Mullin 2007
Mullin 2007
Download as pdf or txt
You might also like
- Anorectal MalformationsDocument28 pagesAnorectal MalformationsVisu ReddyNo ratings yet
- Anorectal MalformationDocument28 pagesAnorectal MalformationJaya Prabha33% (3)
- Intestine ObstructionDocument37 pagesIntestine ObstructionGoesti YudistiraNo ratings yet
- Moisture Content AOAC 984.20 PDFDocument74 pagesMoisture Content AOAC 984.20 PDFWynona Basilio100% (1)
- Reflections On The Prayer of ST Francis of AssisiDocument6 pagesReflections On The Prayer of ST Francis of AssisiRicky Aguilar100% (1)
- 03 US Alteraciones Congenitas RiñonDocument7 pages03 US Alteraciones Congenitas RiñonDonaldo ReleyNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFdr.rahmanNo ratings yet
- Xv-B.pathologic Fetal Kidneys 2017Document8 pagesXv-B.pathologic Fetal Kidneys 2017jamiladeguzmanabcdefghijklmNo ratings yet
- Management of Common Benign Anorectal Disease: What All Physicians Need To KnowDocument7 pagesManagement of Common Benign Anorectal Disease: What All Physicians Need To KnowNeri JaramilloNo ratings yet
- Abnormalities of The Abdominal Wall and GenitaliaDocument51 pagesAbnormalities of The Abdominal Wall and GenitaliaJaser YaminNo ratings yet
- PIIS0002937821006761Document3 pagesPIIS0002937821006761tasnishapeer15No ratings yet
- 20 - Pediatric Urinary DisordersDocument62 pages20 - Pediatric Urinary DisordersKhaalid AbdirahmanNo ratings yet
- Anorectal MalformationDocument28 pagesAnorectal Malformationsulithkuriakose100% (2)
- Management ofARM&HSD 1Document54 pagesManagement ofARM&HSD 1Hayle MaryamNo ratings yet
- New Developments in Anal Surgery Congenital Ano RectalDocument5 pagesNew Developments in Anal Surgery Congenital Ano RectalOctavianus KevinNo ratings yet
- Nizzah Gus Idk1 EpispadiasDocument22 pagesNizzah Gus Idk1 EpispadiasLuthfan Dio Satria BachriNo ratings yet
- Paediatric Surgery Recal- Dr Raghul.MDocument86 pagesPaediatric Surgery Recal- Dr Raghul.MFirst FoundationNo ratings yet
- Anorectal MalformationDocument4 pagesAnorectal MalformationFawzia Haznah Nurul ImaniNo ratings yet
- 2.4.5.2.3.a Bowel ObstructionDocument35 pages2.4.5.2.3.a Bowel ObstructionProject ByNo ratings yet
- Intestinal Pathology III Hirschsprung'S Disease: DR Nzau MuangeDocument21 pagesIntestinal Pathology III Hirschsprung'S Disease: DR Nzau MuangeNzau MuangeNo ratings yet
- Approach To Fetal AnomaliesDocument38 pagesApproach To Fetal Anomaliesamq aloqiliNo ratings yet
- Surgical Problems in ChildrenDocument56 pagesSurgical Problems in ChildrenHugh McGregorNo ratings yet
- Operative Pediatric Surgery Anorectal MalformationDocument21 pagesOperative Pediatric Surgery Anorectal MalformationZaeem KhalidNo ratings yet
- Vascular AccententDocument2 pagesVascular Accententwp4saleNo ratings yet
- Umbilical Varices A Twisted TaleDocument1 pageUmbilical Varices A Twisted TaleAnurisha AsokanNo ratings yet
- Imperforate Hymen Complicated by Obstructive Acute Renal FailureDocument3 pagesImperforate Hymen Complicated by Obstructive Acute Renal FailureQonny WelendriNo ratings yet
- Anorectal MalformationsDocument19 pagesAnorectal MalformationsJumrotun Ni'mahNo ratings yet
- TAP 20230090 NLM New InddDocument8 pagesTAP 20230090 NLM New InddYusuf HardiNo ratings yet
- Anorectalmalformations2 PDFDocument1 pageAnorectalmalformations2 PDFIlham Nyssam AkbarNo ratings yet
- Chapter 341.5 - Other Conditions in PancreatitisDocument1 pageChapter 341.5 - Other Conditions in Pancreatitistubaeker1101No ratings yet
- BR Feto I IYADocument21 pagesBR Feto I IYAshare fosNo ratings yet
- Appendicitis, HasDocument6 pagesAppendicitis, HasHasan MohammedNo ratings yet
- Case Report Rupture Ectopic Pregnancy With History of AppendectomyDocument3 pagesCase Report Rupture Ectopic Pregnancy With History of AppendectomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Anorectal Malformation New 2024Document34 pagesAnorectal Malformation New 2024Urologi RSunudNo ratings yet
- From Functional Imaging in Nephro-Urology (Alain Prigent Etc.) (Z-Library)Document10 pagesFrom Functional Imaging in Nephro-Urology (Alain Prigent Etc.) (Z-Library)Francisco BotelhoNo ratings yet
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNo ratings yet
- 2.obstruction of The Urinary TractDocument22 pages2.obstruction of The Urinary TractAkli JahNo ratings yet
- Gastrointestinal AbnormalitiesDocument69 pagesGastrointestinal AbnormalitiesJaser YaminNo ratings yet
- KelasDocument4 pagesKelasDyan Riza Indah TamiNo ratings yet
- Abdominal Pain in A Patient With Epistaxis, Telangiectasias, and Arteriovenous MalformationsDocument8 pagesAbdominal Pain in A Patient With Epistaxis, Telangiectasias, and Arteriovenous MalformationsUrgencias La RazaNo ratings yet
- HypospDocument39 pagesHypospyoussef.aziz2020No ratings yet
- Congenital Malformations of The Lower Urinary Tract (Without Images-2) - Mar 2012Document9 pagesCongenital Malformations of The Lower Urinary Tract (Without Images-2) - Mar 2012ibmreadywriterNo ratings yet
- Jurnal Atresia AniDocument4 pagesJurnal Atresia AnihumairohimaniaNo ratings yet
- Neonatal Surgical EmergenciesDocument17 pagesNeonatal Surgical EmergenciesfaisaldanyaniNo ratings yet
- Jurnal MAR 2Document10 pagesJurnal MAR 2Taufik HidayatNo ratings yet
- scrotal swellings pptDocument44 pagesscrotal swellings pptraman shrivastavaNo ratings yet
- Pediatric Surgery Notes For NursesDocument8 pagesPediatric Surgery Notes For NursesAhmed SamyNo ratings yet
- Screenshot 2022-05-30 at 9.43.21 PMDocument23 pagesScreenshot 2022-05-30 at 9.43.21 PMAZNo ratings yet
- Anorectal MalformationDocument6 pagesAnorectal MalformationMaryam AkmalNo ratings yet
- Appendicitis: Basic Information DiagnosisDocument5 pagesAppendicitis: Basic Information DiagnosisCarlos Meza HernandezNo ratings yet
- RenalDocument15 pagesRenalfarhathNo ratings yet
- Hydronephrosis in Children: Pelviureteric Junction DysfunctionDocument5 pagesHydronephrosis in Children: Pelviureteric Junction DysfunctionnadyajondriNo ratings yet
- 1 s2.0 S147751312100019X MainDocument7 pages1 s2.0 S147751312100019X MainJad DegheiliNo ratings yet
- Jurnal OG 1Document6 pagesJurnal OG 1Wa Ode Meutya ZawawiNo ratings yet
- 2018.surgery Intestinal Obstruction in Infants and ChildrenDocument11 pages2018.surgery Intestinal Obstruction in Infants and ChildrenFranz SalazarNo ratings yet
- Abdominal Wall DefectsDocument14 pagesAbdominal Wall Defectsskeebs23No ratings yet
- Appendicitis HasanDocument6 pagesAppendicitis HasanHasan MohammedNo ratings yet
- VARICOCELE A ReviewDocument7 pagesVARICOCELE A ReviewEka WarmandanaNo ratings yet
- Renal AbnormalitiesDocument15 pagesRenal AbnormalitiesShambel NegeseNo ratings yet
- Birth of Maggots9807Document3 pagesBirth of Maggots9807Kent Ronnel Ranque PilarNo ratings yet
- Stationary Crusher PlantDocument15 pagesStationary Crusher PlantMr. Slab100% (1)
- Calculate Your Ascendant Ascendants Astrology HomeDocument1 pageCalculate Your Ascendant Ascendants Astrology HomeDreamOn PlzNo ratings yet
- JBL Charge 3 ManualDocument6 pagesJBL Charge 3 ManualCharlesNo ratings yet
- English Class 9th, October TestDocument3 pagesEnglish Class 9th, October TestManjot DdcNo ratings yet
- HP Globe ValvesDocument20 pagesHP Globe ValvesSaadat BilalNo ratings yet
- Desilting Basin - TCSDocument4 pagesDesilting Basin - TCSManojPatne0% (1)
- Bio Deterioration of Historic Buildings and MonumentsDocument2 pagesBio Deterioration of Historic Buildings and MonumentsDarshi Thamali ParanagamaNo ratings yet
- SEA Maths 2009 PDFDocument28 pagesSEA Maths 2009 PDFJake DillonNo ratings yet
- Impressions Decennium 2022 - BrochureDocument12 pagesImpressions Decennium 2022 - BrochureJulianne A. JohnNo ratings yet
- Lightning Protection Systems Design For Substations by Using Masts and Matlab PDFDocument5 pagesLightning Protection Systems Design For Substations by Using Masts and Matlab PDFamitbheltbgNo ratings yet
- Brochure ReticlesDocument2 pagesBrochure ReticlesMYEMAIL6306100% (1)
- Windows BrochureDocument90 pagesWindows BrochureShivansh Singh GautamNo ratings yet
- Design and Simulation of Voltage Source Grid Connected Inverter (VSI)Document5 pagesDesign and Simulation of Voltage Source Grid Connected Inverter (VSI)hesham elrefaieNo ratings yet
- Talzat ZachariaDocument8 pagesTalzat ZachariaArun KumarNo ratings yet
- Correcting Heterogeneous and Biased Forecast Error at Intel For Supply Chain OptimizationDocument14 pagesCorrecting Heterogeneous and Biased Forecast Error at Intel For Supply Chain OptimizationIsabel Zanella ZancaNo ratings yet
- MJT314 RelayDocument4 pagesMJT314 Relaynkiruthigairaju100% (1)
- Lecture Notes On Cosmology (ns-tp430m) by Tomislav Prokopec Part I: An Introduction To The Einstein Theory of GravitationDocument37 pagesLecture Notes On Cosmology (ns-tp430m) by Tomislav Prokopec Part I: An Introduction To The Einstein Theory of GravitationEnzo SoLis GonzalezNo ratings yet
- Dindigul School of TNPSC: Development Administration in Tamil NaduDocument3 pagesDindigul School of TNPSC: Development Administration in Tamil NaduKaniNo ratings yet
- The Attraction DistractionDocument261 pagesThe Attraction DistractionsNo ratings yet
- Mechanics of Materials Lab Fall 2018Document52 pagesMechanics of Materials Lab Fall 2018Hammad RazaNo ratings yet
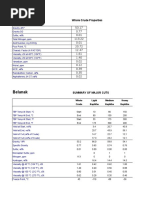
- Belanak: Whole Crude PropertiesDocument6 pagesBelanak: Whole Crude PropertiesHeron SurbaktiNo ratings yet
- PT1 Multi Function TransducerDocument4 pagesPT1 Multi Function TransducerDeepakNo ratings yet
- The Battery Technology Behind The Wheel: Kurt KeltyDocument41 pagesThe Battery Technology Behind The Wheel: Kurt KeltyFazle ElahiNo ratings yet
- Chapter 4 PDFDocument17 pagesChapter 4 PDFelias ferhanNo ratings yet
- KPI in LTE Radio NetworkDocument21 pagesKPI in LTE Radio NetworkkhawlaNo ratings yet
- Installation Manual 60x60 PDFDocument24 pagesInstallation Manual 60x60 PDFB YoungNo ratings yet
- Photoemission Optical BenchDocument2 pagesPhotoemission Optical Benchhobad57099No ratings yet