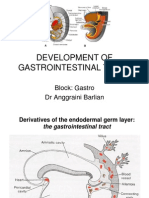
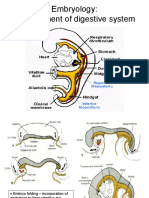
Development of Digestive and Respiratory System
Development of Digestive and Respiratory System
Download as ppt, pdf, or txt
You might also like
- Annual: PerformanceDocument176 pagesAnnual: PerformanceArja WoldeNo ratings yet
- Digestive System EmbryologyDocument104 pagesDigestive System EmbryologyAlistair WalkerNo ratings yet
- Anatomy Digestive SystemDocument5 pagesAnatomy Digestive Systemtimmieb_1No ratings yet
- Stimulation Therapy and Devices - Priority HealthDocument46 pagesStimulation Therapy and Devices - Priority Healthد.موسى التويتي100% (1)
- Development of Gastrointestinal TractDocument28 pagesDevelopment of Gastrointestinal TractSaif100% (1)
- DR - Eftekhar Shamkhee Abbood Senior Lecturer Obstetrician and Gynecologist M.B.Ch.B/Cabog Ibn-Sina University of Medical and Pharmaceutical SciencesDocument26 pagesDR - Eftekhar Shamkhee Abbood Senior Lecturer Obstetrician and Gynecologist M.B.Ch.B/Cabog Ibn-Sina University of Medical and Pharmaceutical Sciencesرلا رةنNo ratings yet
- Embryology of Digestive SystemDocument7 pagesEmbryology of Digestive SystemzahraaNo ratings yet
- Development of Digestive TractDocument14 pagesDevelopment of Digestive TractSulochan Ssplendid Splinterr LohaniNo ratings yet
- Development of The Gi SystemDocument6 pagesDevelopment of The Gi SystemKingNo ratings yet
- Histology of GITDocument58 pagesHistology of GITOlatomide OlaniranNo ratings yet
- Development of The GIT and Clinical ConsiderationsDocument56 pagesDevelopment of The GIT and Clinical Considerationsdrclive130No ratings yet
- Development of The Foregut and Midgut (Autosaved) (1) (Autosaved)Document45 pagesDevelopment of The Foregut and Midgut (Autosaved) (1) (Autosaved)zipporahwaithera404No ratings yet
- Embriology of Digestive System: by Rita RositaDocument30 pagesEmbriology of Digestive System: by Rita Rositacendy_prastiwiNo ratings yet
- Development of Gut Tube Fore GutDocument52 pagesDevelopment of Gut Tube Fore GutSusan SarkerNo ratings yet
- Embriologi GastroDocument50 pagesEmbriologi GastroYeni100% (1)
- GitDocument11 pagesGitM DAaud SAleemNo ratings yet
- Week 4 Embryology Development of Gastrointestinal: DR Marselina TanDocument29 pagesWeek 4 Embryology Development of Gastrointestinal: DR Marselina TanMaria Dini AdmiratiNo ratings yet
- Embryo Development Ofthe GI SytermDocument11 pagesEmbryo Development Ofthe GI SytermKingNo ratings yet
- The General Development Anatomy of Digestive SystemDocument60 pagesThe General Development Anatomy of Digestive Systemidris setyadi lubisNo ratings yet
- Development of Foregut 2-1Document34 pagesDevelopment of Foregut 2-1Çzãr MãlõñëNo ratings yet
- 72 Hours Chick EmbryoDocument18 pages72 Hours Chick EmbryoZhairra Marie DionsonNo ratings yet
- Development of The GI Tract and Respiratory SystemDocument7 pagesDevelopment of The GI Tract and Respiratory SystemZahidaNo ratings yet
- Digestive System (Part 2)Document21 pagesDigestive System (Part 2)alisalahaziz1No ratings yet
- 17 - Development of Foregut-Derivatives and AnomaliesDocument22 pages17 - Development of Foregut-Derivatives and AnomaliesDr.B.B.GosaiNo ratings yet
- GIT EmbryologyDocument39 pagesGIT Embryologyqnz78swpjmNo ratings yet
- Anat 4.5 GIT Embryology MelendresDocument5 pagesAnat 4.5 GIT Embryology Melendreslovelots1234No ratings yet
- Embriologi PDFDocument97 pagesEmbriologi PDFbarbiemeNo ratings yet
- Digestive System: - Primitive Gut (PG) Develops I From EndodermDocument24 pagesDigestive System: - Primitive Gut (PG) Develops I From EndodermRaju GangadharanNo ratings yet
- Embryology and Anatomy of The Gastrointestinal Tract NASPGHANDocument14 pagesEmbryology and Anatomy of The Gastrointestinal Tract NASPGHANOana OanapNo ratings yet
- Embryology Course VIII - Digestive SystemDocument47 pagesEmbryology Course VIII - Digestive SystemRawa MuhsinNo ratings yet
- Development of The Digestive SystemDocument71 pagesDevelopment of The Digestive SystembenmulengajrNo ratings yet
- Development of Body Cavities and Diaphragm: Pleuro-Pericardial and Pleuro-Peritoneal MembraneDocument14 pagesDevelopment of Body Cavities and Diaphragm: Pleuro-Pericardial and Pleuro-Peritoneal MembraneÑäd ÉèmNo ratings yet
- Gastrointestinal Tract EmbroyologyDocument55 pagesGastrointestinal Tract Embroyologywizarddone311No ratings yet
- DIgestive System EmbDocument85 pagesDIgestive System EmbDanish GujjarNo ratings yet
- Development of GITDocument34 pagesDevelopment of GITWahida Amalin Ab RazakNo ratings yet
- Embryology of Digestive System1Document62 pagesEmbryology of Digestive System1Gina AnnisahNo ratings yet
- Respiratory GIT Embryology (Esophagus, Stomach)Document37 pagesRespiratory GIT Embryology (Esophagus, Stomach)olomuoluwatobiNo ratings yet
- Development of GITDocument88 pagesDevelopment of GITBindiya MangarNo ratings yet
- Bio 102 Lec Notes 1Document3 pagesBio 102 Lec Notes 1Kevin ManuelNo ratings yet
- G & D Lecture 9 Development of The Gi System Part 2 Spring 2018Document42 pagesG & D Lecture 9 Development of The Gi System Part 2 Spring 2018John H. SolomonNo ratings yet
- Yu - Git - Emb 2Document56 pagesYu - Git - Emb 2gtaha80No ratings yet
- Development of Gastrointestinal SystemDocument29 pagesDevelopment of Gastrointestinal SystemrifkaraihanaNo ratings yet
- Digestive SystemDocument106 pagesDigestive SystemAuza Moses Ibrahim100% (2)
- Digestive System of PrawnDocument16 pagesDigestive System of Prawnyayeg raja100% (1)
- Yu - Git - Emb 1Document67 pagesYu - Git - Emb 1gtaha80No ratings yet
- First Page PDFDocument1 pageFirst Page PDFIndira Damar PangestuNo ratings yet
- Pemicu 3 Blok GI AndreasDocument124 pagesPemicu 3 Blok GI AndreasEko SiswantoNo ratings yet
- Endodermal Derivatives, Formation of The Gut and Its Subsequent RotationDocument14 pagesEndodermal Derivatives, Formation of The Gut and Its Subsequent RotationmikeNo ratings yet
- Digestive SystemDocument6 pagesDigestive SystemDorence SimuntalaNo ratings yet
- Lecture 4Document14 pagesLecture 4X RamboNo ratings yet
- ACCESORY ORGANS OF THE DIGESTIVE SYSTEM Contrast 1Document56 pagesACCESORY ORGANS OF THE DIGESTIVE SYSTEM Contrast 1Rea FloresNo ratings yet
- Development of Git Part 1 2024 (DR Shahnaj Pervin) Updated For UploadDocument49 pagesDevelopment of Git Part 1 2024 (DR Shahnaj Pervin) Updated For Uploadnikhilsilva7No ratings yet
- Dr. Meidona - Development of Gastrointestinal System PDFDocument54 pagesDr. Meidona - Development of Gastrointestinal System PDFwkwkwkhhhhNo ratings yet
- Development of Respiratory SDocument35 pagesDevelopment of Respiratory SMunewer AbdellaNo ratings yet
- .By Prof Faiz. Shaikh LCMD - Development of Body CavitiesDocument9 pages.By Prof Faiz. Shaikh LCMD - Development of Body Cavitiesumernadeem73.unNo ratings yet
- Intrauterine Development of Respiratory SystemDocument21 pagesIntrauterine Development of Respiratory SystemShubham KathareNo ratings yet
- Embryologi OF The Respiratory System: Arti Rosaria Dewi, DRDocument60 pagesEmbryologi OF The Respiratory System: Arti Rosaria Dewi, DRAsti NuriatiNo ratings yet
- Development of The Respiratory SystemDocument22 pagesDevelopment of The Respiratory SystemtuhinNo ratings yet
- 4Document9 pages4Marielle Anne TuazonNo ratings yet
- 3protected DuodenumDocument29 pages3protected Duodenumrdxbeast777No ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Observations on Abortion: Containing an account of the manner in which it is accomplished, the causes which produced it, and the method of preventing or treating itFrom EverandObservations on Abortion: Containing an account of the manner in which it is accomplished, the causes which produced it, and the method of preventing or treating itNo ratings yet
- TTSH AchievementsDocument50 pagesTTSH AchievementsTan Tock Seng HospitalNo ratings yet
- Nursing Care Plan of IonDocument1 pageNursing Care Plan of IonvhentesixNo ratings yet
- Prevalence of Escherichia Coli O157-H7 and Salmonella Spp. in Surface Waters of Southern Alberta and Its Relation To Manure SourcesDocument10 pagesPrevalence of Escherichia Coli O157-H7 and Salmonella Spp. in Surface Waters of Southern Alberta and Its Relation To Manure SourcesHMVMCNo ratings yet
- FANTASTIC Lifestyle AssessmentDocument6 pagesFANTASTIC Lifestyle AssessmentzacNo ratings yet
- Approaches in Values EducationDocument28 pagesApproaches in Values EducationMaye Zaidyle Borinaga100% (1)
- Break The Chain CampaignDocument2 pagesBreak The Chain CampaignAnju PrakashNo ratings yet
- Neck PainDocument2 pagesNeck PainfrentomegaNo ratings yet
- Pat 202Document7 pagesPat 202Anto RashwinNo ratings yet
- GSO 1016-2000 STD Microbiological Criteria For Food Stuffs - Part 1Document25 pagesGSO 1016-2000 STD Microbiological Criteria For Food Stuffs - Part 1Mm. Sharaby100% (2)
- Alzheimer Clinical DiagnosisDocument13 pagesAlzheimer Clinical DiagnosisClarissa Castro RodríguezNo ratings yet
- Exp. 9 Test For Vitamin CDocument5 pagesExp. 9 Test For Vitamin CEdchelNo ratings yet
- Diabetes Mellitus by BaddiriDocument34 pagesDiabetes Mellitus by BaddiriJason AbudaNo ratings yet
- 08 BuffferDocument7 pages08 BuffferSaid Nafik HkiNo ratings yet
- Fever With RashDocument78 pagesFever With RashRiyan AgusNo ratings yet
- DMC FinalsDocument64 pagesDMC Finalskaye agustinNo ratings yet
- Lesson Plan On HRTDocument22 pagesLesson Plan On HRTArjumand ZargarNo ratings yet
- AcupunctureDocument11 pagesAcupunctureVenkat TNo ratings yet
- Titcomb CV Feb2021 WebsiteDocument9 pagesTitcomb CV Feb2021 Websiteapi-215083347No ratings yet
- White Paper On Food SafetyDocument52 pagesWhite Paper On Food SafetyLuvonga CalebNo ratings yet
- Epididymoorchitis PDFDocument6 pagesEpididymoorchitis PDFdidiNo ratings yet
- Gram-Stain LASTDocument63 pagesGram-Stain LASTBea Francine MercadoNo ratings yet
- 57 4 2 BiologyDocument24 pages57 4 2 BiologytejNo ratings yet
- Alterations in Pediatric Neurological Function: Lisa Musso, ARNP, MN, CPNP Seattle UniversityDocument66 pagesAlterations in Pediatric Neurological Function: Lisa Musso, ARNP, MN, CPNP Seattle Universityfadumo65No ratings yet
- Lecture 8Document13 pagesLecture 8jmanuelNo ratings yet
- Pediatric Dysphagia Management in The SchoolsDocument38 pagesPediatric Dysphagia Management in The SchoolsdikaNo ratings yet
- Mechanism of Action Adverse/Side Effects Nursing Consideration Folic AcidDocument4 pagesMechanism of Action Adverse/Side Effects Nursing Consideration Folic AcidjajalerNo ratings yet
- Articulo Masas en MediatinoDocument6 pagesArticulo Masas en MediatinoLarryftRubenNo ratings yet
- Bhutanese Journal of Agriculture 1 1 PDFDocument157 pagesBhutanese Journal of Agriculture 1 1 PDFMalcolmNo ratings yet