Maternal Ncps Final
Maternal Ncps Final
Download as docx, pdf, or txt
You might also like
- RRB NursingDocument16 pagesRRB Nursingblacknoob231306No ratings yet
- Case Study On PROMDocument11 pagesCase Study On PROMPabhat Kumar89% (9)
- Case Scenario: Prostate CancerDocument5 pagesCase Scenario: Prostate Cancer24 PAULINO ALDRIN MUJARNo ratings yet
- Nursing Care Plans (NCP) of Abruptio PlacentaDocument13 pagesNursing Care Plans (NCP) of Abruptio PlacentaKath76% (21)
- NCP 3rd YearDocument6 pagesNCP 3rd YearTotoro AblogNo ratings yet
- Mod 3C Nursing Care Plan - Macanas, Evangeline Anne A. BSN 2BDocument4 pagesMod 3C Nursing Care Plan - Macanas, Evangeline Anne A. BSN 2BEvangeline Anne MacanasNo ratings yet
- NCP Alterations in Normal LaborDocument9 pagesNCP Alterations in Normal LaborCameron De GuzmanNo ratings yet
- Waiters PATIENT CARE PLAN 2020 For PPHDocument3 pagesWaiters PATIENT CARE PLAN 2020 For PPHTommieNo ratings yet
- MS Soapie #1Document2 pagesMS Soapie #1Fatima KateNo ratings yet
- Nursing Care Plan 1Document1 pageNursing Care Plan 1Janhabi BeheraNo ratings yet
- Ncma 219 Rle Task 1Document10 pagesNcma 219 Rle Task 1Gina PrancelisoNo ratings yet
- Threatened Abortion - Edited 1Document55 pagesThreatened Abortion - Edited 1اكينو ستيفاني100% (1)
- Case Study On PROMDocument11 pagesCase Study On PROMPatricia Denise TiradoNo ratings yet
- NCM 107 (Related Learning Experience) : in Partial Fulfillment of The Requirement inDocument4 pagesNCM 107 (Related Learning Experience) : in Partial Fulfillment of The Requirement inTiffany Joy QuiliopeNo ratings yet
- Now, Try Some Big Leap.: Keep GoingDocument10 pagesNow, Try Some Big Leap.: Keep GoingCameron De GuzmanNo ratings yet
- NMT 06101: Care of A Woman With Obstetric Emergency ConditionsDocument10 pagesNMT 06101: Care of A Woman With Obstetric Emergency ConditionsWILBARD JOACHIMNo ratings yet
- GROUP E2 1M Antenatal ComplicationsDocument25 pagesGROUP E2 1M Antenatal ComplicationsJason Matthew ImpasNo ratings yet
- NCP Post PartumDocument2 pagesNCP Post PartumsteffiNo ratings yet
- Nle BulletsDocument53 pagesNle BulletsdjhemzNo ratings yet
- Facto NCPDocument3 pagesFacto NCPkkd nyleNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Case Report On OligohydramniosDocument3 pagesCase Report On OligohydramniosRakhi BhagatNo ratings yet
- NCM 112 - Rle Nursing Care Plan: To Have Baseline Data. Normal Values Indicate Adequate Tissue PerfusionDocument7 pagesNCM 112 - Rle Nursing Care Plan: To Have Baseline Data. Normal Values Indicate Adequate Tissue Perfusiontherese BNo ratings yet
- Darunday NCP DrugstudyDocument16 pagesDarunday NCP DrugstudyEzra Miguel DarundayNo ratings yet
- Fluid Volume Deficit related to vaginal bleedingDocument8 pagesFluid Volume Deficit related to vaginal bleedingChelsea Mercado BalbaronaNo ratings yet
- May 8-9Document5 pagesMay 8-9MineTagraNo ratings yet
- Hypovolemic Shock Sample NCPDocument14 pagesHypovolemic Shock Sample NCPRENEROSE TORRES100% (1)
- Nursing Care Plan: RationaleDocument5 pagesNursing Care Plan: Rationalerona-chanNo ratings yet
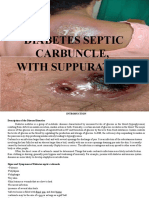
- Diabetes Septic CarbuncleDocument25 pagesDiabetes Septic CarbuncleLouie George Neri0% (1)
- BOX 17.4 NCP Postpartum HemorrhageDocument4 pagesBOX 17.4 NCP Postpartum HemorrhageJam AliNo ratings yet
- NCP PediatricDocument5 pagesNCP PediatricSL Hanna NebridaNo ratings yet
- Jevans TTP Care Plan 4Document8 pagesJevans TTP Care Plan 4api-439893609No ratings yet
- Guinitaran, Christine Ann P. BSN 4 Abruptio Placenta Nursing Care PlanDocument19 pagesGuinitaran, Christine Ann P. BSN 4 Abruptio Placenta Nursing Care PlanGemmalene PaclebNo ratings yet
- Abruptio Placenta NCP 2 FinalDocument19 pagesAbruptio Placenta NCP 2 FinalTin100% (1)
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- Ob Rotation 4Document6 pagesOb Rotation 4Arvinjohn GacutanNo ratings yet
- Case StudyDocument8 pagesCase StudyKrisianne Mae Lorenzo FranciscoNo ratings yet
- Eugenio (NCP and Patient Education)Document6 pagesEugenio (NCP and Patient Education)Sam EugenioNo ratings yet
- TTP Care Plan 1 JevansDocument8 pagesTTP Care Plan 1 Jevansapi-439893609No ratings yet
- Mark Bhen Sumbad - ACTIVITY-2Document2 pagesMark Bhen Sumbad - ACTIVITY-2Mb SumbadNo ratings yet
- Prado, Catherine BSN IIB (Activity 1 Case Scenario)Document52 pagesPrado, Catherine BSN IIB (Activity 1 Case Scenario)Catherine PradoNo ratings yet
- NCP-ABRUPTIO PLACENTAE - PeregrinoDocument5 pagesNCP-ABRUPTIO PLACENTAE - PeregrinoJOYCE ANN PEREGRINONo ratings yet
- Proper Venipuncture ProcedureDocument4 pagesProper Venipuncture ProcedureAngelo Jude Cumpio100% (1)
- Fdar Prcedure EndorsmentDocument9 pagesFdar Prcedure EndorsmentFelipe MeranoNo ratings yet
- Doctor's OrderDocument3 pagesDoctor's OrderStephen S. PadayhagNo ratings yet
- Case StudyDocument6 pagesCase StudyNygie HaudarNo ratings yet
- Leong Et Al-2004-BJOG: An International Journal of Obstetrics & GynaecologyDocument2 pagesLeong Et Al-2004-BJOG: An International Journal of Obstetrics & GynaecologyAngie MandeoyaNo ratings yet
- Abortion BSN 0PR-2: Case Study of BelleDocument27 pagesAbortion BSN 0PR-2: Case Study of BellekervinNo ratings yet
- NCP Pedia WardDocument2 pagesNCP Pedia WardSyrelle GomezNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationBiway RegalaNo ratings yet
- Midwife Care Plan AbruptioDocument6 pagesMidwife Care Plan AbruptioDivina Gracia Vibal CieloNo ratings yet
- Bernas Rhu OpstDocument3 pagesBernas Rhu Opstrbvergz1z5No ratings yet
- Adobe Scan 10 Oct 2023Document2 pagesAdobe Scan 10 Oct 2023sandeshlikesNo ratings yet
- Spina Bifida CaseanalysisDocument26 pagesSpina Bifida Caseanalysisaasimon2466cabNo ratings yet
- NCP Example Pre EclampsiaDocument6 pagesNCP Example Pre EclampsiaChristian Joseph OpianaNo ratings yet
- Excess Fluid Volume Liver CirrhosisDocument3 pagesExcess Fluid Volume Liver CirrhosisSHANIA HASEENAH SALAZARNo ratings yet
- Pedia NCPDocument6 pagesPedia NCPZel MartinezNo ratings yet
- PPH.presentationDocument53 pagesPPH.presentationThe UmerNo ratings yet
- NS1 Case PresDocument8 pagesNS1 Case PresjoanaalpayNo ratings yet
- Nursing Care PlanDocument12 pagesNursing Care Plankeishaaa29100% (6)
- Or LFD 3RD Year Second Sem Finalll 2Document2 pagesOr LFD 3RD Year Second Sem Finalll 2Carey Jamille YadanNo ratings yet
- Hyperthermia - NCPDocument5 pagesHyperthermia - NCPCarey Jamille YadanNo ratings yet
- LFD Med WardDocument2 pagesLFD Med WardCarey Jamille YadanNo ratings yet
- Yadan - LFD Icu Summer TermDocument3 pagesYadan - LFD Icu Summer TermCarey Jamille YadanNo ratings yet
- Arfa Comm Duty z1&2 - YadanDocument2 pagesArfa Comm Duty z1&2 - YadanCarey Jamille YadanNo ratings yet
- Prelim Topics in Geria Part 1Document22 pagesPrelim Topics in Geria Part 1Carey Jamille YadanNo ratings yet
- Higlighted For FNCPSDocument55 pagesHiglighted For FNCPSCarey Jamille YadanNo ratings yet
- Progress Notes 1Document2 pagesProgress Notes 1Carey Jamille YadanNo ratings yet
- DexamethasoneDocument3 pagesDexamethasoneCarey Jamille YadanNo ratings yet
- Clinical Practice Guidelines - Protocols - July 2018Document229 pagesClinical Practice Guidelines - Protocols - July 2018Muzi SitholeNo ratings yet
- SURAT CINTA ULM 2022 + JawabanDocument25 pagesSURAT CINTA ULM 2022 + JawabanBerry BancinNo ratings yet
- Module 5 - MCN TransesDocument6 pagesModule 5 - MCN TransesCarl UyNo ratings yet
- Uterine AtonyDocument20 pagesUterine AtonyKpiebakyene Sr. MercyNo ratings yet
- Salome Mwashiuya ProposalDocument39 pagesSalome Mwashiuya ProposalHerryNo ratings yet
- effectiveness_of_the_intrauterine_balloon.11Document7 pageseffectiveness_of_the_intrauterine_balloon.11Martín GallegosNo ratings yet
- SYNOPSISDocument25 pagesSYNOPSISpriyankaNo ratings yet
- FIGO Recommendations On The Management of Postpartum Hemorrhage 2022Document48 pagesFIGO Recommendations On The Management of Postpartum Hemorrhage 2022Ivan Antonio Tarrillo HuaricachaNo ratings yet
- Postpartum ComplicationsDocument63 pagesPostpartum Complications9s8fjxwhsfNo ratings yet
- MCN FinalsDocument29 pagesMCN FinalsClifford Ricardel CañaNo ratings yet
- Uterine AtonyDocument1 pageUterine AtonyYakumaNo ratings yet
- Drug Used in LabourDocument15 pagesDrug Used in LabourNorlili MurinaNo ratings yet
- Dr Asma answered questions 2024Document33 pagesDr Asma answered questions 2024Sbahat FatimaNo ratings yet
- Module 5 - MCN TransesDocument6 pagesModule 5 - MCN TransesCarl UyNo ratings yet
- OB Revalida Samplex - ZAPDocument38 pagesOB Revalida Samplex - ZAPLowell SalvadorNo ratings yet
- Obstetrics and Gynecology (Internal Medicine) Merged PDFDocument122 pagesObstetrics and Gynecology (Internal Medicine) Merged PDFHimanshuNo ratings yet
- Tarifa, Vannesa Joy B. (NU-202) Module 5 Assignment (NCM-109)Document3 pagesTarifa, Vannesa Joy B. (NU-202) Module 5 Assignment (NCM-109)Vannesa TarifaNo ratings yet
- Obstetrics V13 Obstetric Emergencies Chapter 1614623048Document12 pagesObstetrics V13 Obstetric Emergencies Chapter 1614623048Jeferson CuaranNo ratings yet
- Lasa Case ReportDocument5 pagesLasa Case ReportDeepali GuptaNo ratings yet
- Postpartum Complication NCM109 YBOA 2Document4 pagesPostpartum Complication NCM109 YBOA 2syroise margauxNo ratings yet
- SOAL UJIAN MCQ Jan 2022Document22 pagesSOAL UJIAN MCQ Jan 2022densus awNo ratings yet
- Rev 3 - Bleeding in Late Pregnancy& Complications of 3rd Stage 2022Document18 pagesRev 3 - Bleeding in Late Pregnancy& Complications of 3rd Stage 2022Nabaa YasienNo ratings yet
- NCM 109 Module 3mDocument25 pagesNCM 109 Module 3mKyle ChuaNo ratings yet
- High - Risk Labor and Delivery 2Document106 pagesHigh - Risk Labor and Delivery 2Charmaine Louie Macalanda Lopez-Soriano100% (2)
- Obstetric EmergenciesDocument96 pagesObstetric Emergenciessembakarani thevagumaran100% (1)
- Perdarahan Pasca SalinDocument36 pagesPerdarahan Pasca SalinbennyrolandnababanNo ratings yet
- Postpartum Hemorrhage: Prepared By: Bande, Kyla Marie O. Lorente, Alfie John CDocument22 pagesPostpartum Hemorrhage: Prepared By: Bande, Kyla Marie O. Lorente, Alfie John CNi Ki TaNo ratings yet
- NCM 109 (Prelims) - Lesson 1Document5 pagesNCM 109 (Prelims) - Lesson 1nianNo ratings yet
- Retained Placenta and Postpartum Hemorrhage: Time Is Not EverythingDocument9 pagesRetained Placenta and Postpartum Hemorrhage: Time Is Not EverythingWalid AsyhariNo ratings yet