Anesthesia For Ophthalmic Surgery: An Educational Review
Anesthesia For Ophthalmic Surgery: An Educational Review
Download as pdf or txt
You might also like
- AO Principles of Fracture Management in The Dog and CatDocument490 pagesAO Principles of Fracture Management in The Dog and CatmafercaavNo ratings yet
- Endo Don TicDocument8 pagesEndo Don TicArmareality Armareality100% (1)
- Super Speciality Hospital in KanpurDocument178 pagesSuper Speciality Hospital in KanpurgauravsriNo ratings yet
- Lower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor FracturesDocument5 pagesLower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor Fracturesstoia_sebiNo ratings yet
- Anastesi Operasi Katarak AyuDocument23 pagesAnastesi Operasi Katarak AyuOfkom UnhasNo ratings yet
- Use of A Fibrin Adhesive For Conjunctival Closure in TrabeculectomyDocument4 pagesUse of A Fibrin Adhesive For Conjunctival Closure in TrabeculectomyAlexandre IshizakiNo ratings yet
- Hematoma by PSADocument5 pagesHematoma by PSAMouy EngNo ratings yet
- Boston XODocument5 pagesBoston XOjuan diego RuizNo ratings yet
- Piis2058534917300604 PDFDocument7 pagesPiis2058534917300604 PDFirvan rahmanNo ratings yet
- Local Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryDocument8 pagesLocal Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryFrancisco Javier Rodriguez MolinaNo ratings yet
- Refractive Surgery - The LancetDocument14 pagesRefractive Surgery - The Lancetaann86911No ratings yet
- Eer 4 1 90 102Document13 pagesEer 4 1 90 102bakkouriyacineNo ratings yet
- Effects of Intracameral Cefuroxime On CornealDocument6 pagesEffects of Intracameral Cefuroxime On CornealClaudia MirandaNo ratings yet
- 10.36516-jocass.1319359-3230420Document4 pages10.36516-jocass.1319359-3230420watty3448No ratings yet
- A Comparison of Topical and Retrobulbar PDFDocument8 pagesA Comparison of Topical and Retrobulbar PDFAnggi Junita Endamia BangunNo ratings yet
- Jurnal Mata 5Document6 pagesJurnal Mata 5Dahru KinanggaNo ratings yet
- Intracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryDocument5 pagesIntracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryGlaucoma UnhasNo ratings yet
- Transconjunctival and Subciliary Approach in The TDocument10 pagesTransconjunctival and Subciliary Approach in The TKaren StefNo ratings yet
- Clinical StudyDocument6 pagesClinical StudyKarina Mega WNo ratings yet
- Comparison of A Preservative Free Nonsteroidal.Document7 pagesComparison of A Preservative Free Nonsteroidal.Danty IndriastutyNo ratings yet
- Alamanos 2016Document12 pagesAlamanos 2016dana40018256No ratings yet
- Current ConceptsDocument300 pagesCurrent ConceptsGuilherme Bender LimaNo ratings yet
- Anestesia para Cirugia VitroretinealDocument6 pagesAnestesia para Cirugia Vitroretinealluis castro martinezNo ratings yet
- Lens: Management of Cataract Surgery, Cataract Prevention, and Floppy Iris SyndromeDocument16 pagesLens: Management of Cataract Surgery, Cataract Prevention, and Floppy Iris SyndromeMagny DcrNo ratings yet
- What's New in Ophthalmic AnaesthesiaDocument6 pagesWhat's New in Ophthalmic AnaesthesiaRahmi Ami100% (1)
- s12886 022 02600 XDocument8 pagess12886 022 02600 XHariom ShuklaNo ratings yet
- New Perative UlcerDocument5 pagesNew Perative UlcerkautsarreNo ratings yet
- DownloadDocument14 pagesDownloadhasan nazzalNo ratings yet
- Comparison of The Efficacy of Endoscopic Tympanoplasty With Microscopic Tympanoplasty - April - 2021 - 1148149816 - 7001902Document4 pagesComparison of The Efficacy of Endoscopic Tympanoplasty With Microscopic Tympanoplasty - April - 2021 - 1148149816 - 7001902dilshadahmed201No ratings yet
- Anestesia Ocular 2018 PDFDocument4 pagesAnestesia Ocular 2018 PDFChristian Andres Cruz PerezNo ratings yet
- Failed Root Canals The Case For Apicoectomy (Periradicular Surgery)Document6 pagesFailed Root Canals The Case For Apicoectomy (Periradicular Surgery)Karin Noga VerhagenNo ratings yet
- Medoralv21 I1 p111Document7 pagesMedoralv21 I1 p111Marco ColacinoNo ratings yet
- 12 DecDocument43 pages12 DecJayesh ThakkarNo ratings yet
- Day 4 - APPEC 2021 PDFDocument397 pagesDay 4 - APPEC 2021 PDFGaurieNo ratings yet
- Sulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryDocument6 pagesSulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryPrizilia SaimimaNo ratings yet
- Research ArticleDocument8 pagesResearch Articlekoas mr14No ratings yet
- Discovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualDocument8 pagesDiscovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualGuillermo Castro ContardoNo ratings yet
- Phacoemulsification_and_Intraocular_Lens_ImplantatDocument9 pagesPhacoemulsification_and_Intraocular_Lens_ImplantatScally WagNo ratings yet
- Editorial: The Management of Retinal Detachment: Techniques and PerspectivesDocument3 pagesEditorial: The Management of Retinal Detachment: Techniques and PerspectivesSarahNo ratings yet
- Mcculley 2012Document11 pagesMcculley 2012Luisa Mayta PitmanNo ratings yet
- The Joint Tip Graft: A Joint Support For Rim, Facet and Infratip Lobule in RhinoplastyDocument7 pagesThe Joint Tip Graft: A Joint Support For Rim, Facet and Infratip Lobule in RhinoplastyGöksel TurhalNo ratings yet
- SRC JCCS 20 053 PDFDocument5 pagesSRC JCCS 20 053 PDFProf. Ashraful IslamNo ratings yet
- Ocular Drug Delivery Systems - An Overview PDFDocument35 pagesOcular Drug Delivery Systems - An Overview PDFYuendri IrawantoNo ratings yet
- Eye Surgery in Hot Climates BibliographyDocument2 pagesEye Surgery in Hot Climates BibliographyNurul HasanahNo ratings yet
- Thesis New 2Document66 pagesThesis New 2odoemelawrenceNo ratings yet
- Apm 20050Document6 pagesApm 20050hnzzn2bymdNo ratings yet
- Current Advances in Ophthalmic TechnologyFrom EverandCurrent Advances in Ophthalmic TechnologyParul IchhpujaniNo ratings yet
- Evaluation of The Safety and Efficacy of Therapeutic Bandage Contact Lenses On Post-Cataract Surgery PatientsDocument7 pagesEvaluation of The Safety and Efficacy of Therapeutic Bandage Contact Lenses On Post-Cataract Surgery PatientsFitrian Hanif ZulkarnainNo ratings yet
- Westfall 2019Document6 pagesWestfall 2019yohanasmjtNo ratings yet
- 1.endoscopic Ear Surgery - The Future of Otologic SurgeryDocument3 pages1.endoscopic Ear Surgery - The Future of Otologic SurgeryAnonymous ST1Ot2GAHxNo ratings yet
- Five-Year Results of ViscotrabeculotomyDocument10 pagesFive-Year Results of ViscotrabeculotomyChintya Redina HapsariNo ratings yet
- VitrektomiDocument5 pagesVitrektomiSashikirana KiranNo ratings yet
- Therapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismDocument7 pagesTherapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismStephanie PfengNo ratings yet
- Case Report: Subconjunctival Haemorrhage Following Extraction of A ToothDocument2 pagesCase Report: Subconjunctival Haemorrhage Following Extraction of A ToothMushidayah AuliaNo ratings yet
- Assessing The Rebound Phenomenon in Different Myopia Control Treatment A Systematic Revi 2024Document10 pagesAssessing The Rebound Phenomenon in Different Myopia Control Treatment A Systematic Revi 2024aya mahmoudNo ratings yet
- Phacoemulsification Versus Manual Small Incision Cataract Surgery in Hard NuclearDocument6 pagesPhacoemulsification Versus Manual Small Incision Cataract Surgery in Hard NuclearRagni MishraNo ratings yet
- Assessment of Complications of Peribulbar Block In.6Document5 pagesAssessment of Complications of Peribulbar Block In.6Focus LensNo ratings yet
- Contents OcnaDocument4 pagesContents OcnaGirish SubashNo ratings yet
- Transient Corneal Edema After Phacoemulsification: Original ArticleDocument5 pagesTransient Corneal Edema After Phacoemulsification: Original ArticlesarassashaNo ratings yet
- Surgical Outcome of Blowout Fractures of Floor of Orbit A Case Series Of5 Patients 2155 9570 1000518Document5 pagesSurgical Outcome of Blowout Fractures of Floor of Orbit A Case Series Of5 Patients 2155 9570 1000518Luqman HakimNo ratings yet
- Efficacy of Triple Therapy in Auricular KeloidsDocument5 pagesEfficacy of Triple Therapy in Auricular Keloidsborneo exotic herbsNo ratings yet
- The Control of Conjunctival Fibrosis As A Paradigm For The Prevention of Ocular Fibrosis-Related Blindness. "Fibrosis Has Many Friends"Document12 pagesThe Control of Conjunctival Fibrosis As A Paradigm For The Prevention of Ocular Fibrosis-Related Blindness. "Fibrosis Has Many Friends"Ginda Chitra PuspitaNo ratings yet
- Duchenne Muscular Dystrophy Information SheetDocument2 pagesDuchenne Muscular Dystrophy Information Sheetapi-319448388No ratings yet
- (Dala M Rupi AH) Loka Si: Sem Ua: Sam Pai Tang Gal 25 Mei 2022Document20 pages(Dala M Rupi AH) Loka Si: Sem Ua: Sam Pai Tang Gal 25 Mei 2022Henry BudiawanNo ratings yet
- Postoperative Hip Answer SheetDocument19 pagesPostoperative Hip Answer SheetCrisha Ann Billones BacutaNo ratings yet
- Adolescent Alcohol and Drug Involvement Scale (AADIS)Document3 pagesAdolescent Alcohol and Drug Involvement Scale (AADIS)Janine CarmelNo ratings yet
- Polysitemia VeraDocument3 pagesPolysitemia VeraedwinsyahNo ratings yet
- Drama Initiative Monologues WebsiteDocument9 pagesDrama Initiative Monologues WebsiteWork PrinceNo ratings yet
- Delos Santos v. CoADocument2 pagesDelos Santos v. CoARonnie RimandoNo ratings yet
- Case Study or (PGO)Document10 pagesCase Study or (PGO)Nikki Navalta Dela CruzNo ratings yet
- Vandeventer 2016Document10 pagesVandeventer 2016juanrangoneNo ratings yet
- 5c Faculty of Modern MedicineDocument14 pages5c Faculty of Modern MedicineRamesh SahNo ratings yet
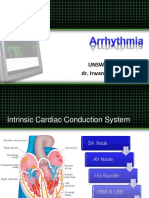
- Unswagati, Cirebon Dr. Irwan M. Loebis, SPJPDocument55 pagesUnswagati, Cirebon Dr. Irwan M. Loebis, SPJPApriliani Nur Puspita SariNo ratings yet
- Effect of Limonene On Permeation Enhancement of Ketoprofen in Palm Oil Esters NanoemulsionDocument6 pagesEffect of Limonene On Permeation Enhancement of Ketoprofen in Palm Oil Esters NanoemulsionStuart GunzburgNo ratings yet
- Awards DetailsDocument3 pagesAwards DetailsWipro Foundation KARNo ratings yet
- On Rounds - 1000 Internal Medicine Pearls - 9781496322210 - Medicine & Health Science Books @Document5 pagesOn Rounds - 1000 Internal Medicine Pearls - 9781496322210 - Medicine & Health Science Books @wong0% (1)
- Lesson Plan On ManiaDocument20 pagesLesson Plan On ManiaAnkush Kulat Patil100% (1)
- Kirschner-Wire Fixation For Postburn Flexion Contracture Deformity and Consequences On Articular SurfaceDocument5 pagesKirschner-Wire Fixation For Postburn Flexion Contracture Deformity and Consequences On Articular SurfaceDanar Hari AdhimuktiNo ratings yet
- Prep For Performance Sho Botham DecodanzDocument32 pagesPrep For Performance Sho Botham DecodanzSunsmart SstplNo ratings yet
- Controversies in Orthopaedic OncologyDocument5 pagesControversies in Orthopaedic OncologyCarlosNo ratings yet
- Blood Pressure: Vital SignsDocument19 pagesBlood Pressure: Vital SignsBruno SuárezNo ratings yet
- Vick Resume 201900Document4 pagesVick Resume 201900api-458528237No ratings yet
- Pursed Lip BreathingDocument4 pagesPursed Lip BreathingDinesh KumarNo ratings yet
- (Bioethics 2) 2.02.02 - Case - Gaetan Dugas (Pat G) PDFDocument1 page(Bioethics 2) 2.02.02 - Case - Gaetan Dugas (Pat G) PDFMikee MeladNo ratings yet
- Healing ArchitectureDocument5 pagesHealing ArchitectureSUDHAKARMANI100% (2)
- Building On ValuesDocument392 pagesBuilding On ValuesRon J. BeliardNo ratings yet
- Procedures - Risk AssessmentDocument16 pagesProcedures - Risk Assessmentapi-303619994No ratings yet
- Clinical Biomechanics in Implant DentistryDocument36 pagesClinical Biomechanics in Implant DentistryMahadevan Ravichandran100% (4)
- ABC Versus CAB For Cardiopulmonary ResuscitationDocument16 pagesABC Versus CAB For Cardiopulmonary Resuscitationaldo199No ratings yet
- 2014-01-06 Gulf War Illness Tied To Cipro AntibioticsDocument10 pages2014-01-06 Gulf War Illness Tied To Cipro AntibioticsAvelox FloxNo ratings yet