☢️MED 2 634 OSPE OSCE CASES تجميعات
☢️MED 2 634 OSPE OSCE CASES تجميعات
Download as pdf or txt
You might also like
- Episode 29-Medicine Shelf Review 1Document54 pagesEpisode 29-Medicine Shelf Review 1Hersheyth AggarwalNo ratings yet
- OSPEDocument14 pagesOSPEHossain ShihabNo ratings yet
- Archer USMLE Step 3 Question BankDocument116 pagesArcher USMLE Step 3 Question Bankrolpf garri50% (4)
- Network Analysis and Synthesis - Franklin F. KuoDocument531 pagesNetwork Analysis and Synthesis - Franklin F. KuoMarco Vraja100% (1)
- PRES3 RecallsDocument9 pagesPRES3 RecallsAhmed GendiaNo ratings yet
- ACR EducationDocument53 pagesACR EducationamereNo ratings yet
- MRCP(UK) and MRCP(I) Part I Best of Fives: Volume IFrom EverandMRCP(UK) and MRCP(I) Part I Best of Fives: Volume INo ratings yet
- CASESDocument61 pagesCASES161220207No ratings yet
- Cardiovascular System Abbas HayatDocument35 pagesCardiovascular System Abbas HayatFiaz medicoNo ratings yet
- Patho Case ScenariosDocument15 pagesPatho Case ScenarioskarthikeyanNo ratings yet
- Internal Medicine Past Written OSCE Stations (2020 - 2023)Document11 pagesInternal Medicine Past Written OSCE Stations (2020 - 2023)Lesego Ladylee ManokoNo ratings yet
- Tutors Short Cases 1 8 With Answers 2018Document5 pagesTutors Short Cases 1 8 With Answers 2018RayNo ratings yet
- 1st MBBS Mock SEQ PaperDocument4 pages1st MBBS Mock SEQ PaperkevinonuransithNo ratings yet
- Nbme Medicine Shelf Review Session 2Document142 pagesNbme Medicine Shelf Review Session 2Swisskelly1100% (1)
- GEMP 3 2020 Advice & TestsDocument52 pagesGEMP 3 2020 Advice & TestsTresor KabambaNo ratings yet
- Hypomagnesemia and Prolonged Hospital Stay: A Case Report and Literature ReviewDocument6 pagesHypomagnesemia and Prolonged Hospital Stay: A Case Report and Literature ReviewIJAR JOURNALNo ratings yet
- Clinical Challenge SeriesDocument28 pagesClinical Challenge SeriesayugitaNo ratings yet
- Prelim LGDocument6 pagesPrelim LGNIRMIT BATAVIANo ratings yet
- Case Study of Anterior Wall MI 48Document32 pagesCase Study of Anterior Wall MI 48سوما الشمريNo ratings yet
- Medicine Multiple Choise QuestionsDocument61 pagesMedicine Multiple Choise QuestionsjuanmoraheNo ratings yet
- 1572790483Document43 pages1572790483Zain ApdiNo ratings yet
- He Ma To PathologyDocument30 pagesHe Ma To Pathologyapi-3722051No ratings yet
- Pathology ChartsDocument21 pagesPathology Chartspadma maliniNo ratings yet
- General Medicine Solved OspeDocument25 pagesGeneral Medicine Solved OspeSajjad AliNo ratings yet
- General Medicine Solved OspeDocument25 pagesGeneral Medicine Solved OspeAnass SaleemNo ratings yet
- Is It Always Anterior Chest Pain Angina Pectoris?Document7 pagesIs It Always Anterior Chest Pain Angina Pectoris?Diana MinzatNo ratings yet
- DR Shaf3y Neurology Revisions 6pDocument6 pagesDR Shaf3y Neurology Revisions 6pOmar HatemNo ratings yet
- PREVIOUS YEAR CASE SCENARIO Dr.PAVINDocument7 pagesPREVIOUS YEAR CASE SCENARIO Dr.PAVINtamilarasiramesh18No ratings yet
- Karapitiya OSCE 2017 With AnswersDocument34 pagesKarapitiya OSCE 2017 With Answersweerawarna fernandoNo ratings yet
- PracticeExam 2 AnsDocument51 pagesPracticeExam 2 AnsBehrouz YariNo ratings yet
- Choose Your Residency - Medicine and Allied by DR SiyabDocument136 pagesChoose Your Residency - Medicine and Allied by DR Siyabwkfxd6ckzwNo ratings yet
- Medicine A Supply 2022: Course of Oral Steroids. On Examination There Is Point Tenderness On Upper Lumber SpineDocument8 pagesMedicine A Supply 2022: Course of Oral Steroids. On Examination There Is Point Tenderness On Upper Lumber SpineRabia RabiaNo ratings yet
- Final Medical Examination 4 Year Medical Student:) Select ONE BEST Answer (Document10 pagesFinal Medical Examination 4 Year Medical Student:) Select ONE BEST Answer (Dhanoush MşđNo ratings yet
- 1 Copy 15Document67 pages1 Copy 15imlegoldstandardNo ratings yet
- CDSA CirculatoryDocument41 pagesCDSA Circulatoryapi-3728522No ratings yet
- Dereje TadesseDocument6 pagesDereje TadesseDereje TadesseNo ratings yet
- Disseminated Intravascular Coagulation and MalignaDocument6 pagesDisseminated Intravascular Coagulation and MalignakhineihmuNo ratings yet
- File 95 - Recall-Questions-File-2Document6 pagesFile 95 - Recall-Questions-File-2Abdullah Althabet50% (2)
- PDFDocument59 pagesPDFfatma daganeNo ratings yet
- CoC ExamDocument29 pagesCoC Examanteneh67% (3)
- Conrad Fischer MCQsDocument328 pagesConrad Fischer MCQsPopescu Tina100% (1)
- General Pathology 2nd BM Neoplasia Blood Vessel Cardiovascular Pathology Pulmonary PathologyDocument64 pagesGeneral Pathology 2nd BM Neoplasia Blood Vessel Cardiovascular Pathology Pulmonary PathologyCherry RahimaNo ratings yet
- 7th Mbbs Yr5 Sem10 Medicine MCQ Baq SaqDocument7 pages7th Mbbs Yr5 Sem10 Medicine MCQ Baq SaqAshbirZammeriNo ratings yet
- Patho4 CDSA CirculatoryDocument30 pagesPatho4 CDSA Circulatoryapi-3728522No ratings yet
- Cardiac Function TestsDocument3 pagesCardiac Function TestsKanishk ChawlaNo ratings yet
- Practice Exam 1Document103 pagesPractice Exam 1aayceeNo ratings yet
- 2.2 Theory Paper II (Problem and Data)Document4 pages2.2 Theory Paper II (Problem and Data)hanlintunNo ratings yet
- Aiimsmedicnequiz2021 Prelims 210912131541Document67 pagesAiimsmedicnequiz2021 Prelims 210912131541Tarakeesh CHNo ratings yet
- USMLE Step 3 Answers To ARCHER Q Bank 1-25Document15 pagesUSMLE Step 3 Answers To ARCHER Q Bank 1-25rashmiajNo ratings yet
- SMLE SESSION 4Document55 pagesSMLE SESSION 4yazid9saadNo ratings yet
- Case 1 History:: RBC Tutorial and AssignmentDocument7 pagesCase 1 History:: RBC Tutorial and AssignmentAbdirashidNo ratings yet
- 9 RFTCXDocument24 pages9 RFTCXpotnic44No ratings yet
- Qstream-1 2Document55 pagesQstream-1 2Vijay100% (1)
- 2 Diclihon Ischemic StrokeDocument5 pages2 Diclihon Ischemic StrokeAllan CastroNo ratings yet
- Self-Assessment: BOFs for MRCP(UK) and MRCP(I) Part IFrom EverandSelf-Assessment: BOFs for MRCP(UK) and MRCP(I) Part INo ratings yet
- Multiple Sclerosis and CNS Inflammatory DisordersFrom EverandMultiple Sclerosis and CNS Inflammatory DisordersLawrence M. SamkoffNo ratings yet
- Practical Management of Systemic Sclerosis in Clinical PracticeFrom EverandPractical Management of Systemic Sclerosis in Clinical PracticeNo ratings yet
- Annual Update in Intensive Care and Emergency Medicine 2020From EverandAnnual Update in Intensive Care and Emergency Medicine 2020No ratings yet
- 6 Months RAN ActivityDocument14 pages6 Months RAN ActivityDaveNo ratings yet
- TalatiDocument143 pagesTalatisunilarunaNo ratings yet
- IBFcoursemoduleDocument1 pageIBFcoursemodulegutluNo ratings yet
- Django Oauth Toolkit LatestDocument56 pagesDjango Oauth Toolkit Latestmarian_costache_2No ratings yet
- Kademe Mini TipperDocument3 pagesKademe Mini TipperAkif ErgunNo ratings yet
- Case Study of BrazilDocument4 pagesCase Study of Brazilcheetah128No ratings yet
- KAFO Vertical-Machining-Center 2019.02Document18 pagesKAFO Vertical-Machining-Center 2019.02randolf cabezaNo ratings yet
- 1.13 Recycle, Bypass, and PurgeDocument13 pages1.13 Recycle, Bypass, and PurgeJosch DenilaNo ratings yet
- Oxygen (Oxygenium) : The International Pharmacopoeia - Tenth Edition, 2020Document5 pagesOxygen (Oxygenium) : The International Pharmacopoeia - Tenth Edition, 2020Passmore DubeNo ratings yet
- Savage 2017Document47 pagesSavage 2017the_fralics9349No ratings yet
- Tenaga Sub Profesional Ekonomi Regional - WijiantoDocument15 pagesTenaga Sub Profesional Ekonomi Regional - WijiantowijiantotepasNo ratings yet
- BW Controller ManualDocument139 pagesBW Controller ManualKarito RojasNo ratings yet
- SyllabusDocument3 pagesSyllabushassaneldibNo ratings yet
- Blake Wordsworth Coleridge HandoutDocument6 pagesBlake Wordsworth Coleridge HandoutFilip Polak100% (1)
- 03 The Radioactive Material.Document2 pages03 The Radioactive Material.khurramNo ratings yet
- Bonus15 Como Negociar SubPersonalidades Time de Sucesso SubconscienteDocument13 pagesBonus15 Como Negociar SubPersonalidades Time de Sucesso SubconscienteOpvlentvsNo ratings yet
- Hydrolysis of StarchDocument5 pagesHydrolysis of StarchJayrone James FuerteNo ratings yet
- CV English October FinalDocument48 pagesCV English October FinalumegeeNo ratings yet
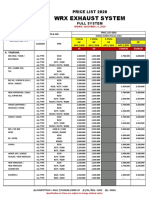
- WRX Exhaust System: Price List 2020Document3 pagesWRX Exhaust System: Price List 2020Safaat PradanaNo ratings yet
- Infrared Thermography Report: ExampleDocument7 pagesInfrared Thermography Report: ExamplesifuszNo ratings yet
- Arne Naess, The Basics of Deep EcologyDocument11 pagesArne Naess, The Basics of Deep EcologytathagathanNo ratings yet
- E2E Delay: R R R LDocument4 pagesE2E Delay: R R R Lspade0987No ratings yet
- Epson L365Document2 pagesEpson L365Jimmy G. Díaz VegaNo ratings yet
- Free Rider & Rocker Instruction ManualDocument1 pageFree Rider & Rocker Instruction ManualBen SzapiroNo ratings yet
- Shunt Capacitor Bank Fundamentals and ProtectionDocument2 pagesShunt Capacitor Bank Fundamentals and ProtectionaryanNo ratings yet
- lecture_8Document29 pageslecture_8Imen KsouriNo ratings yet
- 4 Scob HCD 8Document6 pages4 Scob HCD 8janago7405No ratings yet
- Capacitor in DC Circuits 2Document4 pagesCapacitor in DC Circuits 2JagatNo ratings yet
- Toward Complexity-Effective Verification: A Case Study of The Cray SV2 Cache Coherence ProtocolDocument9 pagesToward Complexity-Effective Verification: A Case Study of The Cray SV2 Cache Coherence ProtocolmightNo ratings yet