Title Layout: Subtitle
Title Layout: Subtitle
Download as pptx, pdf, or txt
You might also like
- Psychopharmacology PDFDocument563 pagesPsychopharmacology PDFmichaeldalessio100% (8)
- LISC 391 Scientific Poster Assignment - Group 6Document1 pageLISC 391 Scientific Poster Assignment - Group 6Alecco PhilippiNo ratings yet
- Poisoning and Drug OverdoseDocument95 pagesPoisoning and Drug OverdoseMohammed Younis Shaheen100% (2)
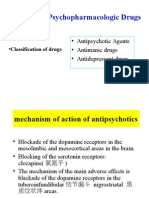
- Psychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDocument18 pagesPsychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDrima EdiNo ratings yet
- PoisoningDocument35 pagesPoisoningMUKESH SUNDARARAJANNo ratings yet
- PoisoningDocument103 pagesPoisoningC Hendra Wijaya100% (2)
- Organophosphate PoisoningDocument22 pagesOrganophosphate Poisoningatiyasimon2020No ratings yet
- Poison InformationDocument27 pagesPoison InformationJanvi PatelNo ratings yet
- Cyanide Poisoning - UpToDateDocument23 pagesCyanide Poisoning - UpToDateAnonymous 9dVZCnTXS100% (2)
- Inhaled PoisonsDocument4 pagesInhaled PoisonsKev ManaogNo ratings yet
- Poisoning and ManagementDocument53 pagesPoisoning and ManagementYusuf Nawaz KhanNo ratings yet
- WHO Management of PoisoningDocument159 pagesWHO Management of PoisoningMarian Joyce Princess YuqueNo ratings yet
- Mod 7 PoisoningDocument20 pagesMod 7 PoisoningKian Alfrz100% (2)
- Drugs in AnesthesiaDocument43 pagesDrugs in AnesthesiaMahyal HabibiNo ratings yet
- ER ToxicologyDocument17 pagesER ToxicologyasclswisconsinNo ratings yet
- Hydrocarbon PoisoningDocument10 pagesHydrocarbon PoisoningVarshith GandlaNo ratings yet
- Poisoning First AidDocument13 pagesPoisoning First AidGerra Mae Tubio Candelasa100% (1)
- Organophosphates and Carbamates PoisoningDocument34 pagesOrganophosphates and Carbamates PoisoningMuhammad Hammad Maahi100% (1)
- Alcoholism & Drug DependanceDocument36 pagesAlcoholism & Drug DependanceRahul NetragaonkarNo ratings yet
- Guideline Antibiotic RationalDocument35 pagesGuideline Antibiotic RationalIstianah EsNo ratings yet
- Organophosphate PoisoningDocument31 pagesOrganophosphate Poisoningjosecarlo_masangkay100% (1)
- Anti Tubercular DrugsDocument63 pagesAnti Tubercular DrugsYasir KhanNo ratings yet
- Paracetamol Overdose Treatment NomogramDocument1 pageParacetamol Overdose Treatment NomogramCoenraad van SchoorNo ratings yet
- Dermatologic PharmacologyDocument31 pagesDermatologic PharmacologyFor ChristNo ratings yet
- Routes of AdministrationDocument32 pagesRoutes of AdministrationEsha pant100% (1)
- Poisoning DecontaminationDocument14 pagesPoisoning DecontaminationadystiNo ratings yet
- Factors Affecting Drug AbsorptionDocument11 pagesFactors Affecting Drug AbsorptionClarilaine JavierNo ratings yet
- Opioid Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineDocument16 pagesOpioid Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineM KNo ratings yet
- PoisoningDocument39 pagesPoisoningNatnael ShifferawNo ratings yet
- 3 Intravenous-TherapyDocument4 pages3 Intravenous-TherapyMarie Louise Nicole TuvillaNo ratings yet
- Extra Corporeal Removal of DrugsDocument25 pagesExtra Corporeal Removal of Drugsyuppie_raj2175No ratings yet
- HI Classmates!!!Document36 pagesHI Classmates!!!Alex SilvanoNo ratings yet
- Microbial Diseases of The Respiratory SystemDocument6 pagesMicrobial Diseases of The Respiratory SystemJohn Daemer Halasan KinocNo ratings yet
- Overdose and PoisoningDocument4 pagesOverdose and PoisoningMahmoud SelimNo ratings yet
- Head Injury: Tsegazeab Laeke, MD, FCS (ECSA) August 1,2018Document38 pagesHead Injury: Tsegazeab Laeke, MD, FCS (ECSA) August 1,2018Amanuel AyladoNo ratings yet
- Module # 5 Pharmacology NursingDocument45 pagesModule # 5 Pharmacology Nursingannyeong_123No ratings yet
- Cardiac Toxic ResponsesDocument10 pagesCardiac Toxic ResponsesDaismar ArenasNo ratings yet
- Accidental PoisoningDocument3 pagesAccidental PoisoningBRUELIN MELSHIA MNo ratings yet
- Knowledge, Attitude and Practice of Self-Medication Among Medical StudentsDocument8 pagesKnowledge, Attitude and Practice of Self-Medication Among Medical StudentsInternational Organization of Scientific Research (IOSR)No ratings yet
- Allergic Rhinitis PDFDocument3 pagesAllergic Rhinitis PDFdrbilalmunirNo ratings yet
- COPDDocument59 pagesCOPDKarenmedicalNo ratings yet
- Anti Hypertensive DrugsDocument40 pagesAnti Hypertensive DrugsjawadNo ratings yet
- 9) Medical Complications of Drug TakingDocument44 pages9) Medical Complications of Drug TakingDr. Zirwa AsimNo ratings yet
- Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis Management, Prognosis and Long Term SequelaeDocument28 pagesStevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis Management, Prognosis and Long Term SequelaePutri SRNo ratings yet
- General Management of Poisoned PatientsDocument38 pagesGeneral Management of Poisoned PatientsDokhter DavidsonNo ratings yet
- Sedative-Hypnotics (SeH) and AnxiolyticsDocument101 pagesSedative-Hypnotics (SeH) and Anxiolyticsmatchees-gone rogueNo ratings yet
- Approach To Poisoned PatientDocument90 pagesApproach To Poisoned PatientGopi KrishnanNo ratings yet
- SympathomimeticDocument56 pagesSympathomimeticvarish0% (1)
- Blood PressureDocument6 pagesBlood PressuremohitNo ratings yet
- Community Pharmacy ManagementDocument29 pagesCommunity Pharmacy ManagementAnushka Mani tripathiNo ratings yet
- Neurological Disorders: Prof. Bernardo Fernandez IIDocument33 pagesNeurological Disorders: Prof. Bernardo Fernandez IIBernardNo ratings yet
- Drug ExcretionDocument20 pagesDrug ExcretionRajalingam BalaNo ratings yet
- Approach To Aggressive PatientsDocument25 pagesApproach To Aggressive PatientsdocshahirNo ratings yet
- Guaphan Syrup Patient Information LeafletDocument1 pageGuaphan Syrup Patient Information LeafletAhmad BakerNo ratings yet
- ToxicologyDocument31 pagesToxicologyHeart Hacker HarryNo ratings yet
- III) Pharmacotherapy of Angina PectorisDocument23 pagesIII) Pharmacotherapy of Angina PectorisAyro Business CenterNo ratings yet
- Different Types of Glass Containers Used in Pharmaceuticals - Pharmaceutical Guidelines PDFDocument2 pagesDifferent Types of Glass Containers Used in Pharmaceuticals - Pharmaceutical Guidelines PDFRama KumarNo ratings yet
- Intravenous Anesthetic AgentsDocument60 pagesIntravenous Anesthetic AgentsAnonymous Ia9LPzNo ratings yet
- 10 AsthmaDocument39 pages10 AsthmaAkash MishraNo ratings yet
- Cardiovascular System: Antihypertensive DrugsDocument73 pagesCardiovascular System: Antihypertensive Drugsأمجد محمدNo ratings yet
- Hematinic AgentsDocument89 pagesHematinic AgentsHussain Rizvi50% (2)
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- SNS and PNS Drugs (Cholinergics and Adrenergics)Document5 pagesSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- ANS PharmacologyDocument18 pagesANS Pharmacologysunit kashyapNo ratings yet
- Cholinoceptors Activating Drugs.Document48 pagesCholinoceptors Activating Drugs.Kate EvangelistaNo ratings yet
- Neurotransmitters and ReceptorsDocument8 pagesNeurotransmitters and ReceptorsmahambaqaiNo ratings yet
- Lecture 15 Cholinergic TransmissionDocument20 pagesLecture 15 Cholinergic TransmissionSamer FarhanNo ratings yet
- Biochemistry Fall 2020 Midterm Exam SolutionsDocument44 pagesBiochemistry Fall 2020 Midterm Exam SolutionsEren KayaNo ratings yet
- Medicinal Chemistry/ CHEM 458/658 Chapter 8-Receptors and MessengersDocument41 pagesMedicinal Chemistry/ CHEM 458/658 Chapter 8-Receptors and MessengersMehak SarfrazNo ratings yet
- Compendium On Pesticide Use in VegetablesDocument147 pagesCompendium On Pesticide Use in VegetablesSan ThoshNo ratings yet
- NP StructureDocument4 pagesNP Structureelsayedola13No ratings yet
- Program and Proceedings - 7th International Regional "Stress and Behavior" Neuroscience and Biopsychiatry Conference (North America), June 22-24, 2016, Miami Beach, FL, USADocument33 pagesProgram and Proceedings - 7th International Regional "Stress and Behavior" Neuroscience and Biopsychiatry Conference (North America), June 22-24, 2016, Miami Beach, FL, USAISBS_SocietyNo ratings yet
- Medicinal Chemistry and Molecular Pharmacology of GABA-C ReceptorsDocument12 pagesMedicinal Chemistry and Molecular Pharmacology of GABA-C ReceptorsHuallpa Samaniego SebastianNo ratings yet
- Huperzia Serrata..........Document60 pagesHuperzia Serrata..........BíchNguyễnNo ratings yet
- Receptors Ionchannel TransporterDocument58 pagesReceptors Ionchannel TransporterDeepu Vijay100% (1)
- PharmacologyDocument93 pagesPharmacologyPh SamerNo ratings yet
- A Review On Anthelmintic Drugs and Their Future ScopeDocument6 pagesA Review On Anthelmintic Drugs and Their Future ScopeIqra IqraNo ratings yet
- Update Pharma Graf GDocument3 pagesUpdate Pharma Graf GSyamil Azhar100% (1)
- T-Type Calcium Channel Blockers: A Patent Review (2012-2018)Document20 pagesT-Type Calcium Channel Blockers: A Patent Review (2012-2018)Zilmaida SalomNo ratings yet
- Patrick: An Introduction To Medicinal Chemistry 5e: Cholinergics & AnticholinesterasesDocument95 pagesPatrick: An Introduction To Medicinal Chemistry 5e: Cholinergics & Anticholinesterasessan50% (2)
- Drug Receptor TheoryDocument9 pagesDrug Receptor TheoryFish YanNo ratings yet
- 1 Cholinergic & Noradrenergic Transmission IDocument37 pages1 Cholinergic & Noradrenergic Transmission IGeraldine Ong100% (2)
- Alu-Mediated Phylogenetic Novelties in Gene Regulation and DevelopmentDocument9 pagesAlu-Mediated Phylogenetic Novelties in Gene Regulation and DevelopmentArtyumR IINo ratings yet
- M3 Lesson 3 Check-In Activity - MAMOLO DENT 3F PDFDocument2 pagesM3 Lesson 3 Check-In Activity - MAMOLO DENT 3F PDFZHAREIGHNEILE C. MAMOLONo ratings yet
- 05 - 06 - 07.curs Farmacologie Speciala (SNV)Document108 pages05 - 06 - 07.curs Farmacologie Speciala (SNV)madalinaNo ratings yet
- Chemicals' List and Mixing Protocol V9 - 06.05.2023Document11 pagesChemicals' List and Mixing Protocol V9 - 06.05.2023Waqas AnjumNo ratings yet
- Cholinergic DrugsDocument22 pagesCholinergic Drugsmug ashNo ratings yet
- Toxicologic Emergencies, 11th Goldfrank's 2019Document10 pagesToxicologic Emergencies, 11th Goldfrank's 2019RenéNo ratings yet
- Cholinergic Agonist and AntagonistDocument4 pagesCholinergic Agonist and Antagoniststephanienwafor18No ratings yet
- Full Download Signal Transduction, Third Edition Kramer PDFDocument64 pagesFull Download Signal Transduction, Third Edition Kramer PDFpujaandjebar100% (2)