GENERAL LINE of Treatment UREA AMMONIA SALT - poISONING
GENERAL LINE of Treatment UREA AMMONIA SALT - poISONING
At a glance
Powered by AI
The key takeaways are that poisoning is always an emergency and needs to be managed immediately. Supportive care to maintain vital functions like respiration and circulation is important until specific treatment can be given. ABC (Airway, Breathing, Circulation) is important.
The general principles of treatment of poisoning include managing the emergency phases first to improve the animal's condition through supportive care. Prompt removal or neutralization of the poison while maintaining vital body functions is important until slow-acting specific treatment can be given.
Methods to remove poison from the stomach include gastric lavage and in ruminants, manual gastric emptying after emergency gastrotomy/ruminotomy. Gastric lavage should be done soon after ingestion and is indicated in small animals like dogs within 2-4 hours of ingestion.
You might also like
- Australian Medicines Handbook Pty LTDDocument23 pagesAustralian Medicines Handbook Pty LTDCleonSciaxeNo ratings yet
- Classification and Dosage of Antimicrobial Agents in Veterinary MedicineDocument24 pagesClassification and Dosage of Antimicrobial Agents in Veterinary MedicineSunil0% (1)
- Nitric Oxide Pharmacology .Document130 pagesNitric Oxide Pharmacology .SunilNo ratings yet
- Restraining of ReptilesDocument85 pagesRestraining of ReptilesSunil100% (1)
- UOP Oleflex Process For Propylene Production: PetrochemicalDocument2 pagesUOP Oleflex Process For Propylene Production: PetrochemicalWong Yee Sun50% (2)
- Drugs Acting On Gastrointestinal SystemDocument41 pagesDrugs Acting On Gastrointestinal SystemDivya JoyNo ratings yet
- Drugs Affecting Calcium BalanceDocument63 pagesDrugs Affecting Calcium BalanceRd Chandane100% (1)
- Chemical Nature of Natural Drugs: Unit 8Document48 pagesChemical Nature of Natural Drugs: Unit 8Preeti VermaNo ratings yet
- Chemotherapy For Protozoal InfectionsDocument32 pagesChemotherapy For Protozoal InfectionsJia YingNo ratings yet
- Tandard Perating Rocedure: RotarodDocument2 pagesTandard Perating Rocedure: RotarodRohan PalNo ratings yet
- Hematinics: Dr. Monalisa Mondal Demonstrator Department of PharmacologyDocument28 pagesHematinics: Dr. Monalisa Mondal Demonstrator Department of PharmacologyShirsh JauriharNo ratings yet
- Practical 1-Far 161-FinishDocument10 pagesPractical 1-Far 161-FinishZulkifli Khairuddin100% (1)
- Antiadrenergic DrugsDocument19 pagesAntiadrenergic DrugsshivanshpandeNo ratings yet
- Bioassay of Histamine by Using Isolated Chicken Ileum: Correspondence For Author Rakesh B. DaudeDocument5 pagesBioassay of Histamine by Using Isolated Chicken Ileum: Correspondence For Author Rakesh B. DaudeCelsia NestiNo ratings yet
- Drugs Acting On Digestive System of AnimalsDocument11 pagesDrugs Acting On Digestive System of AnimalsSunil100% (4)
- Glucose (Mono Reagent) (GOD/POD Method) : For in Vitro Diagnostic Use OnlyDocument2 pagesGlucose (Mono Reagent) (GOD/POD Method) : For in Vitro Diagnostic Use OnlySourav MondalNo ratings yet
- GIT DrugsDocument57 pagesGIT Drugssalva sambaaNo ratings yet
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22No ratings yet
- Pharmacology Renal DiureticsDocument24 pagesPharmacology Renal Diureticskpsuan100% (1)
- Introduction of PharmacotherapyDocument51 pagesIntroduction of PharmacotherapyJeffrey RamosNo ratings yet
- general systemic states د.عزيزةDocument75 pagesgeneral systemic states د.عزيزةAhmed Hamdy NaDa100% (2)
- Screening Methods - Analgesic DrugsDocument28 pagesScreening Methods - Analgesic DrugsKeerthi Sagar100% (1)
- Unit 8 Drugs Acting On The Endocrine SystemDocument26 pagesUnit 8 Drugs Acting On The Endocrine SystemTherese Margarette SantiagoNo ratings yet
- Mouse Handling Techniques PacketDocument24 pagesMouse Handling Techniques PacketLovely Ann AyapanaNo ratings yet
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineDocument21 pagesDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Veterinary Pharmacology Toxicology PDFDocument11 pagesVeterinary Pharmacology Toxicology PDFSandeep Kumar Chaudhary55% (11)
- Screening ShortDocument30 pagesScreening Shortjignesh100% (1)
- Top Drugs: 1. ACETAMINOPHEN (Tylenol)Document12 pagesTop Drugs: 1. ACETAMINOPHEN (Tylenol)epingNo ratings yet
- Cytotoxic Drugs: Pharm. Dr. Ezekiel EfeobhokhanDocument24 pagesCytotoxic Drugs: Pharm. Dr. Ezekiel EfeobhokhanjonaNo ratings yet
- 01 Introduction To Clinical Toxicology (1) - 5Document295 pages01 Introduction To Clinical Toxicology (1) - 5Lyadelou FortuNo ratings yet
- MetronidazoleDocument16 pagesMetronidazoleAnshul Arora100% (2)
- Experimental Pharmacology (PDFDrive)Document168 pagesExperimental Pharmacology (PDFDrive)Priya MohiteNo ratings yet
- Ward RoundDocument2 pagesWard RoundAnonymous whcvnPBeQNo ratings yet
- Animal Used For Experimental PharmacologyDocument3 pagesAnimal Used For Experimental PharmacologyAishwarya PatilNo ratings yet
- Hand Eczema - PPT 59 CKDocument23 pagesHand Eczema - PPT 59 CKGrm MotorsNo ratings yet
- Review Notes For Diabetes MellitusDocument8 pagesReview Notes For Diabetes MellitusEditha LucasNo ratings yet
- Principles of PharmacologyDocument9 pagesPrinciples of Pharmacologybencleese100% (1)
- Anti-Viral Drugs AltDocument42 pagesAnti-Viral Drugs AltSidraNo ratings yet
- CPCSEA GuidelinesDocument27 pagesCPCSEA GuidelinesArchana VanjariNo ratings yet
- ChronopharmacologyDocument5 pagesChronopharmacologyDRx Ijajul HussainNo ratings yet
- Anti LeproticDocument9 pagesAnti LeproticMeenakshi shARMANo ratings yet
- SulfonamidesDocument14 pagesSulfonamidescamzyyy30No ratings yet
- Pharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsDocument48 pagesPharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsAmanuel MaruNo ratings yet
- I. Practicals: Practical Exam Pattern For Ii Mbbs Pharmacology Cbme Batch (2019)Document2 pagesI. Practicals: Practical Exam Pattern For Ii Mbbs Pharmacology Cbme Batch (2019)santhoshNo ratings yet
- Screening MethodsDocument1 pageScreening MethodsManoj chalageriNo ratings yet
- Pharmaco DynamicsDocument7 pagesPharmaco DynamicsDavid NicholasNo ratings yet
- Orientation To Pharmacy-2011Document51 pagesOrientation To Pharmacy-2011khairi_mustafa1704No ratings yet
- ZOOTOXINSDocument72 pagesZOOTOXINSSunil86% (7)
- Organophosphate PoisoningDocument40 pagesOrganophosphate PoisoningMadhu Sudhan PandeyaNo ratings yet
- Antihelminths: DR Japhet Mangoyi Department of Clinical PharmacologyDocument15 pagesAntihelminths: DR Japhet Mangoyi Department of Clinical PharmacologyMitchelle SaurambaNo ratings yet
- Pharmacotherapy of Myocardial InfaractionDocument69 pagesPharmacotherapy of Myocardial InfaractionNikhil KamdiNo ratings yet
- Polioencephalomalacia in GoatsDocument20 pagesPolioencephalomalacia in GoatsUmesh GopalanNo ratings yet
- Pharmacology Practical Manual - Student Copy2Document11 pagesPharmacology Practical Manual - Student Copy2NareshNo ratings yet
- Biomed LDH 51Document2 pagesBiomed LDH 51D Mero LabNo ratings yet
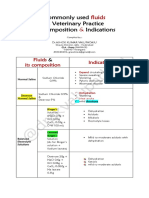
- Common IV Fluids at Composition & IndicationsDocument2 pagesCommon IV Fluids at Composition & IndicationsNilesh SuryawanshiNo ratings yet
- Pharmacology Lecture - 15 Inotropic DrugsDocument3 pagesPharmacology Lecture - 15 Inotropic DrugsChris Queiklin100% (1)
- Pharmacology of The GIT System: CIC Ragasa, RN-MDDocument70 pagesPharmacology of The GIT System: CIC Ragasa, RN-MDCarmencita Ileen Ragasa - AhmedNo ratings yet
- HOMEOPATHY TREATMENT OF VARIOUS DISEASES OF POULTRY (BROILERS & LAYERS) - Pashudhan PrahareeDocument1 pageHOMEOPATHY TREATMENT OF VARIOUS DISEASES OF POULTRY (BROILERS & LAYERS) - Pashudhan PrahareeAashish SatyamNo ratings yet
- Health Promotion and Education in School - VL PDFDocument28 pagesHealth Promotion and Education in School - VL PDFAshu AmmuNo ratings yet
- Anti Hypertensive DrugsDocument3 pagesAnti Hypertensive DrugsMu'allim HawaryNo ratings yet
- 71134lecture 6Document27 pages71134lecture 6azizNo ratings yet
- Fluorosis Phosphorous Nitrate Toxicity in AnimalsDocument55 pagesFluorosis Phosphorous Nitrate Toxicity in AnimalsSunilNo ratings yet
- Mycotoxins in Animal HealthDocument103 pagesMycotoxins in Animal HealthSunil100% (3)
- VPT MCQ ForDocument10 pagesVPT MCQ ForSunilNo ratings yet
- Carbon Monoxide PoisoningDocument22 pagesCarbon Monoxide PoisoningSunilNo ratings yet
- Antiseptics and Disinfectants For Veterinary ClinicsDocument3 pagesAntiseptics and Disinfectants For Veterinary ClinicsSunil100% (5)
- Drugs in ReptilesDocument71 pagesDrugs in ReptilesSunil100% (1)
- Endocrine Vety PharmaDocument16 pagesEndocrine Vety PharmaSunilNo ratings yet
- VCI MSVE 2008 RegulationsDocument136 pagesVCI MSVE 2008 RegulationsSunil50% (2)
- Classification of AmphibiansDocument22 pagesClassification of AmphibiansSunilNo ratings yet
- Toxicological Investigation and Its Significance in Animal Health DiagnosisDocument8 pagesToxicological Investigation and Its Significance in Animal Health DiagnosisSunil100% (1)
- Drugs Acting On Respiratory System of AnimalsDocument8 pagesDrugs Acting On Respiratory System of AnimalsSunil100% (4)
- Site of Action of Drugs Acting On Adrenergic Neurohumoral Transmission PDFDocument1 pageSite of Action of Drugs Acting On Adrenergic Neurohumoral Transmission PDFSunilNo ratings yet
- Drugs Acting On Digestive System of AnimalsDocument11 pagesDrugs Acting On Digestive System of AnimalsSunil100% (4)
- Drugs Acting On Genitourinary System of AnimalsDocument44 pagesDrugs Acting On Genitourinary System of AnimalsSunilNo ratings yet
- Drugs Acting On Haematopoietic System of AnimalsDocument28 pagesDrugs Acting On Haematopoietic System of AnimalsSunil100% (1)
- Mycotoxins in Animal HealthDocument103 pagesMycotoxins in Animal HealthSunil100% (3)
- Toxicokinetics DynamicsDocument76 pagesToxicokinetics DynamicsSunil100% (1)
- Mercury Lead Arsenic Cadmium ToxicityDocument171 pagesMercury Lead Arsenic Cadmium ToxicitySunilNo ratings yet
- ZOOTOXINSDocument72 pagesZOOTOXINSSunil86% (7)
- Systemic Veterinary Pharmacology in A NutshellDocument165 pagesSystemic Veterinary Pharmacology in A NutshellSunil100% (1)
- Trematodes of Wild BirdsDocument5 pagesTrematodes of Wild BirdsSunilNo ratings yet
- LATHYRISM AND PHOTOSENSiTIZATIONDocument33 pagesLATHYRISM AND PHOTOSENSiTIZATIONSunilNo ratings yet
- Classification of AmphibiansDocument22 pagesClassification of AmphibiansSunil100% (1)
- AntiConvulsants Drugs in Brief PDFDocument28 pagesAntiConvulsants Drugs in Brief PDFSunilNo ratings yet
- Extinct and Endangered Animals OF INDIADocument8 pagesExtinct and Endangered Animals OF INDIASunil100% (2)
- Cestodes of Wild Birds PDFDocument5 pagesCestodes of Wild Birds PDFSunil100% (1)
- Pharmaco EconomicsDocument49 pagesPharmaco EconomicsSunil100% (1)
- 3CR12 Data Sheet 2021Document1 page3CR12 Data Sheet 2021Elcio VilanculoNo ratings yet
- Group 3 GunpowderDocument13 pagesGroup 3 GunpowderBrielle Shai CruzNo ratings yet
- Product Brochure Riken Keiki SP-220Document4 pagesProduct Brochure Riken Keiki SP-220Anticristh6666No ratings yet
- Chemical Process Industries (Reviewer)Document78 pagesChemical Process Industries (Reviewer)Emier VillanuevaNo ratings yet
- State-Of-The-Art Reverse Osmosis Desalination PDFDocument77 pagesState-Of-The-Art Reverse Osmosis Desalination PDFJaime MoralesNo ratings yet
- Rice and Einkorn Wheat Husks Reinforced Poly (Lactic Acid) (PLA)Document14 pagesRice and Einkorn Wheat Husks Reinforced Poly (Lactic Acid) (PLA)Sharol Nathalia Garzon SerranoNo ratings yet
- Activity No 2 - PHENOLDocument4 pagesActivity No 2 - PHENOLpharmaebooks100% (4)
- 04042016000000A Avesta 2205 Covered ElectrodesDocument1 page04042016000000A Avesta 2205 Covered Electrodesmeckup123No ratings yet
- Research Framework FormDocument2 pagesResearch Framework FormMohd Hafiz AhmadNo ratings yet
- GTL TechnologyDocument24 pagesGTL Technologychaitanya_scribd100% (1)
- 009 - Pages From (Library of Physico-Chemical Property Data) Carl L (Version 1)Document10 pages009 - Pages From (Library of Physico-Chemical Property Data) Carl L (Version 1)SHAILENDRANo ratings yet
- PSA 50 Paper PDFDocument5 pagesPSA 50 Paper PDFshashi kant kumarNo ratings yet
- 15.1 Bronsted-Lowry Acids and BasesDocument6 pages15.1 Bronsted-Lowry Acids and BasesPatricia de LeonNo ratings yet
- Welding Low Alloy SteelsDocument14 pagesWelding Low Alloy SteelsNanda Al Alif100% (1)
- EN15376Document1 pageEN15376Ganciarov MihaelaNo ratings yet
- Grade 9 Day 2 TB Dqas 2nd QuarterDocument10 pagesGrade 9 Day 2 TB Dqas 2nd QuarterKwen Ann OrtigzNo ratings yet
- IB Chemistry HL Topic4 Questions 1.: O C H H ODocument21 pagesIB Chemistry HL Topic4 Questions 1.: O C H H OKhang Thinh TRANNo ratings yet
- As Chemistry Unit 2 NotesDocument26 pagesAs Chemistry Unit 2 Notesizzy 12100% (1)
- Penyerahan Dan Penilaian TugasanDocument3 pagesPenyerahan Dan Penilaian TugasanKumaResan SubramaniamNo ratings yet
- Oxalic Acid - C2H2O4 - PubChemDocument61 pagesOxalic Acid - C2H2O4 - PubChemMuhamad Risky 'chan'No ratings yet
- SOPs For ChemicalsDocument7 pagesSOPs For ChemicalselizasunderNo ratings yet
- Pharmaceutical and Medicinal Organic Chemistry Lab: Unit OutcomesDocument8 pagesPharmaceutical and Medicinal Organic Chemistry Lab: Unit OutcomesJUDYANN PINEDANo ratings yet
- 1 WeldingDocument52 pages1 WeldingAYUSH PATRANo ratings yet
- One Bath One Stage Dyeing of Polyester / Cellulosic Blends.Document31 pagesOne Bath One Stage Dyeing of Polyester / Cellulosic Blends.sanjay shettiNo ratings yet
- 1950 Barton A N D Mugdan-Vinyl Chloride: J.S.C.I., 6g, March, 7Document5 pages1950 Barton A N D Mugdan-Vinyl Chloride: J.S.C.I., 6g, March, 7Evan Afrista Wiokartina PurbaNo ratings yet
- AlplexDocument2 pagesAlplexWHWENNo ratings yet
- Organic Chemistry: Exercise - I Exercise - Ii Exercise-Iii Exercise Iv Answer KeyDocument39 pagesOrganic Chemistry: Exercise - I Exercise - Ii Exercise-Iii Exercise Iv Answer KeyRaju SinghNo ratings yet
- SINTESIS SURFAKTAN METIL ESTER SULFONAT DARI METIL ESTER MINYAK BIJI KARET (Havea Brasiliensis) MELALUI REAKSI SULFONASI DENGAN PENGARUH VARIASI KATALISDocument6 pagesSINTESIS SURFAKTAN METIL ESTER SULFONAT DARI METIL ESTER MINYAK BIJI KARET (Havea Brasiliensis) MELALUI REAKSI SULFONASI DENGAN PENGARUH VARIASI KATALISAffiano AkbarNo ratings yet
- Concrete and PlasticsDocument14 pagesConcrete and PlasticsYna Marie GutierrezNo ratings yet