Pemicu 7 Blok Saraf & Kejiwaan: Pandu 405140087
Pemicu 7 Blok Saraf & Kejiwaan: Pandu 405140087
Download as pptx, pdf, or txt
You might also like
- Oxford Library of Psychology Jon E Grant Marc N Potenza Editors The Oxford Handbook of Impulse Control Disorders Oxford University Press 2011 PDFDocument592 pagesOxford Library of Psychology Jon E Grant Marc N Potenza Editors The Oxford Handbook of Impulse Control Disorders Oxford University Press 2011 PDFLeo Souza100% (9)
- CRIM 3 Human Behavior and VictimologyDocument18 pagesCRIM 3 Human Behavior and VictimologyRommel Ilang-ilang94% (17)
- 165 AspectDocument5 pages165 AspectNena Stefanović100% (6)
- Females and Autism / Aspergers: A Checklist: Facebook Twitter Linkedin Pinterest Tumblr Email Reddit Print ShareDocument8 pagesFemales and Autism / Aspergers: A Checklist: Facebook Twitter Linkedin Pinterest Tumblr Email Reddit Print ShareMaria Zampetaki100% (1)
- Anxiety NotesDocument4 pagesAnxiety NotesketantchaudhariNo ratings yet
- Anxiety Disorder: College of NursingDocument10 pagesAnxiety Disorder: College of NursingAyr MasenasNo ratings yet
- Psychiatric Nursing ReviewDocument27 pagesPsychiatric Nursing Reviewgrey26No ratings yet
- AnxietyDocument55 pagesAnxietyAbelNo ratings yet
- Biological PerspectiveDocument4 pagesBiological Perspectivezeynub.khan12No ratings yet
- TOPIC: "Neurological and Psychological Disorders": Submitted by Submitted ToDocument15 pagesTOPIC: "Neurological and Psychological Disorders": Submitted by Submitted TosaymaNo ratings yet
- Anxiety DisordersDocument116 pagesAnxiety DisordersusamanurahmedNo ratings yet
- Literature ReviewDocument7 pagesLiterature ReviewResianaPutriNo ratings yet
- Anxiety Disorders Lesson PlanDocument32 pagesAnxiety Disorders Lesson PlanPedrosa NardNo ratings yet
- Nursing Notes: Tryptophan, A Dietary Amino AcidDocument25 pagesNursing Notes: Tryptophan, A Dietary Amino AcidJely BeanNo ratings yet
- Psychiatric Nursing ReviewDocument27 pagesPsychiatric Nursing ReviewbiopoolNo ratings yet
- BY Doon Psychothearaputic CentreDocument33 pagesBY Doon Psychothearaputic CentreRujuta BaramateNo ratings yet
- Urooj Zafar (Assignment)Document8 pagesUrooj Zafar (Assignment)Urooj ZafarNo ratings yet
- Hamilton Anxiety Rating Scale IntroductionDocument10 pagesHamilton Anxiety Rating Scale Introductionxijipe1553No ratings yet
- Psychosis and NeurosisDocument4 pagesPsychosis and NeurosisYashwanth VbNo ratings yet
- Gad 2Document21 pagesGad 2tendolsmithNo ratings yet
- Anxiolytic & Hypnotic Agents: Presented By: Tocpel, SDocument12 pagesAnxiolytic & Hypnotic Agents: Presented By: Tocpel, Sreinnard tocpelNo ratings yet
- Causes and Treatment of Panic DisorderDocument5 pagesCauses and Treatment of Panic DisorderAparajita GuinNo ratings yet
- Obsessive Compulsive Disorder OCDDocument6 pagesObsessive Compulsive Disorder OCDcaly.032803No ratings yet
- Anxiety Disorders - Lecture NotesDocument14 pagesAnxiety Disorders - Lecture NotesPeter Forster67% (3)
- SCHIZOPHRENIA, ResumeDocument14 pagesSCHIZOPHRENIA, ResumePatricia WenNo ratings yet
- Anxiety, Generalized Anxiety Disorder (GAD) : Go ToDocument6 pagesAnxiety, Generalized Anxiety Disorder (GAD) : Go ToLeonardo JeversonNo ratings yet
- Ocd AssignmentDocument12 pagesOcd Assignmentck234aksNo ratings yet
- Psychology 227 HW - 4 (1) ...Document6 pagesPsychology 227 HW - 4 (1) ...Brian ochiengNo ratings yet
- Definition of Reporting Anxiety DisorderDocument5 pagesDefinition of Reporting Anxiety DisorderBEA RADANo ratings yet
- Essay Mental HealthDocument2 pagesEssay Mental HealthFada Azkadina ZNo ratings yet
- Psychology Investigatory ProjectDocument18 pagesPsychology Investigatory Projectmaitreya.medhekarNo ratings yet
- Borderline Personality Disorder 4Document5 pagesBorderline Personality Disorder 4anicagomes16No ratings yet
- AnxietyDocument8 pagesAnxietyhmwdynfzmsmdNo ratings yet
- Physio Notes Midterm Quiz 1Document4 pagesPhysio Notes Midterm Quiz 1detarrocarenNo ratings yet
- Psychopathology PDFDocument26 pagesPsychopathology PDFBenedicte NtumbaNo ratings yet
- Chapter 13Document7 pagesChapter 13Chin SilverNo ratings yet
- M3 - Etiology and Treatment of Mental DisordersDocument41 pagesM3 - Etiology and Treatment of Mental DisordersCedric LosteNo ratings yet
- DepressionDocument23 pagesDepressionapi-263913260No ratings yet
- Generalized Anxiety Disorder: Prakash Gajbhiye M.Phil Clinical Psychology Gwalior Mansik ArogyashalaDocument72 pagesGeneralized Anxiety Disorder: Prakash Gajbhiye M.Phil Clinical Psychology Gwalior Mansik Arogyashalayoshita.chikkyNo ratings yet
- Lesson 6 - Anxiety Disorders and Mental Health ConditionsDocument20 pagesLesson 6 - Anxiety Disorders and Mental Health Conditionspatricia.prabuNo ratings yet
- The Biological Approach - KJDocument6 pagesThe Biological Approach - KJEshaNo ratings yet
- Interpersonal ConflictDocument7 pagesInterpersonal Conflicttadedagi880No ratings yet
- Psycho - Group AssignmentDocument20 pagesPsycho - Group AssignmentJonah the mixerNo ratings yet
- Neurotic Disorders and SomatisationDocument26 pagesNeurotic Disorders and SomatisationNaveen Eldose100% (1)
- Intro Psychological DisordersDocument39 pagesIntro Psychological DisordersMary Jo LegaspiNo ratings yet
- Depression - Monica PathakDocument10 pagesDepression - Monica PathakMehul PanchalNo ratings yet
- Chapter 17Document44 pagesChapter 17Qurrataini IbanezNo ratings yet
- Major Depression - Dysthymic DisorderDocument28 pagesMajor Depression - Dysthymic Disorderapi-3797941No ratings yet
- Rit Aec26 Unit 1 Lecture 2Document56 pagesRit Aec26 Unit 1 Lecture 2pshashank138No ratings yet
- Beck's Anxiety Inventory 033Document21 pagesBeck's Anxiety Inventory 033Tanvi SonawaneNo ratings yet
- Ltz-Psychodiagnostics Intro-Evolution, Growth and DevelopmentDocument88 pagesLtz-Psychodiagnostics Intro-Evolution, Growth and DevelopmentLucy RalteNo ratings yet
- Organic Delusional SyndromeDocument9 pagesOrganic Delusional Syndromehiranaeem222No ratings yet
- Leerdocument DMHDocument42 pagesLeerdocument DMHFlorien BuitendijkNo ratings yet
- Illness Anxiety Disorder: By: Florence Dominique T. RamirezDocument48 pagesIllness Anxiety Disorder: By: Florence Dominique T. RamirezChina VillanuevaNo ratings yet
- Calm and Centered: Overcoming Anxiety and Panic Attacks NaturallyFrom EverandCalm and Centered: Overcoming Anxiety and Panic Attacks NaturallyNo ratings yet
- The Anatomy of Anxiety: The Placebo vs Non-Placebo Approach:From EverandThe Anatomy of Anxiety: The Placebo vs Non-Placebo Approach:No ratings yet
- Conquering Anxiety: A Comprehensive Guide for Patients and Their FamiliesFrom EverandConquering Anxiety: A Comprehensive Guide for Patients and Their FamiliesNo ratings yet
- Beyond The Brain Re-Thinking Epilepsy Diagnosis And Treatment Through The Mind-Body ConnectionFrom EverandBeyond The Brain Re-Thinking Epilepsy Diagnosis And Treatment Through The Mind-Body ConnectionNo ratings yet
- Psicology, depression and humor disturbility: Understanding the basic mechanismsFrom EverandPsicology, depression and humor disturbility: Understanding the basic mechanismsNo ratings yet
- SULPYCO Method - A New Quantum and Integrative Approach to DepressionFrom EverandSULPYCO Method - A New Quantum and Integrative Approach to DepressionNo ratings yet
- Personal Letter B IngDocument8 pagesPersonal Letter B IngElsaNo ratings yet
- Jurnal ReadingDocument2 pagesJurnal ReadingElsaNo ratings yet
- Pemicu 2 Blok Kedaruratan Medis: Erika Juniartha Tungki 405150002Document78 pagesPemicu 2 Blok Kedaruratan Medis: Erika Juniartha Tungki 405150002ElsaNo ratings yet
- Pemicu 8 Blok Saraf & Kejiwaan: Pandu 405140087Document57 pagesPemicu 8 Blok Saraf & Kejiwaan: Pandu 405140087ElsaNo ratings yet
- New Genetic Findings Lead The Way To A Better Understanding of Fundamental Mechanisms of Drug HypersensitivityDocument9 pagesNew Genetic Findings Lead The Way To A Better Understanding of Fundamental Mechanisms of Drug HypersensitivityElsaNo ratings yet
- Pemicu 3: Irwan Surya Angkasa 405150170Document63 pagesPemicu 3: Irwan Surya Angkasa 405150170ElsaNo ratings yet
- Summary Book Abnormal Psychology Barlow Durand PDFDocument58 pagesSummary Book Abnormal Psychology Barlow Durand PDFLee DonghyuckNo ratings yet
- Ocd CaseDocument10 pagesOcd Casenaziaimam62No ratings yet
- Anxiety Disorders: David R. Rosenberg and Jennifer A. ChiribogaDocument10 pagesAnxiety Disorders: David R. Rosenberg and Jennifer A. ChiribogaMelissa CohenNo ratings yet
- WALDEN UNIVERSITY NRNP 6635 MID TERM 2021 Latest Questions and Answers All Correct Study Guide DownDocument95 pagesWALDEN UNIVERSITY NRNP 6635 MID TERM 2021 Latest Questions and Answers All Correct Study Guide Downerick kanyiNo ratings yet
- Anxiety Disorders BBDocument18 pagesAnxiety Disorders BBRyan Justin BoudreauxNo ratings yet
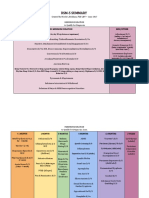
- DSM 5SummaryDurationPrevalencePeakOnsetDocument6 pagesDSM 5SummaryDurationPrevalencePeakOnsetClau Sali67% (3)
- (FREE PDF Sample) LaunchPad For Fundamentals of Abnormal Psychology Ronald J. Comer EbooksDocument49 pages(FREE PDF Sample) LaunchPad For Fundamentals of Abnormal Psychology Ronald J. Comer Ebooksnormiicocoa83100% (2)
- Poster Track2 Lisha 5973Document1 pagePoster Track2 Lisha 5973Lisha BalanNo ratings yet
- Neuropsychological Aspects of Tourette SyndromeDocument11 pagesNeuropsychological Aspects of Tourette SyndromeAndreia SilvaNo ratings yet
- Mental Status ExaminationDocument61 pagesMental Status ExaminationIsha AroraNo ratings yet
- NRSG 411 Exam 2 Blueprint Study GuideDocument25 pagesNRSG 411 Exam 2 Blueprint Study GuideEsther ONo ratings yet
- Module-1 Introduction To Geriatric DisordersDocument8 pagesModule-1 Introduction To Geriatric DisordersAshani AaroraNo ratings yet
- Obsessive Compulsive Related Disorders: PSYC 340Document21 pagesObsessive Compulsive Related Disorders: PSYC 340Sana FatimaNo ratings yet
- GENSLER - 2012 - Autism Spectrum Disorder in DSM-VDocument11 pagesGENSLER - 2012 - Autism Spectrum Disorder in DSM-VLoratadinaNo ratings yet
- Psychiatric and Mental Health NursingDocument56 pagesPsychiatric and Mental Health NursingBrielle ShoppNo ratings yet
- Internet Addiction EssayDocument1 pageInternet Addiction EssaymianliaqatwaqarNo ratings yet
- Schneider 2017Document9 pagesSchneider 2017Tasya Ajeng Trias PutriNo ratings yet
- Asian Journal of Psychiatry: Letter To The EditorDocument2 pagesAsian Journal of Psychiatry: Letter To The Editornofirly hamliNo ratings yet
- Study On Anxiety DisorderDocument18 pagesStudy On Anxiety DisorderRRRNo ratings yet
- Intensive Exposure and Response Prevention For Adolescent Body Dysmorphic Disorder With Comorbid Obsessive-Compulsive Disorder and Major Depressive DisorderDocument17 pagesIntensive Exposure and Response Prevention For Adolescent Body Dysmorphic Disorder With Comorbid Obsessive-Compulsive Disorder and Major Depressive DisorderkaiNo ratings yet
- Istanbul - OCD BBDocument1 pageIstanbul - OCD BBRajesh1861No ratings yet
- Psychiatry Finals - Passport 2nd Edition For Lambert PDFDocument110 pagesPsychiatry Finals - Passport 2nd Edition For Lambert PDFDoctor ShathaNo ratings yet
- Exercise 1Document20 pagesExercise 1Huyen Trang NguyenNo ratings yet
- Doce PDFDocument36 pagesDoce PDFCAMEVANo ratings yet
- DAILY MCQs With Answer and Reason PsychologyDocument6 pagesDAILY MCQs With Answer and Reason Psychologygetaravindh11No ratings yet
- Psychological Outlook of CinemaDocument10 pagesPsychological Outlook of CinemaDevesh PurbiaNo ratings yet