Bronchial Asthma
Bronchial Asthma
Download as pptx, pdf, or txt
You might also like
- AAFP Family Med Board QuestionsDocument96 pagesAAFP Family Med Board QuestionsKamil Hanna100% (2)
- SESAP16 Self AssessmentDocument280 pagesSESAP16 Self AssessmentKamil Hanna100% (2)
- Dr. Lojpur - Dressing and BandageDocument9 pagesDr. Lojpur - Dressing and BandageJayvie Gacutan100% (1)
- Sesap16 Volume 1Document459 pagesSesap16 Volume 1Kamil Hanna33% (3)
- Transfusion ReactionDocument66 pagesTransfusion ReactionAbhineet SalveNo ratings yet
- Transfusion ReactionDocument35 pagesTransfusion ReactionPriya100% (1)
- Central Venous Catheter - StatPearls - NCBI BookshelfDocument11 pagesCentral Venous Catheter - StatPearls - NCBI Bookshelfsafrina100% (1)
- 10 AsthmaDocument39 pages10 AsthmaAkash MishraNo ratings yet
- Cardiac TamponadeDocument10 pagesCardiac TamponadeRahmi Fatma SariNo ratings yet
- Laryngeal Mask LmaDocument25 pagesLaryngeal Mask LmaCiptadi IqbalNo ratings yet
- Bronchiectasis: Dr.K.M.LakshmanarajanDocument238 pagesBronchiectasis: Dr.K.M.LakshmanarajanKM Lakshmana Rajan0% (1)
- 7 Pulmonary EdemaDocument10 pages7 Pulmonary Edemaomar kmr97No ratings yet
- ShockDocument63 pagesShockAhmedNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- Central Venous PressureDocument8 pagesCentral Venous PressureJen GarzoNo ratings yet
- What Is ICU PsychosisDocument6 pagesWhat Is ICU PsychosisAngelicaMarieRafananNo ratings yet
- Case Study (Asthma)Document3 pagesCase Study (Asthma)AIM100% (1)
- Thoracic Injuries 1Document32 pagesThoracic Injuries 1awais mpNo ratings yet
- Postoperative Cognitive Dysfunction Preoperative Risk Assessment and Perioperative Risk Minimization A Pragmatic Review of The LitDocument5 pagesPostoperative Cognitive Dysfunction Preoperative Risk Assessment and Perioperative Risk Minimization A Pragmatic Review of The Litade_liaNo ratings yet
- Anesthesia CHD Non Cardiac SurgeryDocument97 pagesAnesthesia CHD Non Cardiac SurgeryDon DavidNo ratings yet
- Terminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke ManagementDocument28 pagesTerminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke Managementbusiness911No ratings yet
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocument15 pagesPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNo ratings yet
- Oxygen Therapy 1 1Document39 pagesOxygen Therapy 1 1bbeurekaNo ratings yet
- Pneumonectomy S RT RpaDocument4 pagesPneumonectomy S RT RpagireeshsachinNo ratings yet
- Anaesthesia For Cardiac DiseaseDocument26 pagesAnaesthesia For Cardiac DiseasePrabhu KumarNo ratings yet
- Airway Skills 2 - Bag Valve MaskDocument4 pagesAirway Skills 2 - Bag Valve MaskRinna MauLidda100% (1)
- Assignment AnesthesiaDocument9 pagesAssignment AnesthesiaRavi PatelNo ratings yet
- Fecal ImpactionDocument5 pagesFecal Impactioncharie2No ratings yet
- Monitoring in Operation TheatreDocument12 pagesMonitoring in Operation TheatreJunaid ebrahimNo ratings yet
- HSNS264 A1 COPDDocument2 pagesHSNS264 A1 COPDKC Nilam100% (1)
- 13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsDocument10 pages13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsPutri Alin Kende RiaralyNo ratings yet
- Post Resus CareDocument35 pagesPost Resus Caredrjaikrish100% (1)
- Principles of Acute Pain ManagementDocument26 pagesPrinciples of Acute Pain ManagementNasir Jufri100% (1)
- Cardiac Monitor, ECG and CauterizationDocument28 pagesCardiac Monitor, ECG and CauterizationGlaiza Mae Olivar-ArguillesNo ratings yet
- Advanced Trauma Life SupportDocument4 pagesAdvanced Trauma Life SupportMd Ahsanuzzaman PinkuNo ratings yet
- ANAESTHESIA FOR GASTROINTESTINAL CANCER SURGERIES AutosavedDocument40 pagesANAESTHESIA FOR GASTROINTESTINAL CANCER SURGERIES AutosavedKavyasree KatamNo ratings yet
- DR - Sheetal JagatapDocument8 pagesDR - Sheetal JagatapSirisha Ckv100% (1)
- AIRWAY ManagementDocument5 pagesAIRWAY ManagementVijay MgNo ratings yet
- Controlled Hypotensive Anaesthesia What Is Safe ?: DR Hussain Almejadi AL RAZI HospitalDocument50 pagesControlled Hypotensive Anaesthesia What Is Safe ?: DR Hussain Almejadi AL RAZI HospitalcommandityNo ratings yet
- ThoracentesisDocument4 pagesThoracentesisCyntia Theresia Lumintang100% (1)
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDocument2 pagesPericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerlhenNo ratings yet
- Vasodilators: A B C D XDocument1 pageVasodilators: A B C D XPatricia Marie BuenafeNo ratings yet
- Asthma and Status AsthmaticusDocument19 pagesAsthma and Status Asthmaticussharon mogambiNo ratings yet
- Regional AnesthesiaDocument54 pagesRegional AnesthesiaIdza Fariha AfriNo ratings yet
- Mechanical VentilationDocument108 pagesMechanical VentilationKrishnaBihariShuklaNo ratings yet
- Tetralogy of FallotDocument33 pagesTetralogy of FallotjeenaejyNo ratings yet
- A Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionDocument6 pagesA Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionInternational Organization of Scientific Research (IOSR)No ratings yet
- Suctioning TracheaDocument24 pagesSuctioning Trachealuis_chubee100% (1)
- Factors Affectin Block HeightDocument37 pagesFactors Affectin Block HeightshikhaNo ratings yet
- Anaesthesia For Ect March 2020Document120 pagesAnaesthesia For Ect March 2020Sangkaran KumarNo ratings yet
- Sedation in ICUDocument14 pagesSedation in ICUIhtesham Ul Haq100% (1)
- Asthma: A. DefinitionDocument6 pagesAsthma: A. DefinitionElvando SimatupangNo ratings yet
- Preanesthetic Medication JasminaDocument44 pagesPreanesthetic Medication Jasminaanjali sNo ratings yet
- Cardiac TestsDocument17 pagesCardiac TestsGiorgiana pNo ratings yet
- Anaesthesia in Liver Disease PatientDocument49 pagesAnaesthesia in Liver Disease PatientVG FernandezNo ratings yet
- Acute Exacerbation of Asthma Case FileDocument3 pagesAcute Exacerbation of Asthma Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Pleural Fluid AnalysisDocument15 pagesPleural Fluid AnalysisNatalie Sarah MoonNo ratings yet
- Caudal BlockDocument6 pagesCaudal BlockAshish PandeyNo ratings yet
- Management of Emergencies in ChildrenDocument39 pagesManagement of Emergencies in ChildrensastroboyzNo ratings yet
- BASIC LIFE SUPPORT Basics IntroductionDocument27 pagesBASIC LIFE SUPPORT Basics IntroductionMUKESH SUNDARARAJANNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The Anatomical Foundations of Regional Anesthesia and Acute Pain MedicineFrom EverandThe Anatomical Foundations of Regional Anesthesia and Acute Pain MedicineNo ratings yet
- PIIS2468428721000071Document30 pagesPIIS2468428721000071Kamil HannaNo ratings yet
- Fluid and Electrolyte General Surgery Review Course.Document97 pagesFluid and Electrolyte General Surgery Review Course.Kamil HannaNo ratings yet
- Answer: C: Refer To The Information Provided in Figure 7.2 Below To Answer The Following QuestionsDocument5 pagesAnswer: C: Refer To The Information Provided in Figure 7.2 Below To Answer The Following QuestionsKamil HannaNo ratings yet
- Principles of Macroeconomics, 9e - TB1 (Case/Fair/Oster)Document987 pagesPrinciples of Macroeconomics, 9e - TB1 (Case/Fair/Oster)Kamil HannaNo ratings yet
- Candida VulvovaginitisDocument20 pagesCandida VulvovaginitisVicobeingo100% (1)
- BilirubinDocument6 pagesBilirubinwandebesNo ratings yet
- Care of Mother, Child, and Adolescent (Well-Client) Related Learning Experience, Skills LaboratoryDocument7 pagesCare of Mother, Child, and Adolescent (Well-Client) Related Learning Experience, Skills LaboratoryJohn Lawrence YbanezNo ratings yet
- 1.1 BackgroundDocument14 pages1.1 BackgroundDwi WulandariNo ratings yet
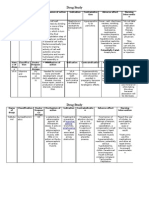
- Drug StudyDocument3 pagesDrug StudyfortunelobsterNo ratings yet
- Artigo 26-04-2019 Obstrução Intestinal Maligna 2019 PDFDocument4 pagesArtigo 26-04-2019 Obstrução Intestinal Maligna 2019 PDFFernanda CorreiaNo ratings yet
- Head NeckDocument8 pagesHead NeckerandolphsavageNo ratings yet
- HYPOSKILIADocument2 pagesHYPOSKILIAMohammad Abid100% (1)
- BabinaDocument39 pagesBabinaSanjeet DuhanNo ratings yet
- SOT SummaryDocument1 pageSOT SummaryRukaphuongNo ratings yet
- Chemical Mediators of Acute Inflammation 2Document41 pagesChemical Mediators of Acute Inflammation 2Sashika Tharindu100% (1)
- Cardiac Medical Center2222Document26 pagesCardiac Medical Center2222Yumna M. EissaNo ratings yet
- Log Book (Eng)Document10 pagesLog Book (Eng)revanth kallaNo ratings yet
- Pet CT ScanDocument37 pagesPet CT ScanCut Hanassa Muly80% (5)
- Biomarkers of Infection and SepsisDocument12 pagesBiomarkers of Infection and SepsisnuelitopNo ratings yet
- (Human Anatomy and Physiology) Jane E. Middleton-Wound Healing - Process, Phases, and Promoting-Nova Science Publishers (2011)Document226 pages(Human Anatomy and Physiology) Jane E. Middleton-Wound Healing - Process, Phases, and Promoting-Nova Science Publishers (2011)Muhammad IrwaniNo ratings yet
- Dr. Michael Golding: California Prison Report On Mental HealthcareDocument161 pagesDr. Michael Golding: California Prison Report On Mental HealthcareLeigh EganNo ratings yet
- Dermatology MCQ With AnswersDocument27 pagesDermatology MCQ With Answershesham0% (1)
- Assessing Six Decades of Rabies in The PhilippinesDocument10 pagesAssessing Six Decades of Rabies in The PhilippinesIJPHSNo ratings yet
- Anatomy and Physiology of Female Reproductive SystemDocument67 pagesAnatomy and Physiology of Female Reproductive Systemannu panchalNo ratings yet
- Cardiopulmonary ResuscitationDocument10 pagesCardiopulmonary ResuscitationZacchariah Zeref CaraigNo ratings yet
- ENLS Acute Ischemic Stroke ProtokolDocument23 pagesENLS Acute Ischemic Stroke ProtokolFransiskus MikaelNo ratings yet
- 1st Quarter Summative Test MapehDocument2 pages1st Quarter Summative Test MapehThel Padiz DistritoNo ratings yet
- Esophagus HUDocument84 pagesEsophagus HURaneen SamraNo ratings yet
- ER 1x20 - Full Moon Saturday NightDocument74 pagesER 1x20 - Full Moon Saturday NightprinceandladyshadeNo ratings yet
- MIMSDocument3 pagesMIMSFrancineAntoinetteGonzalesNo ratings yet
- AmyloidosisDocument15 pagesAmyloidosisNicoletta OrphanouNo ratings yet
- Literature Review On Oxygen TherapyDocument6 pagesLiterature Review On Oxygen Therapyjzneaqwgf100% (1)
- How To Intervene in The Caries Process in Older Adults (CariesRes 2020)Document7 pagesHow To Intervene in The Caries Process in Older Adults (CariesRes 2020)drjiachenwanNo ratings yet
- Non-Hodgkin's Malignant Lymphomas of The Palatine Tonsils: A Case ReportDocument4 pagesNon-Hodgkin's Malignant Lymphomas of The Palatine Tonsils: A Case ReportWorld Journal of Case Reports and Clinical Images (ISSN: 2835-1568) CODEN:USANo ratings yet