Acls Lecture
Acls Lecture
Download as docx, pdf, or txt
You might also like
- Keith RN Asthma Case StudyDocument16 pagesKeith RN Asthma Case StudyCHARLES MAINANo ratings yet
- Summarised Checkpoint Biology NotesDocument48 pagesSummarised Checkpoint Biology NotesTanvi SharmaNo ratings yet
- UntitledDocument1 pageUntitledZaakira SyedNo ratings yet
- Chapter 24 Management of Patients With Structural, Infectious, and Inflammatory Cardiac DisordersDocument41 pagesChapter 24 Management of Patients With Structural, Infectious, and Inflammatory Cardiac Disordersسلطان محمد فوزي سلمانNo ratings yet
- Pepp Als PretestDocument4 pagesPepp Als PretestDave BoppNo ratings yet
- Myocardial Infarction With CABG Concept MapDocument1 pageMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- Nursing Responsibilities in Handling AntibioticsDocument4 pagesNursing Responsibilities in Handling Antibioticsrichardmd20% (1)
- Cardiac DrugsDocument3 pagesCardiac Drugsmikaela_pascuaNo ratings yet
- 2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes Algorithmms_lezahNo ratings yet
- This Study Resource Was: Chamberlain College of NursingDocument5 pagesThis Study Resource Was: Chamberlain College of NursingHugsNo ratings yet
- VATI Mental Health RemediationDocument2 pagesVATI Mental Health RemediationestberryNo ratings yet
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDocument3 pagesDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- The Strategy of Preventive Medicine: Geoffrey RoseDocument8 pagesThe Strategy of Preventive Medicine: Geoffrey RosePaulNo ratings yet
- PcicardDocument2 pagesPcicardWahdat100% (2)
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- ACLS ModuleDocument68 pagesACLS ModuleSalah ElbadawyNo ratings yet
- Critical Care Nurses' Knowledge RegardingManagement of Patients WithAtrial Fibrillation at Baghdad CityDocument5 pagesCritical Care Nurses' Knowledge RegardingManagement of Patients WithAtrial Fibrillation at Baghdad CityIOSRjournalNo ratings yet
- Chronic Renal Failure (Handout)Document3 pagesChronic Renal Failure (Handout)rhizzyNo ratings yet
- Drug Overdose and ManagementDocument9 pagesDrug Overdose and ManagementKoRnflakes100% (1)
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
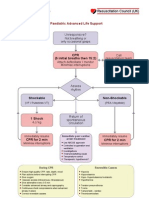
- PalsDocument1 pagePalslordroentgenNo ratings yet
- NLE Poisons and AntidotesDocument2 pagesNLE Poisons and AntidotesGodfrey Franco100% (1)
- AclsDocument62 pagesAclsAlemayehu beharuNo ratings yet
- (Advanced Cardiac Life Support) : ACLS Algorithms 2018Document18 pages(Advanced Cardiac Life Support) : ACLS Algorithms 2018cristina100% (1)
- ACLS Study GuideDocument30 pagesACLS Study GuidemmmmzNo ratings yet
- ECPRRole CardsDocument17 pagesECPRRole Cardsghg sddNo ratings yet
- Cardiovascular Disorders: BY: Maximin A. Pomperada, RN, MANDocument65 pagesCardiovascular Disorders: BY: Maximin A. Pomperada, RN, MANRellie Castro100% (1)
- Acls Topic Wise Mcqs - CompressDocument40 pagesAcls Topic Wise Mcqs - Compressezzat salemNo ratings yet
- Cardiovascular Disorders 1Document44 pagesCardiovascular Disorders 1Nader Smadi100% (1)
- TraumaDocument12 pagesTraumagibreilNo ratings yet
- 15 Item ACLS Drill With RationaleDocument12 pages15 Item ACLS Drill With RationaleLj Ferolino100% (1)
- Dysrhythmias: Se Admin Anticoagulante, Cardioversion As PrescribedDocument10 pagesDysrhythmias: Se Admin Anticoagulante, Cardioversion As Prescribedyaneidys perezNo ratings yet
- American Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityDocument49 pagesAmerican Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityZulkarnainBustamamNo ratings yet
- Advanced Cardiac Life SupportDocument13 pagesAdvanced Cardiac Life SupportEldonVinceIsidroNo ratings yet
- Dvanced Ardiovascular Ife Upport: A C L SDocument10 pagesDvanced Ardiovascular Ife Upport: A C L SErica Jane100% (1)
- Study Guide HESI CommunityDocument29 pagesStudy Guide HESI CommunityBeth Ann100% (1)
- Cardiac DisordersDocument38 pagesCardiac Disordersprototypeallhell100% (1)
- DYSRHYTHMIASDocument9 pagesDYSRHYTHMIASgudobenNo ratings yet
- Set 1Document62 pagesSet 1Alyssa MontimorNo ratings yet
- Clinical Case Study - Online Discussion Form Fall 2020-1Document14 pagesClinical Case Study - Online Discussion Form Fall 2020-1Sabrina Odies100% (1)
- Nursing Review Bullets HighlightsDocument65 pagesNursing Review Bullets HighlightsEuanne OrellanoNo ratings yet
- Neurological Manifestations of HIVDocument34 pagesNeurological Manifestations of HIVashuNo ratings yet
- Necrotizing Otitis 2022Document20 pagesNecrotizing Otitis 2022asmashNo ratings yet
- RNDocument16 pagesRNrunnermn100% (1)
- Shock NotesDocument5 pagesShock NotesAlyss Wallschleger100% (1)
- ACLS Full Lesson PlansDocument60 pagesACLS Full Lesson PlanslateifaNo ratings yet
- Acls FixDocument20 pagesAcls Fixluthfi adityaNo ratings yet
- Pals Que Estion and Answer FullDocument31 pagesPals Que Estion and Answer FullNeo Latoya MadunaNo ratings yet
- High Alert MedicationsDocument17 pagesHigh Alert MedicationsJoanna Marie Datahan EstomoNo ratings yet
- ATCN 2013 Faculty Update (July 23)Document15 pagesATCN 2013 Faculty Update (July 23)Opi SaNg MadRidistas100% (1)
- AclsDocument85 pagesAclsJulia CostaNo ratings yet
- PerfusionDocument9 pagesPerfusionAmanda Brittain100% (2)
- Formative Assessment FinalDocument5 pagesFormative Assessment FinalJonathan YeohNo ratings yet
- Advanced Life Support Training and AssessmentDocument6 pagesAdvanced Life Support Training and AssessmentwilmaNo ratings yet
- NSG 117 PerfusionDocument55 pagesNSG 117 PerfusionAnonymous UJEyEsNo ratings yet
- HeartCode BLSDocument5 pagesHeartCode BLSJohn DiggNo ratings yet
- Advanced Life SupportDocument65 pagesAdvanced Life SupportPrasad Narangoda100% (1)
- Non Classical Research On Vitamin D PresentationDocument13 pagesNon Classical Research On Vitamin D PresentationJoshua AfolabiNo ratings yet
- Cardiac FT: ResultsDocument26 pagesCardiac FT: ResultsBillynTarplainNo ratings yet
- Sample Acls For DummiesDocument3 pagesSample Acls For DummiesTodd Cole100% (1)
- ACLS Simulation ScenariosDocument14 pagesACLS Simulation ScenariosVanessa HermioneNo ratings yet
- Nclex & Cgfns Review Bullets 2Document12 pagesNclex & Cgfns Review Bullets 2blazegomezNo ratings yet
- Frequently Asked ECG & X-Ray QuestionsDocument9 pagesFrequently Asked ECG & X-Ray Questionsزكريا عمرNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Congestive Cardiac Failure: DR Romila Chimoriya Lecturer Department of PediatricsDocument21 pagesCongestive Cardiac Failure: DR Romila Chimoriya Lecturer Department of PediatricsDhiraj PantNo ratings yet
- Clinical Case Presentation: Martin C. Burke, DODocument24 pagesClinical Case Presentation: Martin C. Burke, DONicole.INo ratings yet
- Circulatory SystemDocument51 pagesCirculatory SystemTina TalmadgeNo ratings yet
- PantoprazoleDocument10 pagesPantoprazoleTheresa AbrilloNo ratings yet
- American Dispensatory, Harvey Wickes Felter, M.D., and John Uri Lloyd, PH.D.)Document11 pagesAmerican Dispensatory, Harvey Wickes Felter, M.D., and John Uri Lloyd, PH.D.)howbertdsNo ratings yet
- Pie Chart Showing Percentage of Participants With AsthmaDocument6 pagesPie Chart Showing Percentage of Participants With AsthmaJay Queue JonnyNo ratings yet
- Animal TransportDocument20 pagesAnimal TransportFeranmi AkinboboyeNo ratings yet
- Cvs 253Document253 pagesCvs 253CHALIE MEQUNo ratings yet
- Vethathiriyam - Wellness & LongevityDocument2 pagesVethathiriyam - Wellness & LongevityaleppyNo ratings yet
- NCLEX Notes : Raynaud's Phenomenon - Cold Temperatures or Strong Emotions CauseDocument10 pagesNCLEX Notes : Raynaud's Phenomenon - Cold Temperatures or Strong Emotions CauseDesi Marian100% (12)
- Anesthetic Management For Woman With Single Ventricle Heart After BCPS Who Undergoes Curretage ProcedureDocument3 pagesAnesthetic Management For Woman With Single Ventricle Heart After BCPS Who Undergoes Curretage ProcedureAnastasia AngelaNo ratings yet
- Heart Disease Prediction System Using Machine Learning: Ranjit Shrestha and Jyotir Moy ChatterjeeDocument18 pagesHeart Disease Prediction System Using Machine Learning: Ranjit Shrestha and Jyotir Moy ChatterjeeDarshan PatilNo ratings yet
- LL - Guideline VSD WebsiteDocument30 pagesLL - Guideline VSD WebsiteNesya PutriNo ratings yet
- Structure/Function Relationships in Medical PhysiologyDocument42 pagesStructure/Function Relationships in Medical PhysiologyАлазар ЗелелеNo ratings yet
- Dr. Adolfo Duarte - As 6 Coisas Que Você Tem Que Fazer para Ter Uma Saúde Fenomenal (2014)Document62 pagesDr. Adolfo Duarte - As 6 Coisas Que Você Tem Que Fazer para Ter Uma Saúde Fenomenal (2014)mnevesmaNo ratings yet
- Exercise Standards For Testing and TrainingDocument62 pagesExercise Standards For Testing and TrainingRelviGuzmanApazaNo ratings yet
- Lecture and Q and A Series in Medico Legal PDFDocument942 pagesLecture and Q and A Series in Medico Legal PDFArjhade Sarita100% (2)
- Aspects of DeathDocument45 pagesAspects of DeathDonzzkie DonNo ratings yet
- Physiology Shet #7&8Document12 pagesPhysiology Shet #7&8Rawan Abu HammourNo ratings yet
- Advanced Gynecologic Endoscopy: Edited by Atef DarwishDocument344 pagesAdvanced Gynecologic Endoscopy: Edited by Atef DarwishSandu Alexandra100% (2)
- First AidDocument12 pagesFirst Aidhvjimjim2No ratings yet
- Judi SatoriDocument27 pagesJudi SatoriAlina TudoracheNo ratings yet
- Simulated Exam RationalesDocument20 pagesSimulated Exam Rationalesrhymes2u100% (3)
- The Expanded Biology of SerotoninDocument15 pagesThe Expanded Biology of Serotoninnilberto2No ratings yet
- Nur 111 Session 6 Sas 1Document12 pagesNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Heart Diseases Diabetes Mellitus Substance Abuse Hiv/Aids RH Sensitization AnemiaDocument46 pagesHeart Diseases Diabetes Mellitus Substance Abuse Hiv/Aids RH Sensitization Anemiarevie67% (3)