10 Asthma
10 Asthma
Download as pptx, pdf, or txt
You might also like
- Voice Change - SSC Board QuestionsDocument3 pagesVoice Change - SSC Board QuestionsGazi Hayder Sami100% (8)
- Respiratory Infections 1Document62 pagesRespiratory Infections 1Eduardo Valdez RodríguezNo ratings yet
- Upper Airway InfectionsDocument5 pagesUpper Airway InfectionsPhilline MacapagalNo ratings yet
- Michael Jai White PDFDocument7 pagesMichael Jai White PDFFrank Ramírez ParedesNo ratings yet
- Achilles Repair ProtocolDocument19 pagesAchilles Repair ProtocolRobertNo ratings yet
- Bronchial AsthmaDocument54 pagesBronchial AsthmaSehar162100% (2)
- Bronchial AsthmaDocument25 pagesBronchial AsthmaKamil HannaNo ratings yet
- Metab II DiverticulosisDocument94 pagesMetab II DiverticulosisEthel Lourdes Cornejo AmodiaNo ratings yet
- Nclex Review Pneumonia COPD AsDocument11 pagesNclex Review Pneumonia COPD Asmj078No ratings yet
- Asthma and Status AsthmaticusDocument19 pagesAsthma and Status Asthmaticussharon mogambiNo ratings yet
- Respiratory FailureDocument22 pagesRespiratory FailurereynoldNo ratings yet
- Corrected Bronchial Asthma PPDocument20 pagesCorrected Bronchial Asthma PPKetheesaran LingamNo ratings yet
- Acute Exacerbation of Asthma Case FileDocument3 pagesAcute Exacerbation of Asthma Case Filehttps://medical-phd.blogspot.comNo ratings yet
- LaryngitisDocument40 pagesLaryngitisMikhail Guidicelli100% (1)
- Acute Respiratory InfectionsDocument18 pagesAcute Respiratory InfectionsEmilyRose17No ratings yet
- Thoracic Injuries 1Document32 pagesThoracic Injuries 1awais mpNo ratings yet
- TuberculosisDocument28 pagesTuberculosisBir Mohammad SonetNo ratings yet
- EmphysemaDocument3 pagesEmphysemaKhalid Mahmud ArifinNo ratings yet
- Part I: IntroductionDocument4 pagesPart I: IntroductionChezka PalolaNo ratings yet
- Systemic Inflammatory ResponseDocument2 pagesSystemic Inflammatory Responsesmithaanne20016923No ratings yet
- Chest Pain.Document53 pagesChest Pain.Shimmering MoonNo ratings yet
- CardiomegalyDocument31 pagesCardiomegalyDeepika LingamNo ratings yet
- Pulmonary TuberculosisDocument6 pagesPulmonary TuberculosisZachary CohenNo ratings yet
- Hiv/Aids: by Aisha MansurDocument34 pagesHiv/Aids: by Aisha MansurMpanso Ahmad AlhijjNo ratings yet
- Oncology Nursing Lecture Week 1-6Document171 pagesOncology Nursing Lecture Week 1-6acentino121No ratings yet
- PneumoniasDocument58 pagesPneumoniasKai Edmond MarvellaNo ratings yet
- GfsgsDocument34 pagesGfsgsHeather PorterNo ratings yet
- Pulmonary EmbolismDocument6 pagesPulmonary EmbolismKristina Ana ClaudioNo ratings yet
- Transfusion ReactionDocument35 pagesTransfusion ReactionPriya100% (1)
- Chronic BronchitisDocument5 pagesChronic BronchitisJemalyn M. Saludar100% (2)
- PneumoniaDocument19 pagesPneumoniaMichael UrrutiaNo ratings yet
- Diarrhea: Persistent If 2-4 Weeks, and Chronic If 4 Weeks in DurationDocument12 pagesDiarrhea: Persistent If 2-4 Weeks, and Chronic If 4 Weeks in DurationAnonymous IWRTYznDZnNo ratings yet
- Bronchiectasis - Ppt-Medina Presentation2Document25 pagesBronchiectasis - Ppt-Medina Presentation2chebetnaomi945No ratings yet
- Woman With PneumoniaDocument9 pagesWoman With PneumoniaNohaira SADANGNo ratings yet
- Septic ShockDocument16 pagesSeptic ShockGelo JvrNo ratings yet
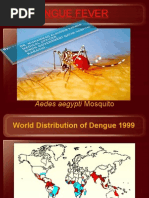
- Dengue FeverDocument39 pagesDengue FeverMuhammad Alauddin Sarwar100% (15)
- Case Study (Asthma)Document3 pagesCase Study (Asthma)AIM100% (1)
- CopdDocument14 pagesCopdMohd Farid Bin RosliNo ratings yet
- 13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsDocument10 pages13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsPutri Alin Kende RiaralyNo ratings yet
- Myasthenia GravisDocument3 pagesMyasthenia Gravisdmnd_cdNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS)Document72 pagesAcute Respiratory Distress Syndrome (ARDS)desyNo ratings yet
- Mini-Case Presentation: Mild Head InjuryDocument16 pagesMini-Case Presentation: Mild Head InjuryMarianne OblefiasNo ratings yet
- Covid 19 - PathophysiologyDocument3 pagesCovid 19 - PathophysiologyRenea Joy ArruejoNo ratings yet
- Management of Septic Shock in An Intermediate Care UnitDocument20 pagesManagement of Septic Shock in An Intermediate Care UnitJHNo ratings yet
- Pneumonia: DefinitionDocument5 pagesPneumonia: DefinitionhemaanandhyNo ratings yet
- N24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis AsthmaDocument42 pagesN24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis Asthmadentist40No ratings yet
- CopdDocument18 pagesCopdHidy SatorreNo ratings yet
- Early and Late Signs of Increased Intracranial PressureDocument8 pagesEarly and Late Signs of Increased Intracranial PressureRhae Raynog100% (2)
- Maplesons Breathing SystemsDocument9 pagesMaplesons Breathing SystemsMohmmed MousaNo ratings yet
- Transfusion ReactionDocument66 pagesTransfusion ReactionAbhineet SalveNo ratings yet
- CardiomyopathyDocument2 pagesCardiomyopathyBianca SarmientoNo ratings yet
- Pulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorDocument16 pagesPulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorKaku ManishaNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- New Human Influenza A (H1N1) : Anthony Z. San Juan, MD PHSAE Resu, CHD-MMDocument57 pagesNew Human Influenza A (H1N1) : Anthony Z. San Juan, MD PHSAE Resu, CHD-MMmlbonthelineNo ratings yet
- An Approach To Coma.Document32 pagesAn Approach To Coma.Divya GNo ratings yet
- Respiratory Emx ARF ARDSDocument12 pagesRespiratory Emx ARF ARDSRENEROSE TORRESNo ratings yet
- PneumothoraxDocument45 pagesPneumothoraxWiDya EmiLiaNo ratings yet
- ShockDocument21 pagesShockNyakie MotlalaneNo ratings yet
- Hematemesis PDFDocument7 pagesHematemesis PDFkevin_jawanNo ratings yet
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- High Altitude Sickness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHigh Altitude Sickness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ludwig’s Angina, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLudwig’s Angina, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Push Pull Legs Program by Mantas EitmonDocument5 pagesPush Pull Legs Program by Mantas EitmonLeafasNo ratings yet
- Clean and Safe Hospitals Benchmark of Alert Comprensive SpecializedDocument69 pagesClean and Safe Hospitals Benchmark of Alert Comprensive SpecializednibretzwNo ratings yet
- Study of Illness ConditionDocument6 pagesStudy of Illness Conditionyong_gret100% (2)
- The Labour Party and The Welfare State in BritainDocument25 pagesThe Labour Party and The Welfare State in BritainBilal B'oNo ratings yet
- 2018 05 01 Shape SingaporeDocument108 pages2018 05 01 Shape SingaporeMitch YeohNo ratings yet
- Clean India Green IndiaDocument2 pagesClean India Green IndiaMaroofa BhatNo ratings yet
- Risk Assessment Procedures - Step To Prepare Risk AssessmentDocument5 pagesRisk Assessment Procedures - Step To Prepare Risk AssessmentaneethavilsNo ratings yet
- Prohibition and Regulation of Sales Under Food Adulteration ActDocument13 pagesProhibition and Regulation of Sales Under Food Adulteration ActFlab ThugsNo ratings yet
- Plo 5Document3 pagesPlo 5api-541819532No ratings yet
- Stopping World Hungry EssayDocument6 pagesStopping World Hungry Essayapi-318032750100% (1)
- 建筑环境对治疗人们心理健康的 影响 - 文献综述 Effects of built environment on healing the mental health of the people -literature reviewDocument9 pages建筑环境对治疗人们心理健康的 影响 - 文献综述 Effects of built environment on healing the mental health of the people -literature reviewWENJIE LINo ratings yet
- General Science Practice Test: 1. Glass Is Made of The Mixture ofDocument49 pagesGeneral Science Practice Test: 1. Glass Is Made of The Mixture ofJerel John CalanaoNo ratings yet
- Case Study 4-Middle County HospitalDocument5 pagesCase Study 4-Middle County HospitalsushmaNo ratings yet
- Teaching PlanDocument1 pageTeaching PlanJamaica AngotNo ratings yet
- Amazing Wellness - Early Winter USA PDFDocument100 pagesAmazing Wellness - Early Winter USA PDFHimanshu KhuranaNo ratings yet
- Heller Bergman 1953Document11 pagesHeller Bergman 1953Sirine AjourNo ratings yet
- Family First Life Lawsuit Do Not Call Lawsuit For $694,000Document91 pagesFamily First Life Lawsuit Do Not Call Lawsuit For $694,000gusNo ratings yet
- Homicidal HangingDocument3 pagesHomicidal HangingChayru nisaNo ratings yet
- DBL 8585 - E - 2010-09 EnglishDocument47 pagesDBL 8585 - E - 2010-09 EnglishPaul RedaiNo ratings yet
- BELOW KNEE AMPUTATION EditDocument16 pagesBELOW KNEE AMPUTATION EditPutri AyuNo ratings yet
- VertigoDocument19 pagesVertigonetifarhatiiNo ratings yet
- Cavity Search Produces 50 Bags of Heroin in Northeastern Pennsylvania COMMENTS ARE The BESTDocument6 pagesCavity Search Produces 50 Bags of Heroin in Northeastern Pennsylvania COMMENTS ARE The BESTKAWNo ratings yet
- HM 340 Rotary Microtome 387831Document60 pagesHM 340 Rotary Microtome 387831Oscar MarencoNo ratings yet
- Preventive OphthalmologyDocument41 pagesPreventive Ophthalmologymalaymallik210No ratings yet
- Name: Sad-Ang, John Daryl P. Course, Year & Section: Bsn-2BDocument2 pagesName: Sad-Ang, John Daryl P. Course, Year & Section: Bsn-2BJohn Daryl Sad-angNo ratings yet
- SOP High Pressure Water Jet CleaningDocument3 pagesSOP High Pressure Water Jet Cleaningtengku hafizNo ratings yet
- Treatment of Tannery WastewaterDocument11 pagesTreatment of Tannery Wastewatersadakeling90% (1)