This document discusses different types of tibial fractures, including tibial plateau fractures, tibial shaft fractures, and pilon fractures of the distal tibia. It covers the anatomy, mechanisms of injury, classification systems, clinical presentation, investigations, treatment options, and potential complications for each type of tibial fracture. The goal of treatment is to obtain a stable, aligned, mobile, and pain-free joint while minimizing the risk of post-traumatic osteoarthritis.
This document discusses different types of tibial fractures, including tibial plateau fractures, tibial shaft fractures, and pilon fractures of the distal tibia. It covers the anatomy, mechanisms of injury, classification systems, clinical presentation, investigations, treatment options, and potential complications for each type of tibial fracture. The goal of treatment is to obtain a stable, aligned, mobile, and pain-free joint while minimizing the risk of post-traumatic osteoarthritis.
This document discusses different types of tibial fractures, including tibial plateau fractures, tibial shaft fractures, and pilon fractures of the distal tibia. It covers the anatomy, mechanisms of injury, classification systems, clinical presentation, investigations, treatment options, and potential complications for each type of tibial fracture. The goal of treatment is to obtain a stable, aligned, mobile, and pain-free joint while minimizing the risk of post-traumatic osteoarthritis.
This document discusses different types of tibial fractures, including tibial plateau fractures, tibial shaft fractures, and pilon fractures of the distal tibia. It covers the anatomy, mechanisms of injury, classification systems, clinical presentation, investigations, treatment options, and potential complications for each type of tibial fracture. The goal of treatment is to obtain a stable, aligned, mobile, and pain-free joint while minimizing the risk of post-traumatic osteoarthritis.
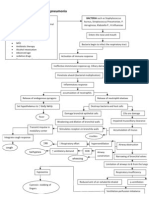
• History of trauma • Evaluate patient: ATLS principles. • Examine limbs for: • Bruises • Swelling • Deformity • Open wound • Absent or weak pulses • Sensation • Motor deficits/loss of function RADIOLOGICAL INX
X-RAY • AP and LAT views (rule of twos) • Oblique views at 45°(nondisplaced spiral #s)
• Note:# type Level Rotation Angulation Translation Shortening AO CLASSIFICATION CLASSIFICATION • AO TREATMENT
Goals of treatment: 1.Complete union 6 months without complications. 2.AP Angulation <10º 3.Varus / Valgus angulation <5º 4.Rotational alignment<10º 5.<1.5 cm of shortening Options for Treatment I. Non-operative Rx: 1. Plaster of Paris 2. Functional Bracing
II. Operative Rx.
1. Intramedullary Nailing 2. External Fixation 3. Plating POP
• Undisplaced/minimally displaced #s.
• Reduce under sedation • LLC 6-8wks with partial weight bearing • Then PTB cast 6-8wk WBAT. • PT Long leg Cast PTB CAST • A sarmiento cast Indications for operative RX
• Union in 95% cases. • Less suitable for #s near bone ends.
• Non-reamed im-nail for Gustilo I II and
IIIA IM NAILING EXTERNAL FIXATION
Main indication: Open #s. Poor surgical risk pt.
Advantage: Good access to soft tissue care. Avoids # site exposure Allows adjustments to be made PWB allowed. Compression. TIBIAL PLATEAU FRACTURES INTRODUCTION • Originally termed a bumper or fender fracture
• Force is directed from the femoral condyles onto
the medial and lateral portions of the tibial plateau,
• Young pt - # pattern = Splitting
• Older pt - # pattern = Depression/Comminution
Osseous Anatomy
Proximal Tibia Widens into lateral and medial tibial flares Flares lead to medial and lateral plateau (condyles) Intercondylar eminence Tibial tubercle (patellar tendon) Proximal tib/fib joint Epidemiology • Mean age in most series of tibial plateau fractures is about 55 years – Large percentage over age 60
• Comprise 1% of all # & 8% of all #in the elderly pop
• Older women >older men
Clinical Details
• Patients may present with:
– Knee pain – Knee effusion (Swelling) – Inability to bear weight on the limb Physical Exam
Vascular exam Popliteal artery and medial plateau injuries Beware of posteriorly displaced fracture fragments
Neurologic exam Peroneal nerve!
Ligamentous/ Meniscal injuries
Radiological investigations
• Include – AP
– Lateral
– Oblique views (40 degrees) if fracture not well
visualized. Radiographs CT image through tibia plateau Classification: Schatzker
I Type I: consists of a wedge fracture of the lateral tibial plateau, produced by low- force injuries. Classification: Schatzker
Type II: combines the
wedge fracture of the lateral plateau with depression of the lateral plateau.
II Classification: Schatzker
III Type III: fractures are classified as those with depression of the lateral plateau but no associated wedge fracture. Classification: Schatzker
Type IV is similar to type
I fracture, except that it involves the medial tibial plateau as opposed to the lateral plateau.
IV Classification: Schatzker
Type V fractures are
termed bicondylar and demonstrate wedge fractures of both the medial and lateral tibial plateaus.
V Classification: Schatzker
Type VI fractures consist
of a type V fracture along with a fracture of the underlying diaphysis and/or metaphysis.
VI The goals in treatment of a tibial plateau fracture are to obtain a stable, aligned, mobile, and painless joint and to minimize the risk of posttraumatic osteoarthritis. Urgent Treatment • Beware of Compartmental syndrome
• Provide temporary external stabilization
– Relieves pain – Stabilizes bone and soft tissues
• Consider spanning external fixation if:
– Complex fracture pattern – Large amount of shortening – Soft tissue conditions or other injuries make immediate ORIF unsafe Treatment …cont’d Most Shatzker #s treated operatively
Indication for surgery are:
– Fractures associated with instability, – Articular incongruity - 5mm young pt, 10mm elderly pt – Ligamentous injury, – Significant articular displacement; – Open fractures; and – Compartment syndrome Treatment …cont’d • Less than 5 mm in stable fractures, nonoperative, early motion and delayed weight-bearing. Prognosis
plafond #s • 85% fibula involvement • Risk of complications is high • Causes: – low-energy rotational forces – high-energy axial compression forces arising from MVA or falls from a height Epidemiology
• Less than 10 % of all lower extremity #
• Males > females
• Less common to children and elderly
• Average age 35 to 40 years
Classification cont… AO/OTA Radiological evaluation • X-ray; - Standard AP and LAT views plus
- Mortise view.
- Contra-lateral ankle X-ray (“template”)
• CT Scan Treatment
• Closed reduction & splinting – Role limited
– Applied in few injuries, minimal displaced Type A or Type C1 #s.
• However, true pilon # need ORIF
Complications
• Malunion • Non union and delayed union • Sepsis • Stiffness – ankle • Ankle OA