Administrative Order
Administrative Order
Download as pdf or txt
You might also like
- Hospital Nutrition and Dietetics Service Management Manual - Third EditionDocument398 pagesHospital Nutrition and Dietetics Service Management Manual - Third EditionDIVINE WORD HOSPITAL100% (10)
- Nursing Exam Questions 2023 Part 12Document2 pagesNursing Exam Questions 2023 Part 12Lejo SunnyNo ratings yet
- Project Proposal On Child Nutrition For Sustainable Health and Prenatal ClinicDocument6 pagesProject Proposal On Child Nutrition For Sustainable Health and Prenatal Clinicczeremar chan80% (5)
- AO 2009 0025 Essential Newborn CareDocument15 pagesAO 2009 0025 Essential Newborn Carejulesubayubay542895% (21)
- Mother and Baby Friendly Hospital Initiative - Session 15 MBFHDocument27 pagesMother and Baby Friendly Hospital Initiative - Session 15 MBFHthirdielacorte75% (4)
- To Ensure That Mother-Baby Friendly Hospital Initiative Program IsDocument6 pagesTo Ensure That Mother-Baby Friendly Hospital Initiative Program IsGlenn L. Ravanilla100% (1)
- Obg-Assignment On Family Welfare ServicesDocument20 pagesObg-Assignment On Family Welfare ServicesRashmi C S80% (10)
- Legal Mandates Related To Nutrition and Diet TherapyDocument2 pagesLegal Mandates Related To Nutrition and Diet TherapyMarielle Chua50% (4)
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- Breast Feeding ProgramDocument2 pagesBreast Feeding ProgramCandice AlincastreNo ratings yet
- Essential Newborn Care PowerpointDocument35 pagesEssential Newborn Care PowerpointKrystal Tan100% (2)
- E Inc PoliciesDocument2 pagesE Inc PoliciesricogeminaNo ratings yet
- Operational Guide Enhancing Optimal Infant and Young Child Feeding Practices Through The Public Health SystemDocument70 pagesOperational Guide Enhancing Optimal Infant and Young Child Feeding Practices Through The Public Health SystemJennifer Pearson-ParedesNo ratings yet
- Irr - Ra 10028Document17 pagesIrr - Ra 10028Noel Cagigas FelongcoNo ratings yet
- CPM16TH Intrapartum and Immediate Postpartum CareDocument25 pagesCPM16TH Intrapartum and Immediate Postpartum CarespringdingNo ratings yet
- Essential Newborn CareDocument3 pagesEssential Newborn CareSheene Ainasthazia Diego AngNo ratings yet
- CPG Intrapartum and Immediate Postpartum Care PDFDocument52 pagesCPG Intrapartum and Immediate Postpartum Care PDFAngela SaldajenoNo ratings yet
- Maternal, Child and Adolescent Health Services: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorDocument32 pagesMaternal, Child and Adolescent Health Services: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorLawrence Ryan DaugNo ratings yet
- Newborn Care Until The First Week of LifeDocument66 pagesNewborn Care Until The First Week of LifeJan Audan100% (1)
- MaternalDocument8 pagesMaternalMarie Claire CacalNo ratings yet
- Nutrition Programs Report.pdfDocument33 pagesNutrition Programs Report.pdfJan herald FernandezNo ratings yet
- Maternal and Child CareDocument6 pagesMaternal and Child CareArizz Tia BaquinquitoNo ratings yet
- Clinical Practice Guidelines Einc 2014Document52 pagesClinical Practice Guidelines Einc 2014dennisreveni100% (1)
- PostPartum Family Planning PDFDocument34 pagesPostPartum Family Planning PDFRyan Michael OducadoNo ratings yet
- Bemoc GuideDocument193 pagesBemoc GuideCindy Rose MisenaNo ratings yet
- CHNDocument7 pagesCHNCient Mae D. QuilonaNo ratings yet
- AO 2008-0029 Rapid Reduction of Maternal and Neonatal MortalityDocument13 pagesAO 2008-0029 Rapid Reduction of Maternal and Neonatal MortalitygiogmailNo ratings yet
- Ao2008 0029 PDFDocument13 pagesAo2008 0029 PDFCacapablen GinNo ratings yet
- Bfhi NotesDocument13 pagesBfhi NotesJyothi Singh SuryavanshiNo ratings yet
- Reproductive and Child Health ProgrammeDocument10 pagesReproductive and Child Health ProgrammeMebin NinanNo ratings yet
- IPNAP Position Paper Updated 01 Mar 2011Document18 pagesIPNAP Position Paper Updated 01 Mar 2011Stephanie PeNo ratings yet
- Ra 7600 PDFDocument5 pagesRa 7600 PDFanorith88No ratings yet
- ThesisDocument45 pagesThesisSonny Aguilar100% (4)
- Rooming in ActDocument5 pagesRooming in ActShaira EddingNo ratings yet
- Reproductive and Child Health ProgramDocument34 pagesReproductive and Child Health Programjissy paulNo ratings yet
- Clinical Guidelines: PMTCT (Prevention of Mother-to-Child Transmission)Document43 pagesClinical Guidelines: PMTCT (Prevention of Mother-to-Child Transmission)Achmad Shiddiq100% (1)
- Rhii. Save MotherhoodDocument11 pagesRhii. Save MotherhoodmahmudbebejiNo ratings yet
- Essential Intrapartum Newborn CareDocument10 pagesEssential Intrapartum Newborn Careacuna27cielsiNo ratings yet
- PostPartum Family PlanningDocument34 pagesPostPartum Family Planning9gyvngf9gkNo ratings yet
- Breast Feeding GuidelinesDocument18 pagesBreast Feeding GuidelinesAdelle SmithNo ratings yet
- Chn Notes Ch13Document6 pagesChn Notes Ch132083120No ratings yet
- Provision of Child Health Care 2010Document50 pagesProvision of Child Health Care 2010Nour AhmededNo ratings yet
- "Maternity", 1963, © 2003 Estate of Pablo Picasso/Artists Rights Society (ARS), New YorkDocument12 pages"Maternity", 1963, © 2003 Estate of Pablo Picasso/Artists Rights Society (ARS), New YorkteabagmanNo ratings yet
- PHL MN 67 01 Law 1992 Eng Rooming in Breast Feeding Act 1992Document4 pagesPHL MN 67 01 Law 1992 Eng Rooming in Breast Feeding Act 1992mclairedenniseNo ratings yet
- Baby Friendly Hospital Initiatives (Bfhi) IntroductionDocument12 pagesBaby Friendly Hospital Initiatives (Bfhi) Introductionjyoti singhNo ratings yet
- World Health Organization, Global Strategy For Infant and Young Child Feeding, 5 (2003)Document4 pagesWorld Health Organization, Global Strategy For Infant and Young Child Feeding, 5 (2003)Roizki Edward MarquezNo ratings yet
- RA 7600 The Rooming-In and Breastfeeding Act of 1992Document4 pagesRA 7600 The Rooming-In and Breastfeeding Act of 1992yeddayadao123No ratings yet
- Seminar ON: Baby Friendly Hospital InitiativeDocument7 pagesSeminar ON: Baby Friendly Hospital InitiativeUmairah BashirNo ratings yet
- Seminar ON: Baby Friendly Hospital InitiativeDocument7 pagesSeminar ON: Baby Friendly Hospital InitiativeUmairah BashirNo ratings yet
- Seminar ON: Baby Friendly Hospital InitiativeDocument7 pagesSeminar ON: Baby Friendly Hospital InitiativeUmairah BashirNo ratings yet
- BFHIDocument5 pagesBFHISangita DebNo ratings yet
- National Health and Family Welfare ProgrammesDocument17 pagesNational Health and Family Welfare ProgrammesSandhya s75% (4)
- MCN Lab WRDocument101 pagesMCN Lab WRMaui TabuzoNo ratings yet
- Predictors of Knowledge and Practice of Exclusive Breastfeeding Among Health Workers in Mwanza City, Northwest TanzaniaDocument8 pagesPredictors of Knowledge and Practice of Exclusive Breastfeeding Among Health Workers in Mwanza City, Northwest TanzaniaDessy WahyuniNo ratings yet
- NDOH - PMTCT Apr 2008Document43 pagesNDOH - PMTCT Apr 2008fosuahlucy685No ratings yet
- Family Nutrition GuideFrom EverandFamily Nutrition GuideNo ratings yet
- Well-Child Care in Infancy: Promoting Readiness for LifeFrom EverandWell-Child Care in Infancy: Promoting Readiness for LifeNo ratings yet
- Healthy Schools, Healthy Lives: A Teacher's Guide to Tackling Childhood ObesityFrom EverandHealthy Schools, Healthy Lives: A Teacher's Guide to Tackling Childhood ObesityNo ratings yet
- Rizal 1 4Document108 pagesRizal 1 4Nathanyel Leigh MongosoNo ratings yet
- 2 Chapters 1 5 1Document149 pages2 Chapters 1 5 1Nathanyel Leigh MongosoNo ratings yet
- Nursing Procedures - SkillsDocument92 pagesNursing Procedures - SkillsNathanyel Leigh MongosoNo ratings yet
- Risk Factors For Pneumonia:: Cultural ConsiderationsDocument9 pagesRisk Factors For Pneumonia:: Cultural ConsiderationsNathanyel Leigh MongosoNo ratings yet
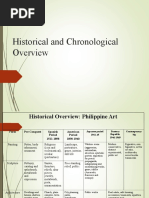
- Chronological Overview Phil ArtDocument4 pagesChronological Overview Phil ArtNathanyel Leigh MongosoNo ratings yet
- Risk Factors For Pneumonia:: Cultural ConsiderationsDocument9 pagesRisk Factors For Pneumonia:: Cultural ConsiderationsNathanyel Leigh MongosoNo ratings yet
- Citronella Shower Jelly: Citronell A SoapDocument1 pageCitronella Shower Jelly: Citronell A SoapNathanyel Leigh MongosoNo ratings yet
- FNCP SampleDocument2 pagesFNCP SampleNathanyel Leigh MongosoNo ratings yet
- 503060Document3 pages503060Nathanyel Leigh MongosoNo ratings yet
- Nona D. Andaya-Castillo, IBCLC International Board Certified Lactation Consultant Director, Nurturers of The EarthDocument34 pagesNona D. Andaya-Castillo, IBCLC International Board Certified Lactation Consultant Director, Nurturers of The Earthjoan nicholsNo ratings yet
- Knowledge and Attitude On Initiation and Establishment of Breast Feeding Among Primi MothersDocument6 pagesKnowledge and Attitude On Initiation and Establishment of Breast Feeding Among Primi MothersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 16.I1.0106-LUCIA NADIANTY-DAPUS - ADocument6 pages16.I1.0106-LUCIA NADIANTY-DAPUS - AAyu MustikaNo ratings yet
- Nutrition in The Life Stages 1 Midterm NotesDocument21 pagesNutrition in The Life Stages 1 Midterm NotesJecel LazarraNo ratings yet
- IMC - Breast Feeding WeekDocument1 pageIMC - Breast Feeding WeekInterActionNo ratings yet
- Manual LunaDocument136 pagesManual LunaFacundo BarraganNo ratings yet
- English Case HIV in Pregnancy ArdeDocument48 pagesEnglish Case HIV in Pregnancy ArdeArde Hidayat100% (1)
- Failure To ThriveDocument93 pagesFailure To ThriveMuhammad Siddiq100% (2)
- Home Economics noteDocument11 pagesHome Economics notesolojam8288No ratings yet
- Lovely Baby Album-WPS OfficeDocument26 pagesLovely Baby Album-WPS OfficeBertlene LacsentoNo ratings yet
- PRINTDocument6 pagesPRINTRhea Kathleen MejiaNo ratings yet
- Aunchalee E.L. Palmquist, PHD, Ma, Ibclc, RLC: Curriculum VitaeDocument22 pagesAunchalee E.L. Palmquist, PHD, Ma, Ibclc, RLC: Curriculum Vitaemavecu0510No ratings yet
- Pediatrics Notes PDFDocument80 pagesPediatrics Notes PDFTG Meadow100% (2)
- Edited Final MekdiDocument61 pagesEdited Final MekdiBetelhiem WoldemedhinNo ratings yet
- The Effectiveness of Prone and Supine Nesting Position-DikonversiDocument11 pagesThe Effectiveness of Prone and Supine Nesting Position-DikonversiFirma WahyuNo ratings yet
- Exclusive BreastfeedingDocument19 pagesExclusive BreastfeedingVANGAWA JOHN100% (1)
- Case Digest Power of Taxation To Declaration of State PrinciplesDocument7 pagesCase Digest Power of Taxation To Declaration of State PrinciplesNorleviwilgemNo ratings yet
- CHN Rationalization 9 16Document22 pagesCHN Rationalization 9 16joyNo ratings yet
- Handbook For ASHA On Home Based Care For Young Child-EnglishDocument116 pagesHandbook For ASHA On Home Based Care For Young Child-EnglishDr. Vanitha BNo ratings yet
- PNC ComplicationsDocument125 pagesPNC ComplicationsZekariyas MulunehNo ratings yet
- Effectiveness of Breastfeeding Skills Training and Support Program Among First Time Mothers: A Randomized Control TrialDocument13 pagesEffectiveness of Breastfeeding Skills Training and Support Program Among First Time Mothers: A Randomized Control Trialnosh.rose95No ratings yet
- Week 15 MCHN Part 1Document7 pagesWeek 15 MCHN Part 1Cyrille Kibbz DonatoNo ratings yet
- Breastfeeding Without Birthing 3Document6 pagesBreastfeeding Without Birthing 3Mark Terence Padua AbrenicaNo ratings yet
- Weaning From The PumpDocument42 pagesWeaning From The PumpEvelyn Chua-FongNo ratings yet
- SRP Breastfeeding Awareness Group 2 NDDocument39 pagesSRP Breastfeeding Awareness Group 2 NDBern NerquitNo ratings yet
- History of Modern Design Third Edition David Raizman download pdfDocument40 pagesHistory of Modern Design Third Edition David Raizman download pdfsajidhirlam100% (2)
- Breast Feeding, Hiv Infection & NutritionDocument47 pagesBreast Feeding, Hiv Infection & NutritionlallianzualahauhnarNo ratings yet
- Nursing Research Paper - Final DraftDocument13 pagesNursing Research Paper - Final Draftapi-724442716No ratings yet
- Enterocolitis NecrosanteDocument21 pagesEnterocolitis NecrosantedenisNo ratings yet