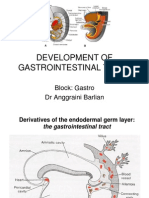
Embryology of Digestive System
Embryology of Digestive System
Download as pdf or txt
You might also like
- New Holland E18SR Mini Crawler Excavator Service Repair ManualDocument21 pagesNew Holland E18SR Mini Crawler Excavator Service Repair ManualggjjjjotonesNo ratings yet
- Digestive System EmbryologyDocument104 pagesDigestive System EmbryologyAlistair WalkerNo ratings yet
- Development of Gastrointestinal TractDocument28 pagesDevelopment of Gastrointestinal TractSaif100% (1)
- Development of The GIT and Clinical ConsiderationsDocument56 pagesDevelopment of The GIT and Clinical Considerationsdrclive130No ratings yet
- Anat 4.5 GIT Embryology MelendresDocument5 pagesAnat 4.5 GIT Embryology Melendreslovelots1234No ratings yet
- Embriologi GastroDocument50 pagesEmbriologi GastroYeni100% (1)
- Histology of GITDocument58 pagesHistology of GITOlatomide OlaniranNo ratings yet
- Development of The Gi SystemDocument6 pagesDevelopment of The Gi SystemKingNo ratings yet
- Embryology of Digestive System1Document62 pagesEmbryology of Digestive System1Gina AnnisahNo ratings yet
- Embryo Development Ofthe GI SytermDocument11 pagesEmbryo Development Ofthe GI SytermKingNo ratings yet
- Week 4 Embryology Development of Gastrointestinal: DR Marselina TanDocument29 pagesWeek 4 Embryology Development of Gastrointestinal: DR Marselina TanMaria Dini AdmiratiNo ratings yet
- Embryology and Anatomy of The Gastrointestinal Tract NASPGHANDocument14 pagesEmbryology and Anatomy of The Gastrointestinal Tract NASPGHANOana OanapNo ratings yet
- DR - Eftekhar Shamkhee Abbood Senior Lecturer Obstetrician and Gynecologist M.B.Ch.B/Cabog Ibn-Sina University of Medical and Pharmaceutical SciencesDocument26 pagesDR - Eftekhar Shamkhee Abbood Senior Lecturer Obstetrician and Gynecologist M.B.Ch.B/Cabog Ibn-Sina University of Medical and Pharmaceutical Sciencesرلا رةنNo ratings yet
- Development of Gut Tube Fore GutDocument52 pagesDevelopment of Gut Tube Fore GutSusan SarkerNo ratings yet
- Digestive SystemDocument6 pagesDigestive SystemDorence SimuntalaNo ratings yet
- Embriology of Digestive System: by Rita RositaDocument30 pagesEmbriology of Digestive System: by Rita Rositacendy_prastiwiNo ratings yet
- Embryology Lecture 8Document42 pagesEmbryology Lecture 8razanrazan978No ratings yet
- 17 - Development of Foregut-Derivatives and AnomaliesDocument22 pages17 - Development of Foregut-Derivatives and AnomaliesDr.B.B.GosaiNo ratings yet
- Development of Digestive and Respiratory SystemDocument48 pagesDevelopment of Digestive and Respiratory SystemFitria PuspariniNo ratings yet
- Yu - Git - Emb 1Document67 pagesYu - Git - Emb 1gtaha80No ratings yet
- The General Development Anatomy of Digestive SystemDocument60 pagesThe General Development Anatomy of Digestive Systemidris setyadi lubisNo ratings yet
- Embryology of GitDocument69 pagesEmbryology of Gititohowoubong37No ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document43 pagesClinical Embriology and Anatomy of Gi Tract Part1Luna LitamiNo ratings yet
- Development of GITDocument88 pagesDevelopment of GITBindiya MangarNo ratings yet
- Development of Digestive TractDocument14 pagesDevelopment of Digestive TractSulochan Ssplendid Splinterr LohaniNo ratings yet
- Development of GITDocument34 pagesDevelopment of GITWahida Amalin Ab RazakNo ratings yet
- Development of The Foregut and Midgut (Autosaved) (1) (Autosaved)Document45 pagesDevelopment of The Foregut and Midgut (Autosaved) (1) (Autosaved)zipporahwaithera404No ratings yet
- Digestive System-1Document19 pagesDigestive System-1asakingofhNo ratings yet
- Digestive System: - Primitive Gut (PG) Develops I From EndodermDocument24 pagesDigestive System: - Primitive Gut (PG) Develops I From EndodermRaju GangadharanNo ratings yet
- Gastrointestinal Tract EmbroyologyDocument55 pagesGastrointestinal Tract Embroyologywizarddone311No ratings yet
- Nahrain University - Abdomen - UPPER GIT ANATOMYDocument42 pagesNahrain University - Abdomen - UPPER GIT ANATOMYSalman KhanNo ratings yet
- Embryology GIT 1-1Document48 pagesEmbryology GIT 1-1gtaha80No ratings yet
- GIT EmbryologyDocument39 pagesGIT Embryologyqnz78swpjmNo ratings yet
- Embryology Course VIII - Digestive SystemDocument47 pagesEmbryology Course VIII - Digestive SystemRawa MuhsinNo ratings yet
- Digestive System (Part 2)Document21 pagesDigestive System (Part 2)alisalahaziz1No ratings yet
- ACCESORY ORGANS OF THE DIGESTIVE SYSTEM Contrast 1Document56 pagesACCESORY ORGANS OF THE DIGESTIVE SYSTEM Contrast 1Rea FloresNo ratings yet
- Pemicu 3 Blok GI AndreasDocument124 pagesPemicu 3 Blok GI AndreasEko SiswantoNo ratings yet
- Development of Gastrointestinal SystemDocument29 pagesDevelopment of Gastrointestinal SystemrifkaraihanaNo ratings yet
- GitDocument11 pagesGitM DAaud SAleemNo ratings yet
- Alimentary Tract.Document10 pagesAlimentary Tract.ghidjammal1234567890No ratings yet
- Development of Foregut 2-1Document34 pagesDevelopment of Foregut 2-1Çzãr MãlõñëNo ratings yet
- 3protected DuodenumDocument29 pages3protected Duodenumrdxbeast777No ratings yet
- Embryology GI TractDocument12 pagesEmbryology GI TractChrysanneNo ratings yet
- Pancreas - Endocrine and Exocrine Functions - Medical LibraryDocument16 pagesPancreas - Endocrine and Exocrine Functions - Medical Libraryjean PiedraNo ratings yet
- Yu - Git - Emb 2Document56 pagesYu - Git - Emb 2gtaha80No ratings yet
- 5 MIDGUT ReportingDocument18 pages5 MIDGUT ReportingMaster MastrikerNo ratings yet
- G & D Lecture 9 Development of The Gi System Part 2 Spring 2018Document42 pagesG & D Lecture 9 Development of The Gi System Part 2 Spring 2018John H. SolomonNo ratings yet
- Abdominal VisceraDocument4 pagesAbdominal ViscerazahraaNo ratings yet
- Git 301 Final 2021 Section TwoDocument8 pagesGit 301 Final 2021 Section TwoBright LunetaNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document44 pagesClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- АНГЛ - аномалии ЖКТ (1) .pptx - 20231025 - 013316 - 0000Document11 pagesАНГЛ - аномалии ЖКТ (1) .pptx - 20231025 - 013316 - 0000waitingforyoupugaNo ratings yet
- Abdominal Wall Defects: Omphalocele vs. GastroschisisDocument15 pagesAbdominal Wall Defects: Omphalocele vs. GastroschisisSerag MonierNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFIndira Damar PangestuNo ratings yet
- 10 Embryology of the Digestive SystemDocument30 pages10 Embryology of the Digestive Systemanneasuquo00No ratings yet
- 4Document9 pages4Marielle Anne TuazonNo ratings yet
- Abdominal CavityDocument51 pagesAbdominal CavitybayennNo ratings yet
- Anatomi Gasttrointestinal FIXDocument79 pagesAnatomi Gasttrointestinal FIXEka TariganNo ratings yet
- Dr. Meidona - Development of Gastrointestinal System PDFDocument54 pagesDr. Meidona - Development of Gastrointestinal System PDFwkwkwkhhhhNo ratings yet
- LAB1MGDC1206.101 t179 15122008Document114 pagesLAB1MGDC1206.101 t179 15122008getsweetNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Lecture 7Document27 pagesLecture 7zahraaNo ratings yet
- Carcinogenesis 2Document100 pagesCarcinogenesis 2zahraaNo ratings yet
- EndocrineDocument6 pagesEndocrinezahraaNo ratings yet
- Lecture 3 2Document17 pagesLecture 3 2zahraaNo ratings yet
- Week 5 Histology PNSDocument3 pagesWeek 5 Histology PNSzahraaNo ratings yet
- Anatomy 3 Upper LimbsDocument5 pagesAnatomy 3 Upper LimbszahraaNo ratings yet
- Lecture 2 1Document31 pagesLecture 2 1zahraaNo ratings yet
- Lecture-11 The Endocrine SystemDocument36 pagesLecture-11 The Endocrine SystemzahraaNo ratings yet
- Abdominal VisceraDocument4 pagesAbdominal ViscerazahraaNo ratings yet
- Lab 13: Voltage MultipliersDocument16 pagesLab 13: Voltage MultipliersLorenzo MenichinoNo ratings yet
- Reheat-Regebnerative CycleDocument7 pagesReheat-Regebnerative CycleBenjamin MabuteNo ratings yet
- Project 1 - Hardware BasicsDocument10 pagesProject 1 - Hardware BasicsterryNo ratings yet
- Theories With Sample StudiesDocument8 pagesTheories With Sample StudiesJohn Michael SaturNo ratings yet
- Science: Quarter 2 - Module 1: Different Forms of EM WavesDocument23 pagesScience: Quarter 2 - Module 1: Different Forms of EM WavesEarl QuimsonNo ratings yet
- Verb Forms: Direct Speech Reported Speech Direct Speech Reported SpeechDocument2 pagesVerb Forms: Direct Speech Reported Speech Direct Speech Reported SpeechMarisa SilvaNo ratings yet
- Database Management Systems (DBMS)Document2 pagesDatabase Management Systems (DBMS)aditya.prakash.gupta.bloggingNo ratings yet
- Open Ended Exp DSPDocument55 pagesOpen Ended Exp DSPTilak shastriNo ratings yet
- Ba Sar2 07 16 Ac2 Nonin Parallel en PDFDocument92 pagesBa Sar2 07 16 Ac2 Nonin Parallel en PDFQuoc HungNo ratings yet
- Session 06Document51 pagesSession 06Michael RahmeNo ratings yet
- Ultrasonic Diffraction in LiquidsDocument5 pagesUltrasonic Diffraction in LiquidsSampriti ShomeNo ratings yet
- 19BCS2206 (Worksheet 3.1)Document5 pages19BCS2206 (Worksheet 3.1)NIKHIL SHARMANo ratings yet
- Radiant Tube Heating StripDocument9 pagesRadiant Tube Heating StripSajib Chandra RoyNo ratings yet
- Volumetric Analysis - 1Document2 pagesVolumetric Analysis - 1Rajesh MishraNo ratings yet
- Sugino Selfeeder Servo Series Catalog 2613EDocument13 pagesSugino Selfeeder Servo Series Catalog 2613EweeraponglunbutNo ratings yet
- Scalar VisualizationDocument46 pagesScalar VisualizationSeshadri Venkata KrishnaNo ratings yet
- CT MMB 732Document9 pagesCT MMB 732Mohd MushahidNo ratings yet
- NukeSurvivalToolkit NewToolsHighlights Release v1.1.0Document14 pagesNukeSurvivalToolkit NewToolsHighlights Release v1.1.0Nicolás Díaz RodríguezNo ratings yet
- IACS Req Pipes Pressure VesselDocument69 pagesIACS Req Pipes Pressure VesselFrancesco CauzNo ratings yet
- Fuel Rail Pressure, CheckingDocument3 pagesFuel Rail Pressure, Checkinghanafi yusuf100% (1)
- Tendons - Basic Science - OrthobulletsDocument1 pageTendons - Basic Science - OrthobulletsHusein AhmadNo ratings yet
- MA313 Real and Complex Analysis: Sequences and Their Limits 2Document7 pagesMA313 Real and Complex Analysis: Sequences and Their Limits 2Piano FeaoNo ratings yet
- Dillimax 690 eDocument4 pagesDillimax 690 ePrabhakar TiwariNo ratings yet
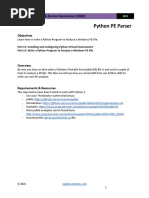
- Lab-02-Python PE ParserDocument4 pagesLab-02-Python PE Parseroscar tebarNo ratings yet
- Efficient Uses of Steam EnergyDocument67 pagesEfficient Uses of Steam EnergytojinboNo ratings yet
- Griswold Flowcon SM ActuatorDocument4 pagesGriswold Flowcon SM ActuatorBlack SmithNo ratings yet
- CTV p2p IptvDocument5 pagesCTV p2p IptvKaKang TrizNaNo ratings yet
- Pune MJP DSR 2018-19 PDFDocument398 pagesPune MJP DSR 2018-19 PDFsomnath rupnawar100% (1)
- JMRT Major Test-7 (English).648c988Document13 pagesJMRT Major Test-7 (English).648c988sahusaumya07No ratings yet