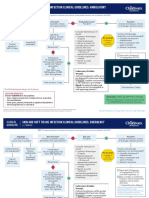
Carbapenem vs. Non-Carbapenem Antibiotics For Ventilator-Associated Pneumonia
Carbapenem vs. Non-Carbapenem Antibiotics For Ventilator-Associated Pneumonia
Download as pdf or txt
You might also like
- Common Pediatric Cases in OpdDocument90 pagesCommon Pediatric Cases in OpdJamie Sebastian100% (3)
- D-K For Amoebae and FlagellatesDocument2 pagesD-K For Amoebae and FlagellatesPrezyNo ratings yet
- Antimicrobial Resistance in Libya - 1970-2011Document8 pagesAntimicrobial Resistance in Libya - 1970-2011Khalifa Sifaw Ghenghesh100% (2)
- Knowledge of and Compliance With Standard Precautions Among Nursing StudentsDocument14 pagesKnowledge of and Compliance With Standard Precautions Among Nursing StudentsLeodoro Labrague100% (1)
- A Systematic Review and Meta-Analyses Show That Carbapenem Use and Medical Devices Are The Leading Risk Factors For Carbapenem-Resistant Pseudomonas Aeruginosa PDFDocument12 pagesA Systematic Review and Meta-Analyses Show That Carbapenem Use and Medical Devices Are The Leading Risk Factors For Carbapenem-Resistant Pseudomonas Aeruginosa PDFGRAÇAS PERFUMARIANo ratings yet
- New Guidelines For NeumoniaDocument7 pagesNew Guidelines For NeumoniacarlosNo ratings yet
- Hospital PneumoniaDocument15 pagesHospital Pneumoniarivai anwarNo ratings yet
- Respiratory Tract Virus Infections in The Elderly With PneumoniaDocument11 pagesRespiratory Tract Virus Infections in The Elderly With PneumoniatanyasisNo ratings yet
- Guideline 133FM PDFDocument13 pagesGuideline 133FM PDFPangestu DhikaNo ratings yet
- Woolfrey2012 PDFDocument22 pagesWoolfrey2012 PDFJorge BarriosNo ratings yet
- CAP - PrinaDocument12 pagesCAP - PrinaSalNo ratings yet
- Management of Pneumonia in Critically Ill Patients: Catia Cillóniz, Antoni Torres, Michael S NiedermanDocument24 pagesManagement of Pneumonia in Critically Ill Patients: Catia Cillóniz, Antoni Torres, Michael S NiedermanMarvin Josue Bustamante GutierrezNo ratings yet
- IDSA Guideline PDFDocument80 pagesIDSA Guideline PDFArifHidayatNo ratings yet
- Infection ControlDocument12 pagesInfection ControlJules FillyNo ratings yet
- Tuberculous Meningitis: A Narrative ReviewDocument10 pagesTuberculous Meningitis: A Narrative ReviewVyom BuchNo ratings yet
- Id2019b2 SampleDocument21 pagesId2019b2 SampleSheikh FaishalNo ratings yet
- VAP PreventionDocument8 pagesVAP PreventionstarykNo ratings yet
- National Tuberculosis ProgramDocument37 pagesNational Tuberculosis ProgramDon Oliveros ÜNo ratings yet
- Hospital Aquired Pneumonia - FullDocument26 pagesHospital Aquired Pneumonia - FullSuvad Dedic100% (1)
- Infectious Diseases - Infective EndocarditisDocument41 pagesInfectious Diseases - Infective Endocarditisfire_n_iceNo ratings yet
- British Thoracic Society Guideline For The Management of Nontuberculous Mycobacterial Pulmonary Disease (NTM-PD) 2017Document13 pagesBritish Thoracic Society Guideline For The Management of Nontuberculous Mycobacterial Pulmonary Disease (NTM-PD) 2017Magaly Esteban GonzalesNo ratings yet
- Dengue GCP Guidelines 2020Document157 pagesDengue GCP Guidelines 2020Nido MalghaniNo ratings yet
- Hypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesDocument51 pagesHypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesskchhabraNo ratings yet
- Antimicrobial StewardshipDocument7 pagesAntimicrobial StewardshipMehwish MughalNo ratings yet
- Surveillance AssignmentDocument8 pagesSurveillance AssignmentPalwasha KhanNo ratings yet
- 05 Campbell LendrumDocument27 pages05 Campbell Lendrummaulia afidahNo ratings yet
- Fungal Infections in Immunocompromised HostsDocument214 pagesFungal Infections in Immunocompromised HostsОлечка Н.No ratings yet
- Community-Acquired Pneumonia (CAP) : Why FocusDocument4 pagesCommunity-Acquired Pneumonia (CAP) : Why FocusYoni KomalasariNo ratings yet
- Epid 600 Homework 7Document5 pagesEpid 600 Homework 7api-458165379No ratings yet
- Use of Surfactant Beyond Respiratory Distress Syndrome, What IsDocument10 pagesUse of Surfactant Beyond Respiratory Distress Syndrome, What Issam2000samNo ratings yet
- Molecular Epidemiology of Infectious DiseasesDocument58 pagesMolecular Epidemiology of Infectious DiseasesStan LamNo ratings yet
- Pneumonia: Recent Evidence Based UpdatesDocument30 pagesPneumonia: Recent Evidence Based UpdatesAli AzamNo ratings yet
- Ciy 866Document47 pagesCiy 866Skripsi ulmNo ratings yet
- Carbapenem-Resistant Pseudomonas Aeruginosa Strains ADocument9 pagesCarbapenem-Resistant Pseudomonas Aeruginosa Strains ACESAR ANTONIO ARTEAGA BENITESNo ratings yet
- Prevalence and Pattern of Maternal Malaria in Owerri, NigeriaDocument8 pagesPrevalence and Pattern of Maternal Malaria in Owerri, Nigeriaijmb333No ratings yet
- TB Guideline TreatmentDocument14 pagesTB Guideline TreatmentNovii NoviiNo ratings yet
- Trypanosoma Brucei: by Christian Jay N. BacantoDocument12 pagesTrypanosoma Brucei: by Christian Jay N. BacantoCHRISTIAN JAY BACANTONo ratings yet
- 2013 Sepsis GuidelinesDocument58 pages2013 Sepsis GuidelinesMuhd Azam100% (1)
- Pseudomonas Aeruginosa - Pathogenesis and Pathogenic MechanismsDocument24 pagesPseudomonas Aeruginosa - Pathogenesis and Pathogenic MechanismsFitryNo ratings yet
- TB PosterDocument1 pageTB PosterSucie 1997No ratings yet
- Conservative and Surgical Modalities in The Management of Pediatric Parapneumonic Effusion and EmpyemaDocument14 pagesConservative and Surgical Modalities in The Management of Pediatric Parapneumonic Effusion and EmpyemaPamela JumpNo ratings yet
- Prevention of Central Line-Associated Bloodstream Infections: Brief Update Review - Making Health Care Safer II - NCBI BookshelfDocument20 pagesPrevention of Central Line-Associated Bloodstream Infections: Brief Update Review - Making Health Care Safer II - NCBI Bookshelfmilove4uNo ratings yet
- MDR GNR PreventionDocument45 pagesMDR GNR Preventiondjdiek100% (1)
- Pseudomonas Infection ControlDocument15 pagesPseudomonas Infection Controlmariafernandasv98No ratings yet
- Adverse Medication Response Recorded in A Referral Health Facility: An Observational StudyDocument6 pagesAdverse Medication Response Recorded in A Referral Health Facility: An Observational StudyInternational Journal of Innovative Science and Research Technology100% (1)
- Multidrug Resistant Gram Negative BacteriaDocument6 pagesMultidrug Resistant Gram Negative BacteriaAniAliciaOrtizCastleNo ratings yet
- Wuhan Coronavirus 2020 Protecting Practical Guide The Updated Rational & Concise Guide From The Covid-19 Prevent Home, Work, Or Commuting / TravelingFrom EverandWuhan Coronavirus 2020 Protecting Practical Guide The Updated Rational & Concise Guide From The Covid-19 Prevent Home, Work, Or Commuting / TravelingNo ratings yet
- Diagnostic Imaging of Infections and Inflammatory Diseases: A Multidiscplinary ApproachFrom EverandDiagnostic Imaging of Infections and Inflammatory Diseases: A Multidiscplinary ApproachNo ratings yet
- Therapeutic Hypothermia - Principles, Indications, Practical ApplicationFrom EverandTherapeutic Hypothermia - Principles, Indications, Practical ApplicationNo ratings yet
- Antibiotics 11 01291Document8 pagesAntibiotics 11 01291semaraNo ratings yet
- PAVM em Terapia IntensivaDocument10 pagesPAVM em Terapia IntensivaVictor Hugo SilveiraNo ratings yet
- 1 s2.0 S0196655316303431 MainDocument5 pages1 s2.0 S0196655316303431 Mainzlatina.dobreva94No ratings yet
- Four-Month Rifapentine Regimens With or Without Moxifloxacin For TuberculosisDocument14 pagesFour-Month Rifapentine Regimens With or Without Moxifloxacin For TuberculosisyanaNo ratings yet
- 1 s2.0 S0924857924001845 MainDocument11 pages1 s2.0 S0924857924001845 MainHector Alejandro Holguin YepesNo ratings yet
- Pseudomonas Aeruginosa2019revista de Acceso Abierto de Investigacin Mdica InternacionalDocument12 pagesPseudomonas Aeruginosa2019revista de Acceso Abierto de Investigacin Mdica InternacionalValentina RondonNo ratings yet
- Piperacillin/tazobactam Vs Carbapenems For Patients With Bacterial Infection: Protocol For A Systematic ReviewDocument6 pagesPiperacillin/tazobactam Vs Carbapenems For Patients With Bacterial Infection: Protocol For A Systematic Reviewyhojan4No ratings yet
- ContentServer - Asp 2Document13 pagesContentServer - Asp 2Nanda Nurdara TaharaNo ratings yet
- Risk Factors For Healthcare-Associated Infection Caused by Carbapenem-Resistant Pseudomonas AeruginosaDocument8 pagesRisk Factors For Healthcare-Associated Infection Caused by Carbapenem-Resistant Pseudomonas AeruginosaUjjwal kumarNo ratings yet
- 1 s2.0 S1201971220302617 MainDocument7 pages1 s2.0 S1201971220302617 MainFaizah ShabrinaNo ratings yet
- Jamainternal Chanderraj 2024 Oi 240014 1719497546.29238Document9 pagesJamainternal Chanderraj 2024 Oi 240014 1719497546.29238Daniel MoralesNo ratings yet
- 16 RaDocument10 pages16 RaNitish TankNo ratings yet
- Comparative Efficacy of Doripenem Versus MeropenemDocument8 pagesComparative Efficacy of Doripenem Versus MeropenemaamirNo ratings yet
- Epidemology Pravctical Questions NR 1Document34 pagesEpidemology Pravctical Questions NR 1Adeeba AshrafNo ratings yet
- Sithind001 - Use Hygienic Practices For Hospitality ServiceDocument2 pagesSithind001 - Use Hygienic Practices For Hospitality ServiceYenna Tan100% (1)
- Chikungunya - DINKES - RS UNAIR 22 November 2017Document24 pagesChikungunya - DINKES - RS UNAIR 22 November 2017Mojo PuskesmasNo ratings yet
- Microbiology Question Paper MidtermDocument2 pagesMicrobiology Question Paper MidtermPoonam khanapurkarNo ratings yet
- Introduction To MicrobiologyDocument211 pagesIntroduction To MicrobiologyGaurav JoshiNo ratings yet
- Salmonella NTS VibrioDocument106 pagesSalmonella NTS VibrioSohil KisanNo ratings yet
- ConidiogenesisDocument5 pagesConidiogenesisHendra S BackNo ratings yet
- Myocarditisandpericarditis: Philip Hunter Spotts,, Fan ZhouDocument14 pagesMyocarditisandpericarditis: Philip Hunter Spotts,, Fan Zhoumiltoncaballero5No ratings yet
- Harmening Chapter 14Document23 pagesHarmening Chapter 14I love dem Coffee (Migz)No ratings yet
- Pulpal NecrosisDocument4 pagesPulpal NecrosisdevitaniaNo ratings yet
- Protocolos Minnesota Piel ATBDocument8 pagesProtocolos Minnesota Piel ATBDaniel Alejandro CastrilloNo ratings yet
- course spec 2018 طفيليات معهد فني معاملDocument7 pagescourse spec 2018 طفيليات معهد فني معاملhanan modaNo ratings yet
- Mathematical Model For Malaria Transmission Dynamics in Human and Mosquito Populations With Nonlinear Forces of InfectionDocument32 pagesMathematical Model For Malaria Transmission Dynamics in Human and Mosquito Populations With Nonlinear Forces of InfectionAshimi Blessing AyindeNo ratings yet
- Texas Health Presbyterian Hospital Dallas Ebola Diagnosis StatementDocument2 pagesTexas Health Presbyterian Hospital Dallas Ebola Diagnosis StatementJason Sickles, Yahoo News100% (1)
- Tenzin Dolma Lama 120351101Document7 pagesTenzin Dolma Lama 120351101Tenzin DolmaNo ratings yet
- Inglês Médico - Aula 01Document26 pagesInglês Médico - Aula 01Leandro Teixeira dos SantosNo ratings yet
- Protists FungiDocument77 pagesProtists FungiEgga AndiniNo ratings yet
- Communicable DiseasesDocument8 pagesCommunicable DiseasesKarla Fralala100% (1)
- The Impact of Vaccination Programs On The Prevention of Infectious Disease Tuberculosis: A Case Study With Gasabo District in RwandaDocument50 pagesThe Impact of Vaccination Programs On The Prevention of Infectious Disease Tuberculosis: A Case Study With Gasabo District in RwandaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Peds ?Document51 pagesPeds ?gissy0522No ratings yet
- Pagwawasto Materyal CopyreadingDocument7 pagesPagwawasto Materyal CopyreadingMary Williams100% (6)
- Solved MCQ For Upsc and MD Entrance Examination in Homeopathy 9788131911662Document22 pagesSolved MCQ For Upsc and MD Entrance Examination in Homeopathy 9788131911662goresamiksha310No ratings yet
- Using Bowel Nosodes ClinicallyDocument33 pagesUsing Bowel Nosodes ClinicallyFuente DelavidaNo ratings yet
- SESSION 2021-22: Chemistry Investigatory ProjectDocument14 pagesSESSION 2021-22: Chemistry Investigatory ProjectsaharyaNo ratings yet
- Derma DR HanadiDocument37 pagesDerma DR HanadiHassan Musadaq HamzahNo ratings yet
- Daftar PustakaDocument4 pagesDaftar Pustaka1906199425101991No ratings yet
- Developed by Cheryl McConnell RN MSNDocument17 pagesDeveloped by Cheryl McConnell RN MSNArva Glazel Defensor GallofinNo ratings yet
- Acquired Imm and Infection - BPTDocument15 pagesAcquired Imm and Infection - BPTKathal 66No ratings yet