Sepsis & SIRS: Wade Woelfle, MD, FAAEM UW ECC 2016 June 21,2016
Sepsis & SIRS: Wade Woelfle, MD, FAAEM UW ECC 2016 June 21,2016
Download as pptx, pdf, or txt
You might also like
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideFrom EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideRating: 5 out of 5 stars5/5 (1)
- Kegawatan Bidang Penyakit Dalam GELSDocument55 pagesKegawatan Bidang Penyakit Dalam GELSwibowo0% (1)
- ROS ChecklistDocument3 pagesROS ChecklistPAschoolstuff100% (4)
- Case Study Breast CancerDocument25 pagesCase Study Breast CancerRalph Neil Manlutac100% (1)
- Sepsis & SIRS: Wade Woelfle, MD, FAAEM UW ECC 2016 June 21,2016Document44 pagesSepsis & SIRS: Wade Woelfle, MD, FAAEM UW ECC 2016 June 21,2016DaintyGarciaNo ratings yet
- Sepsis CmeDocument42 pagesSepsis CmeBonfaceNo ratings yet
- Pediatric Critical CareDocument3 pagesPediatric Critical CareRem Alfelor100% (1)
- Krisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranDocument67 pagesKrisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranLianSiahaanNo ratings yet
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocument34 pagesHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiNo ratings yet
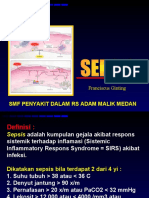
- Gambaran Klinis Dan Tatalaksana SepsisDocument35 pagesGambaran Klinis Dan Tatalaksana SepsisyunielsyaNo ratings yet
- Sepsis 23-24Document45 pagesSepsis 23-24mcmillanb2No ratings yet
- Management of Miscarriage and Sepsis: EsmoeDocument29 pagesManagement of Miscarriage and Sepsis: EsmoeLana LocoNo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- Acute Pancreatitis: Sarvodaya College of Nursing BangaloreDocument45 pagesAcute Pancreatitis: Sarvodaya College of Nursing BangaloreJeo ThomasNo ratings yet
- Journal Club Injamam 6.7.19 DENGUE FinalDocument34 pagesJournal Club Injamam 6.7.19 DENGUE Finalinjamam915No ratings yet
- Acute Trauma Care:: ShockDocument45 pagesAcute Trauma Care:: ShockGeoffrey100% (1)
- Patent Ductus ArteriosusDocument48 pagesPatent Ductus ArteriosusPaul A IBattledaily ScavellaNo ratings yet
- W2D3 DR - Yasa-Bacteremia Dan SepsisDocument54 pagesW2D3 DR - Yasa-Bacteremia Dan SepsisJaka BawaviNo ratings yet
- ShockDocument75 pagesShockaulianmediansyahNo ratings yet
- Sepsis and SIRSDocument24 pagesSepsis and SIRSFryda 'buona' YantiNo ratings yet
- Upper GI BleedingDocument30 pagesUpper GI BleedingBibek GhimireNo ratings yet
- Pulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistDocument34 pagesPulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistEmeka Chinedu Precious PetrousNo ratings yet
- Shock: Ibrahim Ali & Winfred C. ParnellDocument30 pagesShock: Ibrahim Ali & Winfred C. ParnellsgolbariNo ratings yet
- Exam 1 ReviewDocument5 pagesExam 1 ReviewbreNo ratings yet
- Sepsis (from Gr. Σ: Systemic inflammatory response syndromeDocument5 pagesSepsis (from Gr. Σ: Systemic inflammatory response syndromeReyes PaulNo ratings yet
- SepsisDocument18 pagesSepsisubaxlaska44No ratings yet
- Laboratory 1221572191937440 9Document144 pagesLaboratory 1221572191937440 9docprashNo ratings yet
- Sepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashaDocument38 pagesSepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashapashaNo ratings yet
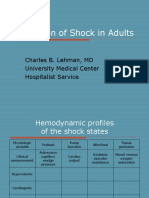
- Evaluation of Shock in AdultsDocument99 pagesEvaluation of Shock in AdultsekramsNo ratings yet
- Lecturer: Idol L. Bondoc, M.D.,R.NDocument58 pagesLecturer: Idol L. Bondoc, M.D.,R.NidolbondocNo ratings yet
- 13.30 DR Arunraj Navaratnarajah - The Septic PatientDocument49 pages13.30 DR Arunraj Navaratnarajah - The Septic PatientagusNo ratings yet
- VASCULITISDocument79 pagesVASCULITISSol CamusNo ratings yet
- Penyakit Vaskular PeriverDocument84 pagesPenyakit Vaskular PeriverFreandhy PutraNo ratings yet
- Diagnosis of Septic Shock G2Document70 pagesDiagnosis of Septic Shock G2Mohammed MagdyNo ratings yet
- Module 3 A PresentationDocument79 pagesModule 3 A PresentationMelinda FiskaNo ratings yet
- Krisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranDocument85 pagesKrisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranSeptian WidiantoNo ratings yet
- 3.kuliah Sepsis Malaysia UsuDocument42 pages3.kuliah Sepsis Malaysia UsuBaran PalanimuthuNo ratings yet
- Sepsis 2013Document42 pagesSepsis 2013RatnaNo ratings yet
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Document46 pagesPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- SEPSIS Doks.Document13 pagesSEPSIS Doks.futureevents872No ratings yet
- Amjad Bani Hani: Sir S, Sep S Is, A N D ModsDocument67 pagesAmjad Bani Hani: Sir S, Sep S Is, A N D ModsRuffaeelJabrNo ratings yet
- Evidence Based Management of Community Acquired PneumoniasDocument50 pagesEvidence Based Management of Community Acquired PneumoniasJindal Chest Clinic100% (1)
- Transplant Registrar BookletDocument9 pagesTransplant Registrar BookletSamiaNazNo ratings yet
- Transfusion Reactions AlphaDocument27 pagesTransfusion Reactions AlphabeautifulbeastNo ratings yet
- Rheumatic Fever: Prof. A K M MohibullahDocument42 pagesRheumatic Fever: Prof. A K M MohibullahNavojit ChowdhuryNo ratings yet
- Hemolytic-Uremic Syndrome: CausesDocument3 pagesHemolytic-Uremic Syndrome: CausesDwi Budi UtamiNo ratings yet
- HTN Majdi FinalDocument87 pagesHTN Majdi FinalYaacoub ChahineNo ratings yet
- Medical Assessment Qs 20160501Document10 pagesMedical Assessment Qs 20160501jaish8904No ratings yet
- Pulmonary Embolism: DR Ntambo L.KDocument43 pagesPulmonary Embolism: DR Ntambo L.Khazunga rayfordNo ratings yet
- Sepsis Kuliah Ukrida Edwin 2014 2 ADocument51 pagesSepsis Kuliah Ukrida Edwin 2014 2 Amau tauNo ratings yet
- Diagnostic TestsDocument85 pagesDiagnostic Testsmelchi santander goNo ratings yet
- 0930 - Lee Pulm HTNDocument32 pages0930 - Lee Pulm HTNAlejandro Kanito Alvarez SNo ratings yet
- Congestive Heart FailureDocument6 pagesCongestive Heart Failureseigelystic100% (1)
- Module 3 A PresentationDocument79 pagesModule 3 A PresentationJesus William Arizapana Mamani100% (1)
- Hemolytic Uremic Syndrome 8.13.18Document34 pagesHemolytic Uremic Syndrome 8.13.18Emily EresumaNo ratings yet
- Sirs & ModsDocument26 pagesSirs & Modsnerlyn silao50% (2)
- HTHSCI 2HH3 List of PathogensDocument4 pagesHTHSCI 2HH3 List of PathogenskristianNo ratings yet
- Septic Shock ManagementDocument34 pagesSeptic Shock ManagementGezu GemechisaNo ratings yet
- Shock in ChildrenDocument35 pagesShock in Childrenreemrida311No ratings yet
- Askep HipertensiDocument23 pagesAskep HipertensiTikaNo ratings yet
- HELLP Syndrome DR - SreevaniDocument29 pagesHELLP Syndrome DR - SreevaniNona Saudale100% (1)
- HTN CDocument26 pagesHTN CharviliaNo ratings yet
- Anamnesis FormatDocument2 pagesAnamnesis FormatScribdTranslationsNo ratings yet
- Achalasia: Tova Rainis Gastroenterology Unit Bnai-Zion Medical CenterDocument34 pagesAchalasia: Tova Rainis Gastroenterology Unit Bnai-Zion Medical CenterHasan Al-HabsyiNo ratings yet
- 11 Foods For Amazing Sex M16Document39 pages11 Foods For Amazing Sex M16Massimiliano Sabato0% (1)
- 8.tatalaksana Intoksikasi Asam Dan Basa KuatDocument33 pages8.tatalaksana Intoksikasi Asam Dan Basa KuatRezza PutriNo ratings yet
- 07aprc - SyokDocument28 pages07aprc - SyokSondang Herikson PanjaitanNo ratings yet
- wp2 FinalDocument3 pageswp2 Finalapi-523698524No ratings yet
- Cognitive Psychology JournalDocument3 pagesCognitive Psychology JournalMcKayla ChurchNo ratings yet
- REFERAT - Ppt.solusio Plasenta ItaDocument18 pagesREFERAT - Ppt.solusio Plasenta ItaMochammad Adam EldiNo ratings yet
- SLRC Handouts CHN OutlineDocument11 pagesSLRC Handouts CHN OutlineLot RositNo ratings yet
- REVALIDADocument53 pagesREVALIDAMercy Anne EcatNo ratings yet
- M2 Rad AnaDocument11 pagesM2 Rad AnaramilccabrigaNo ratings yet
- Kidney Diet Referral Form MNT 508Document2 pagesKidney Diet Referral Form MNT 508Suci AnggrainiNo ratings yet
- 1 IMCI IntroductionDocument13 pages1 IMCI IntroductionESTE CRECIA EDULLANTES BULLECERNo ratings yet
- Patient Pareeksha - Case Sheet Sample 1Document30 pagesPatient Pareeksha - Case Sheet Sample 1Krishnaswamy JajimoggalaNo ratings yet
- Toxic Plants in Traditional Indian Systems of Medicine: Thomas M.Walter, Gopi G.RadhaDocument8 pagesToxic Plants in Traditional Indian Systems of Medicine: Thomas M.Walter, Gopi G.Radharajesh_rajesh_rajeshNo ratings yet
- Stages of Infection & Chain of InfectionDocument29 pagesStages of Infection & Chain of Infectionkrenzoolo XDNo ratings yet
- Wesleyan: College of Nursing and Allied Medical SciencesDocument2 pagesWesleyan: College of Nursing and Allied Medical SciencesShane Aileen AngelesNo ratings yet
- Carolyn Smith-Morris - Lenore Manderson (Eds.) - Chronic Conditions, Fluid States - Chronicity and The Anthropology of Illness (2010)Document333 pagesCarolyn Smith-Morris - Lenore Manderson (Eds.) - Chronic Conditions, Fluid States - Chronicity and The Anthropology of Illness (2010)leoNo ratings yet
- CHN HandiesDocument10 pagesCHN HandiesFreeNursingNotesNo ratings yet
- Pain MedicationsDocument3 pagesPain Medicationsapi-3739910100% (1)
- The Evolution of MedicineDocument7 pagesThe Evolution of MedicineEva SheikhNo ratings yet
- NTA Chikungunya and DengueDocument6 pagesNTA Chikungunya and Denguemanasseetharama049No ratings yet
- PNLE III For Medical Surgical NursingDocument13 pagesPNLE III For Medical Surgical NursingZymer Lee Abasolo100% (1)
- Exclusive BreastfeedingDocument1 pageExclusive BreastfeedingLeah BancaleNo ratings yet
- Udan's Neuro, Musculoskel, EentDocument2 pagesUdan's Neuro, Musculoskel, EentReygie Marsada100% (4)
- Inguinal HerniaDocument6 pagesInguinal HerniaignatiuserikNo ratings yet
- AguidetorespiratorycodingDocument16 pagesAguidetorespiratorycodingSusan GleesonNo ratings yet
- DSSQ PDFDocument12 pagesDSSQ PDFKiyo Korean StationaryNo ratings yet