
Informed Consent
Informed Consent
Uploaded by
Wayan ArdhanaCopyright:
Available Formats
Informed Consent
Informed Consent
Uploaded by
Wayan ArdhanaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Informed Consent
Informed Consent
Uploaded by
Wayan ArdhanaCopyright:
Available Formats
70 Orthodontic Update
September 2008
Oliver J Campbell
Daljit S Gill and Farhad B Naini
Informed Consent and Orthodontic Treatment
Abstract: Informed consent is a fundamental component of good clinical practice and clinical governance. Dental practitioners must be aware of the principal factors that need to be addressed to ensure that consent is valid. This paper provides a comprehensive review of current English law on consent issues and relates these to proposed orthodontic treatment. Clinical Relevance: Orthodontic treatment is not without risk to the patient. The clinician undertaking treatment must aim to provide the competent patient with enough information to perform a risk-benefit analysis, supported by best current scientific evidence, so that an informed decision can be made prior to commencing orthodontic treatment. Ortho Update 2008; 1: 70-76 The Nuremberg Code (1947)1 is generally regarded as the first document to establish ethical regulations in human experimentation based on informed consent. Later, the Declaration of Helsinki (1964),2 developed by the World Medical Association, made informed consent a central requirement for ethical research. In English law, there is no overall statute which sets out the general principles of consent. However, case law (common law) has established that touching a patient without valid consent may constitute the civil or criminal offence of battery. Therefore, consent prior to active treatment is a general legal and ethical principle that is fundamentally central to all forms of healthcare. With the advent of Modernising NHS Dentistry (2000)3 and issues of clinical governance, valid consent prior to treatment is absolutely central to ensure the provision of a high standard of clinical dental care4 and is advocated by the defence societies of the United Kingdom and the NHS Management Executive. A comprehensive summary of current English legal requirements for obtaining valid consent and on the situations where the law recognizes exceptions to common law has been published by the Department of Health in England (DH).5 This document also includes references to legal cases and good practice guidance from regulatory bodies such as the General Medical Council. Along with this article, a recent circular (HSC 2001/023),6 aimed at clinicians, focused on the action necessary and required time-scales for implementing the model consent documentation in day-today NHS practice. A number of DH guidance documents and leaflets on consent for patients7,8 are also available from the DH website (www.dh.gov.uk). As highlighted in The NHS Plan (2000),9 a DH advisory group produced national consent guidance to ensure that best practice, when patients consent to examination or treatment, was adopted throughout the NHS. The guidance included a model consent policy and four model consent forms to be used locally as part of their good practice in consent initiative.10 By following consent principles, the clinician may be protected, under the law of tort, from liability from patient complaints (through the NHS complaints procedure or to professional bodies), civil claims and claims of negligence but NOT criminal charges. However, the NHS Litigation Authority has recently issued an alert regarding changes to the law on informed consent. As highlighted by the recent case of Chester v Ashfar (2004),11 the House of Lords decision had the effect of significantly extending clinicians liability in cases where less than full consent is obtained. Despite the acknowledgment that there had been no clinical negligence, the adverse outcome, combined with the invalid consent (as the patient claimed lack of information), led to the successful judgement of negligence. It must be appreciated that case law on consent is a constantly evolving area and health professionals have a duty to remain up-to-date with regard to legal developments which may affect their practice.
What is consent?
Consent is defined as: The voluntary and continuing permission of the patient to receive particular treatments. It must be based upon adequate knowledge of the purpose, nature, likely effects and risks of that treatment, including the likelihood of its success, and a discussion of any alternative to it.12 Normally, it is the patient undergoing orthodontic treatment that gives consent, although there are occasions whereby the consent of a parent/guardian is required (discussed later). There are two main
Oliver J Campbell, BDS, MSc, MFDS RCS (Eng), MOrth RCS(Eng), Specialist Registrar in Orthodontics, Department of Orthodontics, UCL Eastman Dental Institute and Hospital, UCLH Foundation Trust, London, Daljit S Gill, BSc(Hons), BDS(Hons), MSc, FDS RCS(Eng), MOrth RCS(Eng), FDS(Orth) RCS, Consultant in Orthodontics/Honorary Senior Lecturer, Department of Orthodontics, UCL Eastman Dental Institute and Hospital, UCLH Foundation Trust, London and Honorary Consultant, Great Ormond Street Hospital, London, Farhad B Naini, BDS, FDS RCS, MSc, MOrth RCS, FDSOrth RCS, Consultant Orthodontist, St Georges Hospital and Kingston Hospital, London, UK.
September 2008
Orthodontic Update 71
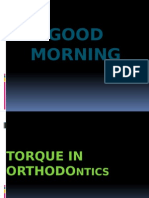
TISSUE EXTRA-ORAL Soft
RISK Trauma Skin allergy Burns
COMMENTS UK - 3.6% extra- and intra-oral injuries with Klen type facebow;37 eye injury - rare HG strap or whisker/bonding agents (rare)/latex Uncommon. Chemical acid burn from etchant/thermal Common in population. Multifactorial aetiology. Good evidence orthodontics does not cause or cure TMD38 Evidence very little. Extractions may have a small effect on profile (not necessarily detrimental). No significant difference in facial profile of extraction v non-extraction cases. Facial growth - overriding factor39 Common. 296% incidence40 Risk of abrasion Ceramic brackets > metal brackets Transient. Nearly all FA wearers. Attachment loss rare Uncommon. Minimal crestal loss (0.51 mm) and no longterm effect41 (if no pre-existing periodontal disease) Transient pulpitis (90%). Loss of vitality increased risk in previously traumatized teeth42 Some degree of external root resorption inevitable Risk factors: Blunt and pipette-shaped roots/short roots (16.5% of teeth loss of root length exceeding 2.5 mm).45 Previous tooth trauma (periapical radiograph monitoring preand during treatment is essential). Treatment mechanics heavy forces/FA/rectangular AW/Class 2 traction/ treatment time/distance of tooth movement/tooth intrusion and torque. Long term effects rare Common. Ulceration from AW/brackets/HG whisker Rare. Nickel46 (most common allergen) AW/bands/ brackets/HG. Latex elastics/gloves. Bis-GMA bonding agents Highly subjective. After FA adjustment: intensity dependent on age and diurnal variation. Duration: 56 days;47 initial pain perceived at 2 hours, peak at 24 hours and reduction by day 348 Risk of damage to the restoration (eg veneer/crown)/Heavily restored teeth at debond Particularly upper canines undergoing orthodontic alignment. Risks: discoloration, ankylosis, root resorption, relapse Rare. Sources as above Risk procedures: Extractions/banding/separation/cleaning and polishing/?traction to unerupted teeth Consider: Bacterial/viral/fungal/prion and new variant CJD radiation exposure DPT/lateral cephalogram/intra-oral films
TMJ Profile
Temporomandibular dysfunction (TMD) Profile damage
INTRA-ORAL
Enamel
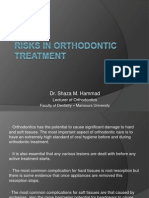
Decalcification/ caries (Figure 1) Fracture/wear Gingival inflammation (Figure 2) Alveolar bone loss Pulpal reactions Root resorption43,44 (Figure 3)
Periodontal
Pulp Root
Other Allergy
Soft tissue trauma (Figure 4)
Pain
Restorations (Figure 5) Ectopic canines49,50 (Figure 6) SYSTEMIC Allergy Infective endocarditis51 Cross infection Radiation
Table 1. Summary of the potential extra-/intra-oral and systemic iatrogenic risks associated with orthodontic treatment. (Abbreviations HG: headgear; FA: fixed appliance; AW: archwire).
72 Orthodontic Update
September 2008
Figure 1. Extensive decalcification of the dentition following orthodontic treatment.
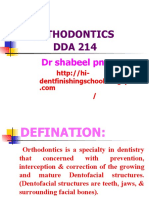
Figure 4. Trauma to the buccal mucosa during fixed appliance orthodontic treatment.
Figure 2. Severe inflammation of the gingival tissues immediately following orthodontic treatment.
Figure 5. Decoronation of the first permanent molar on removal of the rapid maxillary expansion (RME) device.
caveat that must be remembered is that a consent form is only a record and not proof that genuine consent has been obtained. Hence, the conclusion that a signed consent form is synonymous with valid consent is misleading. For consent to be valid, the person (child or adult) must: Be capable of making that particular decision (competent); Act voluntarily and freely (without duress or pressure) from emotional situations and not taking drugs or medicines that could influence understanding;13 Be provided with enough information to enable them to make a decision. It is paramount that the patient undergoing the proposed treatment fully understands the factors involved. The orthodontic provider has the responsibility of providing the information (properly recording this in the notes) and explaining it carefully and comprehensively in terminology that the patient understands. This particularly applies to children and, in addition, should take into account that English may not be the patients first language, whereby an interpreter should be involved. Time should also be given to allow the patient to digest the disclosed information.
What information should be disclosed?
There are key principal factors that need to be discussed jointly between patient and orthodontic provider when seeking valid consent prior to treatment. The information to be provided presents a relatively exhaustive list of potential topics for discussion and essentially represents a risk-benefit management strategy.14 For orthodontics, these factors include: The nature and purpose of all viable treatment options (including the implications of non-treatment); What each proposed treatment will and will not achieve (particularly if treatment objectives are limited) and the likelihood of success; The proposed benefits, limitations and risks of treatment; The degree of patient commitment required. Important practical information that patients/parents need include an estimation of treatment time, the frequency of appointments, the need for additional appointments if breakages occur and the need for retention; The cost of the treatment (if applicable). As a result of the ruling in the Chester v Afshar case (2004), the NHS Litigation Authority (2004) announced the following recommendations:
Figure 6. Ankylosis of the upper right canine during orthodontic alignment with fixed appliances and consequent severe disruption of the occlusal plane.
Figure 3. Marked root resorption of the upper central incisor teeth during fixed appliance orthodontic treatment: (a) pre-treatment; (b) during treatment.
types of consent: Implied (eg voluntarily opening the mouth to allow examination); or Expressed (oral or written to an examination or specific procedure). At present, there is no requirement in common law for written
consent and it makes no difference whether a form is signed by a patient to indicate his/her consent or whether it is given orally or nonverbally. Also, English law does not directly prescribe a threshold above which a formal conversation between the treatment provider and patient concerning consent should occur. However, as a general rule, the more complex the treatment becomes, the greater the need to ensure that the patient has given his/ her consent. The value of a signed consent form is that it provides some evidence of an agreement between the patient and the clinician and, for the sole purpose of defending against negligence claims, signed consent should be mandatory. An important
September 2008
Orthodontic Update 73
Extreme care in the taking of consent is even more crucial than ever; Careful and comprehensive warnings about all significant possible adverse outcomes must be given; These warnings must be properly recorded in the notes; Patients should be invited to sign the relevant entry to confirm that he/she has been given the warning, has understood it, and accepts the risk; It is equally important to make a full entry in the notes, preferably signed by the patient, if treatment is refused, including the reason when given; Whenever possible, the clinician who discussed and is able to perform the treatment should be the one who obtains the consent.
Does the patient have the capacity to consent?
The current DH booklet Seeking Consent: Working with Children (2001)15 provides comprehensive guidance to healthcare practitioners on how to seek consent from children in their care. Generally, if children are competent to give consent for themselves, it should be taken directly from them before examination and treatment. However, the legal position regarding competence is more complex in English law for children aged above and below 16 years of age. As the current law stands, the basic principles are as follows.
Children aged 16 and 17 years
Gillick competent (coined by Lord Scarman in 1985).17 However, it must be remembered that a childs capacity can only be determined in the context of the proposed treatment. Consequently, the understanding of minors may vary, depending on different treatment procedures and, therefore, the issue of the consent being valid may arise. In England and Wales, the Fraser ruling does not apply to unreasonable refusal by a child to receive treatment which is in the childs best interest. Legally, a person with parental responsibility or a court can, in certain circumstances, over-ride the decision of a competent child (under 16) if he or she refuses treatment. Under the Children Act (1989),18 this action is considered if it is in the childs best interests but is an unlikely event in orthodontic treatment. In Scotland, however, children may refuse treatment provided they are competent. Ultimately, for an ideal orthodontic outcome, parental support and involvement in the decision-making process are key factors for the success of treatment and valid consent should be sought from the patient and assent from the parent.
Treating non-competent patients
According to Section 8(1) of the Family Law Reform Act (1969),16 young people (aged 16 years and over) are presumed in law to be competent to consent for themselves for medical, surgical or dental treatment. Therefore, this means that in many respects they should be treated as adults and it is not necessary to obtain a separate consent from the parent or guardian. If a competent child consents to orthodontic treatment and the requirements of valid consent are met, a parent cannot over-ride that consent except in exceptional circumstances (although this is unlikely to occur in orthodontics).
Younger children (under 16 years)
For the management of minors, clinicians should seek the agreement of the parent or carer. However, patients below 16 years of age who have sufficient competency and maturity to understand the consequences of their orthodontic treatment may also, in principle, give consent independent of parental or legal guardian responsibility. This is now referred to as Fraser ruling competent as opposed to
One issue that poses a problem for clinicians assessing competence are those patients in which competence is doubtful, hence their ability to provide valid consent is questionable. In England and Wales (not Scotland), no adult, including next-of-kin, can give consent for treatment on behalf of another adult (aged 18 or over). As it stands, current English law allows a patient who lacks the capacity to consent to be treated without consent if the proposed treatment is necessary and in the patients best interest. The Mental Capacity Act (2005),19 which came into force in April 2007 in England and Wales, provides a statutory framework to empower and protect vulnerable people who are unable to make their own decisions. It sets out clear legal requirements for both assessing patient competence (referred to capacity in the act) and the treatment of non-competent patients. Generally, the act applies to people aged 18 and over but may also apply to 16 and 17 year-olds whose incompetence is likely to persist into adulthood. The Act is governed by the following five key principles: A presumption of capacity every adult has the right to make his or her own decisions and must be assumed to have the capacity to do so unless it is proved otherwise; The right for individuals to be supported to make their own decisions people must be given all appropriate help before anyone concludes that they cannot make their own decisions;
That individuals must retain the right to make what might be seen as eccentric or unwise decisions; Best interests anything done for, or on behalf of, people without the capacity must be in their best interests; Least restrictive intervention anything done for, or on behalf of, people without the capacity should be the least restrictive of their basic rights and freedoms. If a child is not competent to give consent directly, it should be sought from a person (legally, only one is required) with parental responsibility and normally this means the childs parent(s). However, the Children Act (1989) has identified a number of people who may have legally acquired parental responsibility.18 Principally, it discusses the issues related to whether the parents are legally married or not, the role of a legally appointed guardian and the role of a local authority if designated. For example, a natural father not married to the childs mother at the time of the childs birth has no parental responsibility unless it has been acquired under the terms of the Children Act (1989).18 Under the Act, generally in an emergency situation, the clinician should proceed with treatment if it is in the patients best interest. More complex issues regarding children and consent are provided by the DH publication on Seeking Consent: Working with Children (2001).15
Orthodontic management
As highlighted, effective communication is a key process in healthcare provision. So that valid consent may be obtained, it is paramount that patients are fully versed of the various aspects of orthodontic management that raise consent issues (eg the benefit versus the risk of treatment). In most orthodontic cases where written consent is being sought, treatment options will generally be discussed well in advance of the actual procedure being performed. The consent process will therefore have at least two stages. After the initial consultation, patient leaflets are an invaluable source of information to reference for patients considering treatment. However, a recent study has highlighted the inadequacies of a number of current orthodontic patient information leaflets (PILs) from professional organizations and commercial companies. Specifically, the mean readability of all the PILs was deemed fairly difficult to understand for 60% of the UK population.20 Also, information recall (15 to 30 minutes later) from both patient and parent after explanation from the orthodontic provider regarding the proposed orthodontic treatment (eg the reasons for
74 Orthodontic Update
September 2008
treatment, the risks, etc) is low21 (particularly in less educated, low-income patients). Therefore, some patients may not fully comprehend the information given during informed consent discussions. Consequently, this may have important implications when assessing whether the informed consent is actually valid. The Developments and Standards Committee of the British Orthodontics Society (BOS) has produced a number of clinical guidelines, which have been critically reviewed from a medico-legal perspective,22 and three consent documents.23 For orthodontic management, the relevant BOS advice sheets include: Consent in Orthodontics (including multidisciplinary management);24 The use and storage of digital photographs;25 The use of headgear and facebows.26 However, despite the importance of obtaining valid consent, a recent survey of all consultant orthodontists on the BOS database showed that written information on orthodontic treatment was provided by only 56% of respondents and that written consent was only obtained by 41%.27
Orthodontic treatment
Orthodontics encompasses a spectrum of treatment modalities to correct malocclusions which may be a result of tooth irregularity, disproportionate
jaw relationships, or both. It is considered good clinical practice for the orthodontic provider to obtain written consent before any proposed orthodontic treatment. This includes: The extraction of teeth (primary and secondary) as part of the treatment plan; The provision of removable (including retention appliances), functional and fixed appliances; The provision of headgear; Multidisciplinary treatment. Appliance therapy may or may not be indicated, depending on a number of patient (eg compliance) and clinical factors, as assessed by the dental health and aesthetic components of the Index of Orthodontic Treatment Need (IOTN).28 Ultimately, treatment should be based on a comprehensive risk-benefit analysis and the clinician should seek to minimize risk and employ risk management strategies.29 As some patients are more at risk than others, when orthodontic treatment is to be undertaken, it is paramount that the competent patient is fully versed in the reasons for treatment and the risks so that a fully informed decision can be made and valid consent obtained. Importantly, it must be remembered that consent is dynamic and can be withdrawn at any time, even in the middle of orthodontic treatment. If a patient wishes to terminate treatment early, advice
should be given to the patient on the likely adverse consequences. Subsequently, the fixed appliances must be removed if the patient still wishes to terminate treatment prematurely and the incident recorded in the patient's notes.
Multidisciplinary treatment
Patients who require both orthodontic treatment and a procedure from another dental specialty (eg major surgery and/or complex restorative procedures) need particular care. Good inter-specialty communication and the appropriate liaison between clinicians (eg joint specialist clinics) is essential. Sufficient clarity and detail must be provided from each of the specialties on who is to provide what treatment. This ensures that the patient can decide and provide valid consent for both procedures before either treatment is started. For restorative procedures, particular emphasis should be placed on the long-term implications. In all multidisciplinary cases, it is good clinical practice to obtain written consent.
Digital photography
The use and storage of digital images is an essential component of orthodontic patient records. However, at present, there is an absence of clear DH guidelines owing to the local nature of the advice between various employing
BENEFIT Appearance Function Dento-facial aesthetics Mastication Speech Dental health TMD38 Tooth impaction Caries
COMMENTS Evidence improved psychological health59 Evidence equivocal Evidence none that orthodontic treatment will correct disorders Evidence weak linking predisposition to TMD ? risk of dentigerous cyst formation associated with unerupted canines Multifactorial aetiology. Evidence none that orthodontic treatment reduces caries risk Evidence none that orthodontic treatment reduces risk of long-term periodontal disease Evidence some migration of incisors where OJ has been Reducing an OJ: ? reduces risk of future tooth trauma60 OB: labial and palatal trauma 2 to deep OB but no long-term problems if oral hygiene is good Teasing about teeth caused greatest distress Evidence none that malocclusion causes poor self esteem in long-term
Periodontal disease58
Trauma
Psychological
Well-being/self-esteem14
Table 2. Summary of the proposed benefits of orthodontic treatment. (Abbreviations OJ: overjet; OB: overbite).
September 2008
Orthodontic Update 75
organizations, ie particularly NHS Trusts. Nevertheless, it is important to consider obtaining consent and to comply with the rules of the Data Protection Act (1998),30 which came into force in March 2000. The following points are adapted from BOS Advice Sheet 525 and summarize the general advice:
Do I need consent for photography?
consent should be obtained and that this be recorded in the patient records under the relevant heading in the locally issued consent form.
RISKS of orthodontic treatment
strategies have been broadly reviewed35, 36 and include: Tissue damage; Treatment failure and relapse; Greater predisposition to dental disorders.
Tissue damage
DH model consent policy: states that if there is no prospect of a patient being recognised from a clinical photograph, then it may be used within the clinical setting for education or research purposes without the express consent of the patient. However, where it is possible to identify the patient, specific written consent must be obtained. The Institute of Medical Illustrators (IMI) model consent policy (http://www.imi. org.uk): states that subjective interpretation of whether a patient is likely to be identified from a clinical photograph is not sufficient and written consent must be obtained. If there is any doubt, obtaining written consent is advisable.
What about dental practice and the Data Protection Act?
A dental practice should be registered with the Information Commissioners Office (ICO), even if not computerized, because it holds personal information that can be directly traced to the patient. With the advent of digital image use and storage, a dental practice may need to seek advice from and notify the ICO. The ICO (www.dataprotection.gov.uk/) is an independent public body set up to promote access to official information and to protect personal information. It aims to regulate and enforce the Data Protection Act and provides guidance to organizations and individuals.
What about hospital and community departments?
Regarding the possible risks of orthodontic treatment and what information should be disclosed to the patient so that the clinician may avoid a claim of negligence, English law is continually evolving, as highlighted by the number of milestone cases. Currently, English law utilizes the Bolam (1957)31 test in cases of alleged dental negligence. Essentially, the judgement ruled that a clinician is not negligent if he/ she informs the patient of the same risks as a responsible body of medical opinion, this representing the professional standard. Furthermore, as illustrated by the Sidaway case (1985)32, the House of Lords extended the Bolam test and described which risks should be explained to inform the patient. The House was increasingly determined to make clinicians more accountable for their actions and, if the clinician was too lax in informing the patient, then the courts may intervene. The prevailing view was that the standard of information provision should be judged according to the Bolam criteria. Since Sidaway, it is evident that English law is moving towards making consent more patient-centred where the main issue is what a reasonable patient (an objective standard) would expect to be informed about as the standard. This was highlighted by the case of Pearce v United Bristol Healthcare NHS Trust (1998)33 whereby Lord Woolf concluded that: if there is a significant risk which would affect the judgement of a reasonable patient, then in the normal course it is the responsibility of a doctor to inform the patient of that significant risk; if the information is needed so that the patient can determine..what course he or she should adopt. The Australian adoption of the objective reasonable patient was undertaken following the case of Rogers v Whittaker (1993),34 which judged that, even a remote risk should be disclosed if it had potentially serious consequences, regardless of the view of a responsible body of medical opinion. Therefore, for valid consent, ideally all risks, however low, should be highlighted to the patient and parent prior to the start of orthodontic treatment so that a mutual decision can be made as to whether treatment should commence. The potential hazards of orthodontic treatment and prevention
(Table 1)
Treatment failure and relapse
It has been estimated that failure to complete orthodontic treatment is high (423%)52 and may be attributed to patient non-compliance, incorrect diagnosis or incorrect management (eg incorrect choice of appliance).35 Post-orthodontic treatment relapse53 may result secondarily to: Soft tissue factors (eg teeth initially severely rotated); Late facial growth and occlusal development (eg leading to lower labial segment crowding); Supporting tissue factors (eg compromised periodontal support); Occlusal factors (eg insufficient overbite to maintain a corrected Class III incisor relationship); Non-compliance with recommended retention regime; Persistence of habits. There are currently no predictive factors54 that enable clinicians to identify patients that are likely to relapse or suffer late lower incisor crowding. Therefore, to guarantee long-term tooth alignment after orthodontic treatment, it is important to explain to patients about the requirement to wear retaining appliances on a long-term basis before commencing treatment.
Greater predisposition to dental disorders
Local rules apply and it is important to seek advice from the Trusts data protection officer who ensures the Data Protection Act is complied with. In some Trusts, employees (including trainees) are considered independent data controllers and must register with the Data Protection Act. In others, individuals may already be covered by the Trust/University data registration provided they comply with the local rules of the Trust. If in doubt, seek advice from the local Trusts data protection officer. Compliance with the Data Protection Act is fundamental as part of the consent process. It is prudent to ensure that patients are aware of the use of their images, particularly if they are to be used in patient information leaflets, for publication or on the World Wide Web. It is important that valid
Supposedly, orthodontic treatment may increase the predisposition to a number of certain problems, including temporomandibular joint dysfunction syndrome (TMJDS) and periodontal disease. At present, a large contingent of studies55,56,57 have concluded that the evidence directly linking orthodontic treatment to TMJDS is equivocal at best. There is also no evidence to suggest that patients undergoing orthodontic treatment are at a greater risk of long-term periodontal disease.58
Benefits of orthodontic treatment
As well as being fully informed of the potential iatrogenic risks of orthodontic therapy, the patient should be advised of the proposed benefits to dento-facial aesthetics and dental health from orthodontic treatment (Table 2).
Conclusion
Ultimately, orthodontic treatment
76 Orthodontic Update
September 2008
aims to provide the patient with optimum dento-facial aesthetics and a functional, stable occlusion. If these principal factors are to be achieved, shared responsibility between the orthodontic provider and the patient must be sought and valid consent obtained prior to active treatment. Consent issues can be complex (particularly with respect to the treatment of children) and are constantly changing. It is imperative that clinicians maintain an up-to-date knowledge of the legal aspects of consent so that optimum clinical care can be delivered.
References
1. 2. 3. Nuremberg Doctors Trial. The Nuremberg Code (1947). Br Med J 1996; 313: 1448. Nuremberg Doctors Trial. Declaration of Helsinki (1964). Br Med J 1996; 313: 14481449. Department of Health. Modernising NHS Dentistry Implementing the NHS Plan, September 2000; 151. General Dental Council Standards Guidance. Principles of Patient Consent. May 2005; 18. Department of Health. Reference Guide to Consent for Examination or Treatment. April 2001; 130. Department of Health. HSC 2001/023: Good Practice in Consent: Achieving the NHS Plan Commitment to Patient-centred Consent Practice. November 2001; 15. Department of Health. Consent: A Guide for Children and Young People. July 2001; 112. Department of Health. Consent What You have the Right to Expect: A Guide for Adults. July 2001; 112. Department of Health. The NHS Plan: A Plan for Investment, A Plan for Reform. July 2000; 1144. Department of Health. Good Practice in Consent Implementation Guide: Consent to Examination or Treatment. November 2001; 155. Chester v Ashfar (2004) UKHL 41. Department of Health. (http://www.dh.gov. uk/en/index.htm) Poswillo D. Obtaining consent to oral and maxillofacial surgery. Ann Acad Med Singapore 1989; 18: 616621. Shaw WC, OBrien KD, Richmond S, Brook P. Quality control in orthodontics: risk/benefit considerations. Br Dent J 1991; 170: 3337. Department of Health. Seeking Consent: Working with Children. November 2001; 127. Family Law Reform Act 1969. Gillick v West Norfolk and Wisbech Health Authority (1985) 3 All ER 402-437. Children Act 1989 (http://www.opsi.gov.uk/ acts/acts1989/Ukpga_19890041_en_1.htm). Mental Capacity Act 2005. (http://www.opsi. gov.uk/acts/acts2005/20050009.htm). Harwood A, Harrison JE. How readable are orthodontic patient leaflets? J Orthod 2004; 31: 210219. Mortensen MG, Kiyak HA, Omnell L. Patient and parent understanding of informed consent in orthodontics. Am J Orthod Dentofacial Orthop 2003; 124: 541550.
4. 5.
6.
7. 8.
9. 10.
11. 12. 13.
14.
15. 16. 17. 18. 19. 20.
21.
22. Jones JW. A medico-legal review of some current UK guidelines in orthodontics: a personal view. Br J Orthod 1999; 26: 307324. 23. Haines WF, Williams DW. Consent and Orthodontic Treatment. Br J Orthod 1995; 22: 101103. 24. Developments and Standards Committee. Advice Sheet 4: Consent in Orthodontics. BOS 2003. 25. Developments and Standards Committee. Advice Sheet 5: The Use and Storage of Digital Photographs. BOS 2004. 26. Developments and Standards Committee. Advice Sheet 8: The Use of Headgear and Facebows. BOS 2001. 27. Gardner AW, Jones JW. An audit of the current consent practices of consultant orthodontists in the UK. J Orthod 2002; 29: 330334. 28. Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod 1989; 11: 309320. 29. Nightingale C. Belle Maudsley Lecture 2001. Risk management in orthodontics making clinical practice safer. Dent Update 2001; 28: 437441. 30. Data Protection Act 1998. (http://www.opsi. gov.uk/acts/acts1998/19980029.htm). 31. Bolam v Friern Barnet Hospital Management Committee (1957) 1 WLR 582. 32. Sidaway v Board of Governors of the Bethlem Royal and the Maudsley Hospital (1985) 1 All ER 643. 33. Pearce v United Bristol Healthcare NHS Trust (1998) 48 BMLR 118. 34. Rogers v Whittaker (1993) 67 ALJR 47. 35. Ellis PE, Benson PE. Potential hazards of orthodontic treatment what your patient should know. Dent Update 2002; 29: 492496. 36. Travess H, Roberts-Harry D, Sandy J. Orthodontics. Part 6: Risks in orthodontic treatment. Br Dent J 2004; 196: 7177. 37. Samuels RH, Willner F, Knox J, Jones ML. A national survey of orthodontic facebow injuries in the UK and Eire. Br J Orthod; 23: 1120. 38. Luther F. Orthodontics and the temporomandibular joint: where are we now? Part 1. Orthodontic treatment and temporomandibular disorders. Angle Orthod 1998; 68: 295304. 39. Paquette DE, Beattie JR, Johnston LE. A long-term comparison of nonextraction and premolar extraction edgewise therapy in borderline Class II patients. Am J Orthod Dentofacial Orthop 1992; 102: 114. 40. Chang HS, Walsh LJ, Freer TJ. Enamel demineralization during orthodontic treatment. Aetiology and prevention. Aus Dent J 1997; 42: 322327. 41. Alstad S, Zachrisson BU. Longitudinal study of periodontal condition associated with orthodontic treatment in adolescents. Am J Orthod 1979; 76: 277286. 42. Hamilton RS, Gutmann JL. Endodonticorthodontic relationships: a review of integrated treatment planning challenges. Int Endod J 1999; 32: 343360. 43. Brezniak N, Wasserstein A. Orthodontically induced inflammatory root resorption. Part I: The basic science aspects. Angle Orthod 2002;
72: 175179. 44. Brezniak N, Wasserstein A. Orthodontically induced inflammatory root resorption. Part II: The clinical aspects. Angle Orthod 2002; 72:180184. 45. Linge L, Linge BO. Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofacial Orthop 1991; 99: 3543. 46. Rahilly G, Price N. Nickel allergy and orthodontics. J Orthod 2003; 30: 171174. 47. Jones M, Chan C. The pain and discomfort experienced during orthodontic treatment: a randomized controlled clinical trial of two initial aligning arch wires. Am J Orthod Dentofacial Orthop 1992; 102: 373381. 48. Erdinc AM, Dincer B. Perception of pain during orthodontic treatment with fixed appliances. Eur J Orthod 2004; 26: 7985. 49. McSherry PF. The ectopic maxillary canine: a review. Br J Orthod 1998; 25: 209216. 50. Woloshyn H, Artun J, Kennedy DB, Joondeph DR. Pulpal and periodontal reactions to orthodontic alignment of palatally impacted canines. Angle Orthod 1994; 64: 257264. 51. Gould FK, Elliott TS, Foweraker J et al. Guidelines for the prevention of endocarditis: report of the Working Party of the British Society for Antimicrobial Chemotherapy. J Antimicrob Chemother 2006; 57: 10351042. 52. Brattstrom V, Ingelsson M, Aberg E. Treatment co-operation in orthodontic patients. Br J Orthod 1991; 18: 3742. 53. Houston WJB, Stephens CD, Tulley, WJ. Stability and retention. In: A Textbook of Orthodontics 2nd edition. Wright: Butterworth-Heinemann Ltd, 1992; pp.346356. 54. Shah AA. Postretention changes in mandibular crowding: a review of the literature. Am J Orthod Dentofacial Orthop 2003; 124: 298308. 55. Reynders RM. Orthodontics and temporomandibular disorders: a review of the literature (19661988). Am J Orthod Dentofacial Orthop 1990; 97: 463471. 56. Sadowsky CS. The risk of orthodontic treatment for producing temporomandibular mandibular disorders: a literature overview. Am J Orthod Dentofacial Orthop 1992; 10: 983. 57. Egermark I, Carlsson GE, Magnusson T. A prospective long-term study of signs and symptoms of temporomandibular disorders in patients who received orthodontic treatment in childhood. Angle Orthod 2005; 75: 645650. 58. Sadowsky C, BeGole EA. Long-term effects of orthodontic treatment on periodontal health. Am J Orthod 1981; 80: 156-172. 59. O'Brien K, Wright J, Conboy F et al. Effectiveness of early orthodontic treatment with the Twin-block appliance: a multicentre, randomized, controlled trial. Part 2: Psychosocial effects. Am J Orthod Dentofacial Orthop 2003; 124: 488494. 60. Koroluk LD, Tulloch JF, Phillips C. Incisor trauma and early treatment for Class II Division 1 malocclusion. Am J Orthod Dentofacial Orthop 2003; 123: 117125.
You might also like
- 1989 The Development of An Index of Orthodontic Treatment PriorityNo ratings yet1989 The Development of An Index of Orthodontic Treatment Priority12 pages
- An Arithmetic Crown-Down Dynamic Tactile Instrumentation Technique: A Case Report of An S-Shaped Root Canal100% (2)An Arithmetic Crown-Down Dynamic Tactile Instrumentation Technique: A Case Report of An S-Shaped Root Canal8 pages
- Artificial Intelligence in Dentistry Current Applications and Future PerspectivesNo ratings yetArtificial Intelligence in Dentistry Current Applications and Future Perspectives10 pages
- Consent in Orthodontics: Advice Sheet 4 British Orthodontic SocietyNo ratings yetConsent in Orthodontics: Advice Sheet 4 British Orthodontic Society10 pages
- Treating the Dental Patient with a Developmental DisorderFrom EverandTreating the Dental Patient with a Developmental DisorderKaren A. RaposaNo ratings yet
- Management of Endodontic Complications: From Diagnosis to PrognosisFrom EverandManagement of Endodontic Complications: From Diagnosis to PrognosisNo ratings yet
- INTERDISCIPLINARY APPROACH IN THE TREATMENT OF IMPACTED CANINES - Review and A Case Report PDFNo ratings yetINTERDISCIPLINARY APPROACH IN THE TREATMENT OF IMPACTED CANINES - Review and A Case Report PDF6 pages
- Extractions, Retention and Stability The Search For Orthodontic Truth Sheldon PeckNo ratings yetExtractions, Retention and Stability The Search For Orthodontic Truth Sheldon Peck7 pages
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkNo ratings yetProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok Ok5 pages
- Orthodontic Treatment: Patient Information LeafletNo ratings yetOrthodontic Treatment: Patient Information Leaflet2 pages
- Pre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesNo ratings yetPre-And Postoperative Management Techniques. Before and After. Part 1: Medical Morbidities6 pages
- Class II Treatment Efficiency in U4 Extraction & Non Extraction Protocols 2007No ratings yetClass II Treatment Efficiency in U4 Extraction & Non Extraction Protocols 20079 pages
- Dental Trauma Guidelines I Fractures and Luxations - Flores Anderson AndreassenNo ratings yetDental Trauma Guidelines I Fractures and Luxations - Flores Anderson Andreassen6 pages
- Dental Extractions and Bisphosphonates: The Assess-Ment, Consent and Management, A Proposed AlgorithmNo ratings yetDental Extractions and Bisphosphonates: The Assess-Ment, Consent and Management, A Proposed Algorithm6 pages
- Orthodontics & Dentofacial Orthopaedics MDS - 403No ratings yetOrthodontics & Dentofacial Orthopaedics MDS - 40315 pages
- CURRICULUM Orodontie - Anul V Sem X2149096871966833453No ratings yetCURRICULUM Orodontie - Anul V Sem X214909687196683345318 pages
- BSDH Domiciliary Guidelines August 2009No ratings yetBSDH Domiciliary Guidelines August 200940 pages
- Orthodontics: History Taking and ExaminationNo ratings yetOrthodontics: History Taking and Examination39 pages
- Certification Program in Orthodontics: 3 ModulesNo ratings yetCertification Program in Orthodontics: 3 Modules14 pages
- Management of Impacted Maxillary Canines Using Mandibular Anchorage100% (1)Management of Impacted Maxillary Canines Using Mandibular Anchorage4 pages
- Saliva / Orthodontic Courses by Indian Dental AcademyNo ratings yetSaliva / Orthodontic Courses by Indian Dental Academy191 pages
- What Is A Complete Denture? - My Dental Technology NotesNo ratings yetWhat Is A Complete Denture? - My Dental Technology Notes9 pages
- Burstone's Biomechanical Foundation of Clinical Orthodontics: Second EditionFrom EverandBurstone's Biomechanical Foundation of Clinical Orthodontics: Second EditionNo ratings yet
- World Journal of Orthodontics-2010 All Issues67% (3)World Journal of Orthodontics-2010 All Issues358 pages
- Mode of Action of Functional Appliances / Orthodontic Courses by Indian Dental AcademyNo ratings yetMode of Action of Functional Appliances / Orthodontic Courses by Indian Dental Academy116 pages
- Stability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesNo ratings yetStability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed Appliances8 pages
- Orofacial Dysfunction Nonnutritive Sucking Hab 2022 American Journal of OrtNo ratings yetOrofacial Dysfunction Nonnutritive Sucking Hab 2022 American Journal of Ort8 pages
- Comparison of Anterior Retraction and Anchorage Control BetweenNo ratings yetComparison of Anterior Retraction and Anchorage Control Between44 pages
- Impact of Wearing Fixed Orthodontic Appliances On Quality of Life Among Adolescents: Case-Control StudyNo ratings yetImpact of Wearing Fixed Orthodontic Appliances On Quality of Life Among Adolescents: Case-Control Study6 pages
- And Pharyngeal Airway Passage Dimension Changes Following Twin-Block TherapyNo ratings yetAnd Pharyngeal Airway Passage Dimension Changes Following Twin-Block Therapy24 pages
- Effect of Serial Extraction Alone On Crowding...No ratings yetEffect of Serial Extraction Alone On Crowding...6 pages
- Dental Age Estimation of 6-15 Year Old Indian Children Using Demirjian MethodNo ratings yetDental Age Estimation of 6-15 Year Old Indian Children Using Demirjian Method4 pages
- KLSINSTDENT - Dentoalveolar Instruments ClarizioNo ratings yetKLSINSTDENT - Dentoalveolar Instruments Clarizio28 pages
- 1972 Ricketts. An Overview of Cornputerized CephalometricsNo ratings yet1972 Ricketts. An Overview of Cornputerized Cephalometrics28 pages
- Lingual Orthodontics Understanding The Issues Is The Ke - 2018 - Seminars in or PDFNo ratings yetLingual Orthodontics Understanding The Issues Is The Ke - 2018 - Seminars in or PDF15 pages
- Resume of Periodontist, Prof. Dr. Ninad MoonNo ratings yetResume of Periodontist, Prof. Dr. Ninad Moon8 pages























































































- 1989 The Development of An Index of Orthodontic Treatment Priority1989 The Development of An Index of Orthodontic Treatment Priority
- An Arithmetic Crown-Down Dynamic Tactile Instrumentation Technique: A Case Report of An S-Shaped Root CanalAn Arithmetic Crown-Down Dynamic Tactile Instrumentation Technique: A Case Report of An S-Shaped Root Canal
- Artificial Intelligence in Dentistry Current Applications and Future PerspectivesArtificial Intelligence in Dentistry Current Applications and Future Perspectives
- Consent in Orthodontics: Advice Sheet 4 British Orthodontic SocietyConsent in Orthodontics: Advice Sheet 4 British Orthodontic Society
- Treating the Dental Patient with a Developmental DisorderFrom EverandTreating the Dental Patient with a Developmental Disorder
- Management of Endodontic Complications: From Diagnosis to PrognosisFrom EverandManagement of Endodontic Complications: From Diagnosis to Prognosis
- Prosthetic Treatment of the Edentulous PatientFrom EverandProsthetic Treatment of the Edentulous Patient
- INTERDISCIPLINARY APPROACH IN THE TREATMENT OF IMPACTED CANINES - Review and A Case Report PDFINTERDISCIPLINARY APPROACH IN THE TREATMENT OF IMPACTED CANINES - Review and A Case Report PDF
- Extractions, Retention and Stability The Search For Orthodontic Truth Sheldon PeckExtractions, Retention and Stability The Search For Orthodontic Truth Sheldon Peck
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok Ok
- Orthodontic Treatment: Patient Information LeafletOrthodontic Treatment: Patient Information Leaflet
- Pre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesPre-And Postoperative Management Techniques. Before and After. Part 1: Medical Morbidities
- Class II Treatment Efficiency in U4 Extraction & Non Extraction Protocols 2007Class II Treatment Efficiency in U4 Extraction & Non Extraction Protocols 2007
- Dental Trauma Guidelines I Fractures and Luxations - Flores Anderson AndreassenDental Trauma Guidelines I Fractures and Luxations - Flores Anderson Andreassen
- Dental Extractions and Bisphosphonates: The Assess-Ment, Consent and Management, A Proposed AlgorithmDental Extractions and Bisphosphonates: The Assess-Ment, Consent and Management, A Proposed Algorithm
- CURRICULUM Orodontie - Anul V Sem X2149096871966833453CURRICULUM Orodontie - Anul V Sem X2149096871966833453
- Management of Impacted Maxillary Canines Using Mandibular AnchorageManagement of Impacted Maxillary Canines Using Mandibular Anchorage
- Saliva / Orthodontic Courses by Indian Dental AcademySaliva / Orthodontic Courses by Indian Dental Academy
- What Is A Complete Denture? - My Dental Technology NotesWhat Is A Complete Denture? - My Dental Technology Notes
- Burstone's Biomechanical Foundation of Clinical Orthodontics: Second EditionFrom EverandBurstone's Biomechanical Foundation of Clinical Orthodontics: Second Edition
- Mode of Action of Functional Appliances / Orthodontic Courses by Indian Dental AcademyMode of Action of Functional Appliances / Orthodontic Courses by Indian Dental Academy
- Stability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesStability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed Appliances
- Orofacial Dysfunction Nonnutritive Sucking Hab 2022 American Journal of OrtOrofacial Dysfunction Nonnutritive Sucking Hab 2022 American Journal of Ort
- Comparison of Anterior Retraction and Anchorage Control BetweenComparison of Anterior Retraction and Anchorage Control Between
- Impact of Wearing Fixed Orthodontic Appliances On Quality of Life Among Adolescents: Case-Control StudyImpact of Wearing Fixed Orthodontic Appliances On Quality of Life Among Adolescents: Case-Control Study
- And Pharyngeal Airway Passage Dimension Changes Following Twin-Block TherapyAnd Pharyngeal Airway Passage Dimension Changes Following Twin-Block Therapy
- Dental Age Estimation of 6-15 Year Old Indian Children Using Demirjian MethodDental Age Estimation of 6-15 Year Old Indian Children Using Demirjian Method
- 1972 Ricketts. An Overview of Cornputerized Cephalometrics1972 Ricketts. An Overview of Cornputerized Cephalometrics
- Lingual Orthodontics Understanding The Issues Is The Ke - 2018 - Seminars in or PDFLingual Orthodontics Understanding The Issues Is The Ke - 2018 - Seminars in or PDF