 pagesPEDIATRICSJoanne BlancoNo ratings yet
- Clinical Features and Diagnosis of Lower Extremity Peripheral Artery DiseaseDocument42 pagesClinical Features and Diagnosis of Lower Extremity Peripheral Artery DiseaseAdrianaIDCNo ratings yet
- Silabus Training Imo 2011-DigestifDocument2 pagesSilabus Training Imo 2011-DigestiffinaakmaliaNo ratings yet
- Devic's Disease - The Pathogenesis, Diagnosis and Treatment: Choroba Devica-Patogeneza, Diagnostyka I LeczenieDocument14 pagesDevic's Disease - The Pathogenesis, Diagnosis and Treatment: Choroba Devica-Patogeneza, Diagnostyka I LeczenieVonny MaharaniNo ratings yet
- Assisting With Lumbar PunctureDocument4 pagesAssisting With Lumbar PuncturePhelanCoy100% (1)
- DrugDocument15 pagesDrugknxdg86vk2No ratings yet
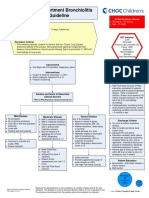
- Emergency Department Bronchiolitis Care Guideline: Inclusion CriteriaDocument3 pagesEmergency Department Bronchiolitis Care Guideline: Inclusion CriteriaPatricia KoikyNo ratings yet
- Fetal Face and Neck - Student SlidesDocument35 pagesFetal Face and Neck - Student SlidessdafasdNo ratings yet
- Páginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Document1 pagePáginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Sotfonic SotfonicNo ratings yet
- Template BHW Registry Form 2023Document6 pagesTemplate BHW Registry Form 2023daisy1279.dds165No ratings yet
- Croup (Laryngotracheobronchitis) : EtiologyDocument13 pagesCroup (Laryngotracheobronchitis) : EtiologyOmar mohamedNo ratings yet
- Sam 2023Document94 pagesSam 2023Shadow TiNo ratings yet