Surgery Department: Emergency Case Reports
Surgery Department: Emergency Case Reports
Download as pptx, pdf, or txt
You might also like
- KV Krishna Das Medicine 5th EditionDocument1,490 pagesKV Krishna Das Medicine 5th EditionPratik100% (10)
- Physical Examination of Spine (TN)Document55 pagesPhysical Examination of Spine (TN)Francesc OktofabregasNo ratings yet
- Lalpathlab PDFDocument3 pagesLalpathlab PDFTushar Kar0% (1)
- DR Suparman Edit IP 5-2-14Document58 pagesDR Suparman Edit IP 5-2-14Mohamad ZulfikarNo ratings yet
- Emergency Case Dr. SyarifDocument38 pagesEmergency Case Dr. SyarifsitisrisuryaniNo ratings yet
- Emcase 04 Feb 2019 Dr. KometDocument56 pagesEmcase 04 Feb 2019 Dr. KometKomet Rama DaudNo ratings yet
- Surgery Department: Emergency Case ReportsDocument47 pagesSurgery Department: Emergency Case ReportsMohamad ZulfikarNo ratings yet
- Surgery Department: Emergency Case ReportsDocument17 pagesSurgery Department: Emergency Case ReportsMohamad ZulfikarNo ratings yet
- Emcase 1 Juli EnglishDocument38 pagesEmcase 1 Juli EnglishAndi Nurjannah KaddirajaNo ratings yet
- Ambulation: Patient Hospitalized: 4 Patients Observation: 1 Patient Operated: 3 Patient Death: PatientDocument64 pagesAmbulation: Patient Hospitalized: 4 Patients Observation: 1 Patient Operated: 3 Patient Death: PatientMohamad ZulfikarNo ratings yet
- Slide Emcae DR Suleman, 12-2-2014Document58 pagesSlide Emcae DR Suleman, 12-2-2014Mohamad ZulfikarNo ratings yet
- Surgery Department: Emergency Case ReportsDocument27 pagesSurgery Department: Emergency Case ReportsMukhizalNo ratings yet
- Case Report 31-01-2019Document38 pagesCase Report 31-01-2019Anastanio AnugrahNo ratings yet
- Emcase DR Asdar 9 Juli 2015Document24 pagesEmcase DR Asdar 9 Juli 2015MukhizalNo ratings yet
- Surgery Department: Emergency Case ReportsDocument19 pagesSurgery Department: Emergency Case ReportsMohamad ZulfikarNo ratings yet
- Surgery Department: Emergency Case ReportsDocument20 pagesSurgery Department: Emergency Case ReportsMohamad ZulfikarNo ratings yet
- Case Presentation RADocument6 pagesCase Presentation RAdocv526No ratings yet
- Fracture MandibulaDocument13 pagesFracture MandibulaMohamad ZulfikarNo ratings yet
- Abdominal Trauma TreatmentDocument43 pagesAbdominal Trauma TreatmentChester Bennington Crawling in our skinNo ratings yet
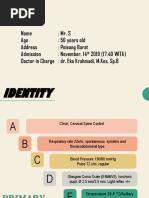
- Main Complaint: ConditionDocument12 pagesMain Complaint: ConditionMyra MieraNo ratings yet
- IA 070519 Lap - Jag. BayanganDocument55 pagesIA 070519 Lap - Jag. BayanganridhoprasetNo ratings yet
- Surgery Department: Emergency Case ReportsDocument46 pagesSurgery Department: Emergency Case ReportsMohamad ZulfikarNo ratings yet
- Surgery Department: Emergency Case ReportsDocument43 pagesSurgery Department: Emergency Case ReportsMukhizalNo ratings yet
- Luka Tusuk BusurDocument5 pagesLuka Tusuk BusurMohamad ZulfikarNo ratings yet
- Depressed FractureDocument13 pagesDepressed FractureMohamad ZulfikarNo ratings yet
- DR Agus Emcase 17-2-14 EditDocument46 pagesDR Agus Emcase 17-2-14 EditMohamad ZulfikarNo ratings yet
- Surgery Department: Emergency Case Reports Sunday, August 12 2018Document36 pagesSurgery Department: Emergency Case Reports Sunday, August 12 2018MukhizalNo ratings yet
- 14-11-2019, Mr. Sandi-57 Yo, Open Fraktur Metatarsal Digiti I, 2,3 Pedis Dekstra, Dr. Eko Krahmadi, M.Kes., SP.BDocument13 pages14-11-2019, Mr. Sandi-57 Yo, Open Fraktur Metatarsal Digiti I, 2,3 Pedis Dekstra, Dr. Eko Krahmadi, M.Kes., SP.BRa' DesireeNo ratings yet
- Peritonitis Generalisata Post Laparoskopi AppendiktomiDocument15 pagesPeritonitis Generalisata Post Laparoskopi AppendiktomiguterizalNo ratings yet
- Death Case Dr. MeikoDocument49 pagesDeath Case Dr. MeikoMohamad ZulfikarNo ratings yet
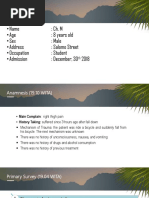
- Name: Ch. M - Age: 8 Years Old - Sex: Male - Address: Salomo Street - Occupation: Student - Admission: December, 30 2018Document13 pagesName: Ch. M - Age: 8 Years Old - Sex: Male - Address: Salomo Street - Occupation: Student - Admission: December, 30 2018Ishmah 'Killua' ChanNo ratings yet
- Night Report 1 MarchDocument34 pagesNight Report 1 MarchRatu Qurroh AinNo ratings yet
- 09-09-2019 - Ch. Faizal - 15YO - Vulnus Laceratum Regio Dorsum Pedis Sinistra - DR - Tri Tuti, Sp. OTDocument14 pages09-09-2019 - Ch. Faizal - 15YO - Vulnus Laceratum Regio Dorsum Pedis Sinistra - DR - Tri Tuti, Sp. OTAtfalNo ratings yet
- Emergency Case Reports: Surgery DepartmentDocument37 pagesEmergency Case Reports: Surgery DepartmentamrulNo ratings yet
- DR MA16072019 Edit SoreDocument27 pagesDR MA16072019 Edit SoreridhoprasetNo ratings yet
- Surgery Department: Morning ReportsDocument17 pagesSurgery Department: Morning ReportsguterizalNo ratings yet
- Emergency Case Reports: Surgery DepartmentDocument27 pagesEmergency Case Reports: Surgery DepartmentMukhizalNo ratings yet
- MR - Shock Septic + Kolangitis + Ikterus Obstruktif + Trombositopenia + Hypercoagulable State + AKI+ Hiperkalemia 8 Desember 2021Document41 pagesMR - Shock Septic + Kolangitis + Ikterus Obstruktif + Trombositopenia + Hypercoagulable State + AKI+ Hiperkalemia 8 Desember 2021yoeldpNo ratings yet
- Surgery Department: Emergency Case ReportsDocument31 pagesSurgery Department: Emergency Case ReportsmasyfuqNo ratings yet
- Penetrating Injury: TJ Kevin DoctorDocument105 pagesPenetrating Injury: TJ Kevin DoctorTj Kevin P-DoctorNo ratings yet
- Emergency Case Reports: Surgery DepartmentDocument19 pagesEmergency Case Reports: Surgery DepartmentdeoNo ratings yet
- Laporan Kasus: Gout ArthritisDocument55 pagesLaporan Kasus: Gout ArthritisikaNo ratings yet
- Syok Hipovolemik PerbaikanDocument24 pagesSyok Hipovolemik Perbaikanyoelpurnama1991No ratings yet
- Vulnus Ictum: Dr. Jeremia SamosirDocument64 pagesVulnus Ictum: Dr. Jeremia SamosirjerryNo ratings yet
- Morning Report: DM Irene DM CenDocument10 pagesMorning Report: DM Irene DM CenYunriNo ratings yet
- CasePres Dr. EpiliDocument5 pagesCasePres Dr. EpiliPeter PanNo ratings yet
- Perforasi GasterDocument22 pagesPerforasi Gasterlukas mansnandifuNo ratings yet
- Morning Report-Ucha Anggiani Putri-1908437660Document45 pagesMorning Report-Ucha Anggiani Putri-1908437660Muhamad AlfariziNo ratings yet
- Surgery Department: Emergency Case ReportsDocument22 pagesSurgery Department: Emergency Case ReportsMohamad ZulfikarNo ratings yet
- Surgery Department: Emergency Case ReportsDocument34 pagesSurgery Department: Emergency Case ReportsMohamad ZulfikarNo ratings yet
- Death Case DR Agus 9-2-2014 EditDocument18 pagesDeath Case DR Agus 9-2-2014 EditMohamad ZulfikarNo ratings yet
- Renal Cell Carcinoma Tuberous SclerosisDocument48 pagesRenal Cell Carcinoma Tuberous SclerosisPiyushNo ratings yet
- LapjagDocument19 pagesLapjagVinnie Juliana YonatanNo ratings yet
- Ca - CacaoDocument2 pagesCa - CacaoISRAEL JULIANO SALGADONo ratings yet
- STEMI AnteroseptalDocument14 pagesSTEMI AnteroseptalJalalludin AnNo ratings yet
- ED Case Discussion - TraumaDocument23 pagesED Case Discussion - TraumaMimi Suhaini SudinNo ratings yet
- Surgery Department: Emergency Case ReportsDocument16 pagesSurgery Department: Emergency Case ReportschiciNo ratings yet
- Chief Complaint: Case: No. Name: Ch. A Sex: Female Age: 5 Years Old No. Reg: 627575Document6 pagesChief Complaint: Case: No. Name: Ch. A Sex: Female Age: 5 Years Old No. Reg: 627575Mohamad ZulfikarNo ratings yet
- Case Report Dr. EduardDocument6 pagesCase Report Dr. EduardIrene Elysia GunawanNo ratings yet
- Morning Report 13 September 2019Document54 pagesMorning Report 13 September 2019ugd armyNo ratings yet
- Emergency Case Reports Tuesday, February 3 2020: Surgery DepartmentDocument22 pagesEmergency Case Reports Tuesday, February 3 2020: Surgery DepartmentAndi Nurjannah KaddirajaNo ratings yet
- Integrasi Igd Aortic DissectionDocument21 pagesIntegrasi Igd Aortic Dissectionrahageng wida kusumaNo ratings yet
- Second Announcement PIN IKABDIDocument18 pagesSecond Announcement PIN IKABDIFrancesc OktofabregasNo ratings yet
- Characteristic of Gastric Perforation Type and The Histopathology at Haji Adam Malik General Hospital Medan-IndonesiaDocument3 pagesCharacteristic of Gastric Perforation Type and The Histopathology at Haji Adam Malik General Hospital Medan-IndonesiaFrancesc OktofabregasNo ratings yet
- Cerebral ComplicationDocument6 pagesCerebral ComplicationFrancesc OktofabregasNo ratings yet
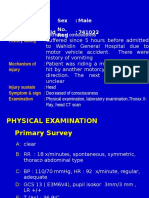
- No. Name: Mr. L Sex: Male Age: 20 Years Old No. Reg: 741022Document5 pagesNo. Name: Mr. L Sex: Male Age: 20 Years Old No. Reg: 741022Francesc OktofabregasNo ratings yet
- No. Nam E:mr. L Sex: Male Age:20 Years Old No. Reg: 741022Document5 pagesNo. Nam E:mr. L Sex: Male Age:20 Years Old No. Reg: 741022Francesc OktofabregasNo ratings yet
- Jurnal DigestiveDocument9 pagesJurnal DigestiveFrancesc OktofabregasNo ratings yet
- AUTOIMMUNITYDocument36 pagesAUTOIMMUNITYFrancesc OktofabregasNo ratings yet
- Anatomy Heart Homework (Due Mon. 3-9 1 or Tues. 3-10 2 /4) Vocabulary - Define The FollowingDocument2 pagesAnatomy Heart Homework (Due Mon. 3-9 1 or Tues. 3-10 2 /4) Vocabulary - Define The FollowingKameron WardNo ratings yet
- Neuromuscular Diseases PDFDocument205 pagesNeuromuscular Diseases PDFsalmazzNo ratings yet
- Sexual Function After Partial Penectomy For Penile CancerDocument4 pagesSexual Function After Partial Penectomy For Penile CancerNanang BumimasNo ratings yet
- The Medical Mystery of Vincent Van GoghDocument21 pagesThe Medical Mystery of Vincent Van Goghapi-243780701No ratings yet
- TKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Document6 pagesTKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Fayza RihastaraNo ratings yet
- Acute AppendicitisDocument70 pagesAcute AppendicitisTimbur IgorNo ratings yet
- Allport's Eight Stages of Self (Proprium) Development - The Mouse TrapDocument19 pagesAllport's Eight Stages of Self (Proprium) Development - The Mouse TrapiqrarifatNo ratings yet
- Proefschrift Karin Burgerhout PDFDocument198 pagesProefschrift Karin Burgerhout PDFsvetiljka100% (1)
- Research Article: International Journal of Public Health and Epidemiology ResearchDocument11 pagesResearch Article: International Journal of Public Health and Epidemiology ResearchPremier PublishersNo ratings yet
- IGCSE Bio Syllabys Guide 2015-2016Document21 pagesIGCSE Bio Syllabys Guide 2015-2016Saima IslamNo ratings yet
- CW1: Written Assessment LC666 Global Health and Society Module Leader: Bala Pokuboye-Amakiri Student Name: Student IDDocument10 pagesCW1: Written Assessment LC666 Global Health and Society Module Leader: Bala Pokuboye-Amakiri Student Name: Student IDchaturvedi.palash18No ratings yet
- Meaning and Scope of Medical AnthropologyDocument11 pagesMeaning and Scope of Medical AnthropologyInsane ReaderNo ratings yet
- CV of Jiaqi GaoDocument2 pagesCV of Jiaqi Gaoapi-455900676No ratings yet
- Case StudyDocument8 pagesCase Studyapi-402829443No ratings yet
- Olianna Peer DrakeDocument21 pagesOlianna Peer Drakenishink9No ratings yet
- Unsw Eet Thesis PosterDocument7 pagesUnsw Eet Thesis Postermoz1selajuk2100% (2)
- PaginieDocument7 pagesPaginiethe_szabikaNo ratings yet
- Bionematicides in Brazil RAPP 2022Document15 pagesBionematicides in Brazil RAPP 2022cporto_silvaNo ratings yet
- Molecules 26 07153 v21Document43 pagesMolecules 26 07153 v21Hà PhanNo ratings yet
- Uptodate Terms of Use: Author: Section Editor: Deputy EditorDocument18 pagesUptodate Terms of Use: Author: Section Editor: Deputy EditorXtineNo ratings yet
- Combined Vaccines TRS 980 Annex 6Document72 pagesCombined Vaccines TRS 980 Annex 6UniNo ratings yet
- Download ebooks file Handbook of Diabetes 4th Edition Rudy Bilous all chaptersDocument50 pagesDownload ebooks file Handbook of Diabetes 4th Edition Rudy Bilous all chaptersasmarsloanwf100% (9)
- Script For PresentationDocument5 pagesScript For PresentationSamuel LimNo ratings yet
- Chapter 7: Mood Disorders and SuicideDocument41 pagesChapter 7: Mood Disorders and SuicideEsraRamosNo ratings yet
- Essay Question RNA and DNA Structure and FunctionDocument1 pageEssay Question RNA and DNA Structure and FunctionInactiveAccount100% (5)
- HONCHI HO, HYOCHI HO: Root and Branch Treatment Staging in Contemporary Japanese AcupunctureDocument77 pagesHONCHI HO, HYOCHI HO: Root and Branch Treatment Staging in Contemporary Japanese Acupuncturekeiraku100% (3)
- Napolcom Review Handbook-39Document2 pagesNapolcom Review Handbook-39atom.suit235No ratings yet
- Dmac 15Document6 pagesDmac 1517BME3157 Raja pugalarasuNo ratings yet