Breast and Nipple Conditions
Breast and Nipple Conditions
Download as ppt, pdf, or txt
You might also like
- Antenatal and Postnatal CareDocument12 pagesAntenatal and Postnatal CarehiwaNo ratings yet
- 39-Assessment of Fetal Well BeingDocument34 pages39-Assessment of Fetal Well Beingdr_asalehNo ratings yet
- Newborn of A Diabetic Melitus MotherDocument22 pagesNewborn of A Diabetic Melitus MotherDennis MiritiNo ratings yet
- Case Presewntation - C - SectionDocument12 pagesCase Presewntation - C - Sectionpriyanka67% (3)
- Hiv in Pregnant WomenDocument33 pagesHiv in Pregnant WomenWill CheahNo ratings yet
- BFHI Section 4Document94 pagesBFHI Section 4Aprilian Ayu SitaNo ratings yet
- Puerperal SepsisDocument22 pagesPuerperal SepsisSuhas IngaleNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument5 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- LegalaspectsDocument47 pagesLegalaspectssanthiyasandy100% (1)
- Dysfunctional Labour by Abhishek JaguessarDocument34 pagesDysfunctional Labour by Abhishek Jaguessarreedoye21No ratings yet
- High Risk PregnancyDocument33 pagesHigh Risk PregnancyDakshayini MbNo ratings yet
- Induction and Augmentation of Labor: By: Yibelu Bazezew (MSC in Clinical Midwifery)Document59 pagesInduction and Augmentation of Labor: By: Yibelu Bazezew (MSC in Clinical Midwifery)Yibelu BazezewNo ratings yet
- Antenatal Assessment of Fetal Well-BeingDocument18 pagesAntenatal Assessment of Fetal Well-BeingAmritaNo ratings yet
- Physiology of Lactation: Prepared By: Fy MSC NursingDocument32 pagesPhysiology of Lactation: Prepared By: Fy MSC NursingSùjâl PätídàrNo ratings yet
- OxytocinDocument1 pageOxytocinSubbie OutlierNo ratings yet
- Preconceptional CareDocument22 pagesPreconceptional CareSantosh KumariNo ratings yet
- ApgarDocument4 pagesApgarjaysille09100% (1)
- Preconception Care Presentation SlidesDocument15 pagesPreconception Care Presentation SlidesLucy AsconaNo ratings yet
- Birth Injuries: By: Murad Sawalha RN, MSNDocument18 pagesBirth Injuries: By: Murad Sawalha RN, MSNPriyanka JainNo ratings yet
- Primigravida Mothers Knowledge-2128Document15 pagesPrimigravida Mothers Knowledge-2128Mariecor EnriquezNo ratings yet
- Effectiveness of Planned Teaching Program On Knowledge of Immediate Postpartum Intrauterine Contraceptive Devices PPIUCD Among Antenatal Mothers in Selected Community Areas, DehradunDocument5 pagesEffectiveness of Planned Teaching Program On Knowledge of Immediate Postpartum Intrauterine Contraceptive Devices PPIUCD Among Antenatal Mothers in Selected Community Areas, DehradunEditor IJTSRDNo ratings yet
- Chapter 19 - Nutritional Needs of A NewbornDocument8 pagesChapter 19 - Nutritional Needs of A NewbornMerenisa LiminNo ratings yet
- Respiratory Problems in The NewbornDocument9 pagesRespiratory Problems in The NewbornIgwe SolomonNo ratings yet
- The High Risk New BornDocument23 pagesThe High Risk New Bornchhaiden100% (4)
- Brest Feeding - FinalDocument25 pagesBrest Feeding - FinalPranabh KushwahaNo ratings yet
- Breast FeedingDocument43 pagesBreast FeedingFetria Melani50% (2)
- A Study To Assess The Effectiveness of Planned Teaching Programme On Febrile Convulsions Among The Parents of Under 5 Children in BD Bhajoriya Rajkiya Hospital SaharanpurDocument4 pagesA Study To Assess The Effectiveness of Planned Teaching Programme On Febrile Convulsions Among The Parents of Under 5 Children in BD Bhajoriya Rajkiya Hospital SaharanpurEditor IJTSRDNo ratings yet
- Breast CareDocument2 pagesBreast Carearjuna rahmatNo ratings yet
- Prenatal Care by Connie Sussan AustenDocument31 pagesPrenatal Care by Connie Sussan AustenNoraNo ratings yet
- Abnormal Labour and It ManagementDocument27 pagesAbnormal Labour and It ManagementOsama AhmadNo ratings yet
- Rhesus Iso ImmunizationDocument12 pagesRhesus Iso Immunizationapi-3705046No ratings yet
- Missed AbortionDocument2 pagesMissed AbortionRyan MulanoNo ratings yet
- S.G.R.D Institution of Nursing (Pandher) : Lesson PlanDocument22 pagesS.G.R.D Institution of Nursing (Pandher) : Lesson PlanCharanNo ratings yet
- High Risk in PregnancyDocument3 pagesHigh Risk in PregnancyPrince Rudy DoctoleroNo ratings yet
- Deep Vein Thrombosis in Pregnancy - Epidemiology, Pathogenesis, and Diagnosis - UpToDateDocument26 pagesDeep Vein Thrombosis in Pregnancy - Epidemiology, Pathogenesis, and Diagnosis - UpToDateCristinaCaprosNo ratings yet
- Hepatitis in Pregnancy NewwDocument16 pagesHepatitis in Pregnancy Newwfarah betari100% (1)
- Prolonged LaborDocument13 pagesProlonged Laborsujinaranamagar18No ratings yet
- Breast FeedingDocument18 pagesBreast FeedingAnis Rakhmawati100% (1)
- CP PihDocument33 pagesCP PihArchita SharmaNo ratings yet
- Steps For Performing Manual Vacuum Aspiration (MVA) : Dr. Faten Al-ShargabiDocument2 pagesSteps For Performing Manual Vacuum Aspiration (MVA) : Dr. Faten Al-ShargabiMohammed Al-shargabi100% (1)
- Neonatal Seizures: Intr0DuctionDocument5 pagesNeonatal Seizures: Intr0DuctionsubashikNo ratings yet
- Magnesium Sulfate AdministrationDocument14 pagesMagnesium Sulfate AdministrationPATRIZJA YSABEL REYESNo ratings yet
- 1-Evidence Based Midwifery CareDocument11 pages1-Evidence Based Midwifery CarepriyankaNo ratings yet
- Baby Friendly HospitalDocument30 pagesBaby Friendly HospitalSarika YadavNo ratings yet
- Forceps DeliveryDocument13 pagesForceps DeliveryStar AlvarezNo ratings yet
- Hypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DDocument22 pagesHypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DMegha D100% (1)
- Drugs Used in ObstetricsDocument6 pagesDrugs Used in ObstetricsJubin RajuNo ratings yet
- 3 - Puerperium and LactationDocument29 pages3 - Puerperium and LactationKholoud KholoudNo ratings yet
- 1-Evidence Based Midwifery Care PDFDocument11 pages1-Evidence Based Midwifery Care PDFsinarNo ratings yet
- Breast FeedingDocument76 pagesBreast FeedingSanjeet DuhanNo ratings yet
- Nicu Class Room TeachingDocument18 pagesNicu Class Room Teachingsaritha Oruganti100% (2)
- 466-495 CH16 Lowdermilk - QXDDocument30 pages466-495 CH16 Lowdermilk - QXDHamss AhmedNo ratings yet
- Trail of LaborDocument5 pagesTrail of LaborNithiya NadesanNo ratings yet
- Cephalopelvic DisproportionDocument15 pagesCephalopelvic DisproportionPriscilla Sarah PayneNo ratings yet
- Partograph Literature ReviewDocument36 pagesPartograph Literature ReviewIrma Fatimah100% (2)
- Intranatal Care Plan-1Document23 pagesIntranatal Care Plan-1nathsujitkr1980No ratings yet
- Breast Cancer Awareness Among Pregnant Women at Hoima Regional Referral Hospital, Western UgandaDocument12 pagesBreast Cancer Awareness Among Pregnant Women at Hoima Regional Referral Hospital, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Tumors, Anomalies, Prolapse & Cyst With PregancyDocument97 pagesTumors, Anomalies, Prolapse & Cyst With PregancySumankumar 8099No ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- The Art or Practice of Using Herbs and Herbal Preparations To Maintain Health and To Prevent, Alleviate, or Cure DiseaseDocument15 pagesThe Art or Practice of Using Herbs and Herbal Preparations To Maintain Health and To Prevent, Alleviate, or Cure DiseasedaveNo ratings yet
- Is Synthesized and Secreted by The, and Regulates The Development, Growth, Pubertal Maturation, and Reproductive Processes of The BodyDocument2 pagesIs Synthesized and Secreted by The, and Regulates The Development, Growth, Pubertal Maturation, and Reproductive Processes of The BodydaveNo ratings yet
- Midwifery Research: Maria Teresa C. PadillaDocument45 pagesMidwifery Research: Maria Teresa C. PadilladaveNo ratings yet
- Community Health Nursing ProcessDocument35 pagesCommunity Health Nursing Processdave100% (1)
- Pencils Template: Great For School PresentationsDocument9 pagesPencils Template: Great For School PresentationsdaveNo ratings yet
- Specialized Community Health NursingDocument45 pagesSpecialized Community Health NursingdaveNo ratings yet
- Click To Edit Master Title StyleDocument5 pagesClick To Edit Master Title StyledaveNo ratings yet
- Making Your Hospital Mother Baby FriendlyDocument19 pagesMaking Your Hospital Mother Baby Friendlydave100% (2)
- Sess 6 How Milk Get FrombreastDocument30 pagesSess 6 How Milk Get FrombreastdaveNo ratings yet
- Sess 8 Practices That AssistDocument33 pagesSess 8 Practices That AssistdaveNo ratings yet
- Sess 4 Milk CodeDocument13 pagesSess 4 Milk CodedaveNo ratings yet
- Sess 1 Global StrategyDocument12 pagesSess 1 Global StrategydaveNo ratings yet
- Sess 2 Communication SkillsDocument66 pagesSess 2 Communication SkillsdaveNo ratings yet
- Medication: D I I T atDocument116 pagesMedication: D I I T atdaveNo ratings yet
- Nursing Jurisprudence: By: Atty Deirdree Codamon-Gallman, RNDocument66 pagesNursing Jurisprudence: By: Atty Deirdree Codamon-Gallman, RNdaveNo ratings yet
- Upaya Penurunan AKI Dan AKBDocument14 pagesUpaya Penurunan AKI Dan AKBJoshuaRobertoPratamaNo ratings yet
- The Feature of Postpartum Bues in Adolescent Mother in Sukowono, JemberDocument7 pagesThe Feature of Postpartum Bues in Adolescent Mother in Sukowono, JemberInatul AuliaNo ratings yet
- Cardiotocography: Reported by AGNES M. JARAYA, MDDocument73 pagesCardiotocography: Reported by AGNES M. JARAYA, MDMuriel FialiwanNo ratings yet
- SELASI ADZO KORLEY - Staff MidwifeDocument2 pagesSELASI ADZO KORLEY - Staff MidwifeSelasi KorleyNo ratings yet
- Prolonged LabourDocument3 pagesProlonged Labourannu panchalNo ratings yet
- Assignments, Chapter 15, Nursing Care of A Family During Labor and BirthDocument8 pagesAssignments, Chapter 15, Nursing Care of A Family During Labor and BirthGLORY MI SHANLEY CARUMBANo ratings yet
- Visting (EBR)Document3 pagesVisting (EBR)Christian HarvestNo ratings yet
- Maternal and Child Health ProgrammesDocument55 pagesMaternal and Child Health ProgrammesArchana Sahu100% (1)
- Ashrafian, Hutan Sunzi Surgical Philosophy Concepts of Modern Surgery Paralleled To Sun Tzus Art of WarDocument4 pagesAshrafian, Hutan Sunzi Surgical Philosophy Concepts of Modern Surgery Paralleled To Sun Tzus Art of WarWilliam AdiputraNo ratings yet
- Planned Home BirthDocument27 pagesPlanned Home BirthGratia EstherNo ratings yet
- Intra Uterin Fetal DeathDocument15 pagesIntra Uterin Fetal Deathanojan100% (1)
- Midwives: Valerie Gommon Midwifery Practice LTDDocument3 pagesMidwives: Valerie Gommon Midwifery Practice LTDAlex BekeNo ratings yet
- Adolphe Pinard (1844-1934) of Paris and Intrauterine Paediatric CareDocument3 pagesAdolphe Pinard (1844-1934) of Paris and Intrauterine Paediatric CareArliska WulandariNo ratings yet
- Mengstayehu- Research paper (1)Document50 pagesMengstayehu- Research paper (1)Tolessa SolomonNo ratings yet
- Prof. Patricia MotaDocument3 pagesProf. Patricia MotaMárciaValenteValenteNo ratings yet
- Robson Classification - Implementation ManualDocument56 pagesRobson Classification - Implementation ManualJuan Miguel PangilinanNo ratings yet
- Obg ResearchDocument15 pagesObg ResearchAGERI PUSHPALATHANo ratings yet
- Antenatal Prenatal Care: Early and Continuous Risk AssessmentDocument3 pagesAntenatal Prenatal Care: Early and Continuous Risk AssessmentAmalNo ratings yet
- WBUHS Obstetrics and Gynaecology Papers PDFDocument245 pagesWBUHS Obstetrics and Gynaecology Papers PDFAnangsha DattaNo ratings yet
- Asha Incentives PHC Dusi April 2022Document2 pagesAsha Incentives PHC Dusi April 2022Nani SaiNo ratings yet
- CV CorrectedDocument8 pagesCV CorrectedAbdulazeez AhmedNo ratings yet
- Comprehensive Exam NCM 350Document23 pagesComprehensive Exam NCM 350JustJ Things100% (2)
- 2022 Pro No.Document1,344 pages2022 Pro No.Cheska Fulminar PachecoNo ratings yet
- NCP Group TaskDocument2 pagesNCP Group TaskHILARY MAE MARINNo ratings yet
- Baby Book Template Free PrintablesDocument22 pagesBaby Book Template Free Printablesapi-537172848No ratings yet
- MCH 161118045354Document38 pagesMCH 161118045354SrideviRaviNo ratings yet
- Clinical Learning Model in Professional Midwifery Education ProgramDocument59 pagesClinical Learning Model in Professional Midwifery Education ProgramHana NazeefaNo ratings yet
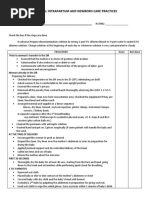
- Eesential Intrapartum and Newborn Care Practices - RleDocument2 pagesEesential Intrapartum and Newborn Care Practices - Rleding dutolloNo ratings yet
- NCP No. 1 (Postpartum Duty)Document2 pagesNCP No. 1 (Postpartum Duty)Chrizley Shawn DeroniaNo ratings yet