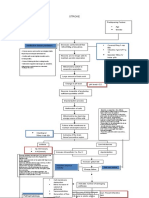
Hipotiroid
Hipotiroid
Download as ppt, pdf, or txt
You might also like
- Magic MouthwashDocument5 pagesMagic MouthwashAdiAri Rosiu100% (3)
- KeloidsDocument49 pagesKeloidslyn valerieNo ratings yet
- Abdominal Distention and Bloating - Kiiko Matsumoto Japanese StyleDocument4 pagesAbdominal Distention and Bloating - Kiiko Matsumoto Japanese StyleAWEDIOHEAD100% (2)
- Concept Map CVADocument1 pageConcept Map CVASuzette Rae Tate100% (3)
- Hipo HiperthyroidDocument49 pagesHipo HiperthyroidMuhammad Bilal Bin AmirNo ratings yet
- THyroid DisorderDocument39 pagesTHyroid DisorderT.A.BNo ratings yet
- Thyroid Function Tests: Drneha Mahajan MD PathologyDocument71 pagesThyroid Function Tests: Drneha Mahajan MD PathologyMukesh Kumar ChaudharyNo ratings yet
- '3'hyperthyroid and HypothyroidDocument42 pages'3'hyperthyroid and Hypothyroidafriskha bulawanNo ratings yet
- Anal Canal: Fissure in Ano HaemorrhoidsDocument37 pagesAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaNo ratings yet
- Mammary Gland Additional NotesDocument36 pagesMammary Gland Additional NotesjdfNo ratings yet
- Epidemiological and Clinical Characteristics of Hookwormrelated Cutaneous Larva MigransDocument9 pagesEpidemiological and Clinical Characteristics of Hookwormrelated Cutaneous Larva MigransShelyAzradNo ratings yet
- Thyroid CancerDocument39 pagesThyroid CancerFaheem SarwarNo ratings yet
- BCCA Febrile Neutropenia GuidelinesDocument2 pagesBCCA Febrile Neutropenia GuidelinesdenokayuMRNo ratings yet
- Chapter 56 Liver & Lung TrematodesDocument24 pagesChapter 56 Liver & Lung TrematodesbartsnewNo ratings yet
- Thyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistDocument30 pagesThyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistNurul HikmaNo ratings yet
- Anti Thyroid AntibodyDocument16 pagesAnti Thyroid AntibodyFritz HaryadiNo ratings yet
- Acute Tubular NecrosisDocument18 pagesAcute Tubular NecrosisAbdisalan hassanNo ratings yet
- Lichen PlanusDocument6 pagesLichen Planusأحمد عبد الوهابNo ratings yet
- Hemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoDocument18 pagesHemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoToraoNo ratings yet
- Efusi PleuraDocument51 pagesEfusi PleuraFarid FirnandaNo ratings yet
- Diagnosis and Management of Upper Gastrointestinal Bleeding PDFDocument10 pagesDiagnosis and Management of Upper Gastrointestinal Bleeding PDFKetut Suwadiaya P AdnyanaNo ratings yet
- Pathophysiology of Acute Liver FailureDocument39 pagesPathophysiology of Acute Liver Failurelefebi6403No ratings yet
- Hyperthyroidism (Thyrotoxicosis) : 郑州大学第一附院内分泌科 王守俊 Wang shou junDocument133 pagesHyperthyroidism (Thyrotoxicosis) : 郑州大学第一附院内分泌科 王守俊 Wang shou junapi-19916399No ratings yet
- Skin Bacterial Disease - Part-IIDocument11 pagesSkin Bacterial Disease - Part-IIElijah Wood100% (1)
- Trichinella Spiralis: A. ClassificationDocument6 pagesTrichinella Spiralis: A. ClassificationtinasheNo ratings yet
- Typhoid Fever Final 2Document28 pagesTyphoid Fever Final 2gAARaNo ratings yet
- Pancreatic Hormones and The Treatment of Diabetes MellitusDocument46 pagesPancreatic Hormones and The Treatment of Diabetes MellitusasmaNo ratings yet
- Thyroid DiseaseDocument30 pagesThyroid Diseasemy Lord JesusNo ratings yet
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- Regulasi Dan Mekanisme EndokrinDocument121 pagesRegulasi Dan Mekanisme Endokrinluthfiyya syafiqaNo ratings yet
- Doac Vs LMWHDocument6 pagesDoac Vs LMWHTry Enos OktafianNo ratings yet
- Cor Pulmonale - StatPearls - NCBI BookshelfDocument4 pagesCor Pulmonale - StatPearls - NCBI BookshelfAldi RafaelNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pratiwi S Gunawan, BDS., DDS., MDSC, PHDDocument53 pagesPratiwi S Gunawan, BDS., DDS., MDSC, PHDBima Ewando KabanNo ratings yet
- Redness Eye TreatmentDocument52 pagesRedness Eye TreatmentIka HandayaniNo ratings yet
- Grave - S Disease Edit OkDocument17 pagesGrave - S Disease Edit OkriniNo ratings yet
- Acute Lymphocytic LeukemiaDocument43 pagesAcute Lymphocytic LeukemiaCormeus BaltiNo ratings yet
- Von Willibrand DiseasesDocument34 pagesVon Willibrand DiseasesZulfadli Hussein100% (1)
- Algorithm Kel 3Document1 pageAlgorithm Kel 3Anonymous 5zeOnd1No ratings yet
- Papular UrticariaDocument10 pagesPapular UrticariaNuri Sakina SuhartoNo ratings yet
- D Dimer TestDocument20 pagesD Dimer TestHAJI RASHIDNo ratings yet
- Fisiologi Hemostasis Dan FibrinolisisDocument45 pagesFisiologi Hemostasis Dan FibrinolisisBesth To Frynce HutabaratNo ratings yet
- Thyroid Parathyroid (2012)Document83 pagesThyroid Parathyroid (2012)Hesti AnggrainiNo ratings yet
- Malaria PathogenesisDocument39 pagesMalaria PathogenesisRasyiqa TharifaNo ratings yet
- HypertyroidismDocument46 pagesHypertyroidismenriNo ratings yet
- Cor PulmonaleDocument14 pagesCor PulmonaleEvangelin MelvinNo ratings yet
- Science of Epidemiology-31.8.'16 Modified On 23.10.2016Document7 pagesScience of Epidemiology-31.8.'16 Modified On 23.10.2016Alankrit PatnaikNo ratings yet
- Toxoplasma and RubellaDocument37 pagesToxoplasma and RubellaHervi LaksariNo ratings yet
- Kholesistis & Kholelitiasis 30-11-14Document67 pagesKholesistis & Kholelitiasis 30-11-14Dian AzhariaNo ratings yet
- HepatitisDocument46 pagesHepatitisGusti Tirtha Drag JrNo ratings yet
- Biomarker SepsisDocument18 pagesBiomarker SepsisSukma EffendyNo ratings yet
- C+F-Spirometra İnfection in Cats and DogsDocument5 pagesC+F-Spirometra İnfection in Cats and Dogstaner_soysurenNo ratings yet
- Disorder of Sexual DevelopmentDocument14 pagesDisorder of Sexual DevelopmentPutri Mulia Hasibuan100% (1)
- Praktikum MalariaDocument22 pagesPraktikum MalariaGeniaaldafitriaasgen100% (1)
- KriptorkismusDocument14 pagesKriptorkismusMutiara Prima DianaNo ratings yet
- Filariasis: Dr. Suhaemi, SPPD, FinasimDocument30 pagesFilariasis: Dr. Suhaemi, SPPD, FinasimErreli K. KhusumawerdanieNo ratings yet
- Phylum Platyhelminthes (Flatworms) : Important InformationDocument26 pagesPhylum Platyhelminthes (Flatworms) : Important InformationYoussef EmadNo ratings yet
- Thyroid DiseasesDocument76 pagesThyroid DiseasesSolomon Fallah Foa SandyNo ratings yet
- Primary Biliary CholangitisDocument23 pagesPrimary Biliary CholangitisAbdul hadiNo ratings yet
- Hepatocellular CarcinomaDocument62 pagesHepatocellular CarcinomaWilliams Emmanuel AdeyeyeNo ratings yet
- AMLDocument19 pagesAMLquerokeropi100% (1)
- Pathophysiology of Fever-Tropmed2013Document24 pagesPathophysiology of Fever-Tropmed2013Yessy Dwi Oktavia100% (1)
- Endocrinology Board Review: Thyroid DisordersDocument46 pagesEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoNo ratings yet
- Clinical Manifestations and Diagnosis of Acute Pancreatitis PDFDocument32 pagesClinical Manifestations and Diagnosis of Acute Pancreatitis PDFChumas VidalNo ratings yet
- broschuere_diabetes_mellitus_englischDocument5 pagesbroschuere_diabetes_mellitus_englischtainurratulNo ratings yet
- The Dental Effects of Head and Neck Rhabdomyosarcoma Treatment - A Case SeriesDocument6 pagesThe Dental Effects of Head and Neck Rhabdomyosarcoma Treatment - A Case SeriesMohammad Abdulmon’emNo ratings yet
- A Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirDocument12 pagesA Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirDavit SoesantoNo ratings yet
- Auricular Acupuncture or Ear Acupuncture: Acu + Puncture !?!?Document2 pagesAuricular Acupuncture or Ear Acupuncture: Acu + Puncture !?!?DanNo ratings yet
- Care of Unconscious PatientDocument5 pagesCare of Unconscious PatientRuchika Kaushal67% (3)
- Inflammatory Bowel DiseaseDocument15 pagesInflammatory Bowel DiseaseYanushka Bruce HerathNo ratings yet
- Pancreatic CancerDocument45 pagesPancreatic Cancerapi-1964133750% (2)
- Guide 2015Document78 pagesGuide 2015bovarep216No ratings yet
- Neurologic ExamDocument1 pageNeurologic Examjiglly23100% (2)
- Respiratory ExaminationDocument59 pagesRespiratory ExaminationNur Hamizah Md FuziNo ratings yet
- Pals 2020 Nuevas ConsideracionesDocument1 pagePals 2020 Nuevas Consideracionesfrancia perezNo ratings yet
- OB Part1 - 2022 FatimaDocument119 pagesOB Part1 - 2022 FatimaFemale calmNo ratings yet
- Peripheral Nerve InjuriesDocument810 pagesPeripheral Nerve Injuriessadaf29No ratings yet
- GBSDocument35 pagesGBSJanine CabreraNo ratings yet
- Herings Law of Cure 2011 PDFDocument2 pagesHerings Law of Cure 2011 PDFYannah ReonalNo ratings yet
- Losartan Drug StudyDocument1 pageLosartan Drug Studyiammkrissa88% (17)
- NCPDocument5 pagesNCPRose AnnNo ratings yet
- NCPDocument10 pagesNCPRobin HaliliNo ratings yet
- Pathophysiology, Clinical Manifestation and Diagnosis of PeritonitisDocument6 pagesPathophysiology, Clinical Manifestation and Diagnosis of PeritonitisIOSRjournalNo ratings yet
- SyphilisDocument3 pagesSyphilisstaci_lutchman100% (2)
- Triage Case StudyDocument26 pagesTriage Case Studynadriyaasiin f.gNo ratings yet
- Unit 9 Taking About Symtoms + Unit 13 Family MedicineDocument2 pagesUnit 9 Taking About Symtoms + Unit 13 Family MedicineThuy AnhNo ratings yet
- Global Guidelines For The Prevention of Surgical Site Infection: An IntroductionDocument8 pagesGlobal Guidelines For The Prevention of Surgical Site Infection: An IntroductionJNUHospital NABHNo ratings yet
- What Is A Baker's Cyst ("Popliteal Cyst") ?Document2 pagesWhat Is A Baker's Cyst ("Popliteal Cyst") ?Faris AzharNo ratings yet
- ASCIA Action Plan Allergic Reactions Green 2023Document1 pageASCIA Action Plan Allergic Reactions Green 2023Charles ChinnaiahNo ratings yet
- Poultry Medication: Product Indication Composition Reg No G979 G1305Document1 pagePoultry Medication: Product Indication Composition Reg No G979 G1305irfan syuhada100% (1)