Acute Exacerbation of Asthma
Acute Exacerbation of Asthma
Download as pptx, pdf, or txt
You might also like
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanAl RizkyNo ratings yet
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- NR-37 - Dez 2018 - ENGDocument46 pagesNR-37 - Dez 2018 - ENGJohn TerryNo ratings yet
- Charlotte Pittar Resume 15 AugDocument2 pagesCharlotte Pittar Resume 15 Augapi-5278345660% (1)
- Asthma Clinical Care GuidelinesDocument17 pagesAsthma Clinical Care GuidelinesWalaa MoustafaNo ratings yet
- Case - Vii: AsthmaDocument18 pagesCase - Vii: AsthmaabubakarNo ratings yet
- ASTHMA exacerbation oral - نسخةDocument4 pagesASTHMA exacerbation oral - نسخةnoura ayedNo ratings yet
- Connections: Nursing Practice ApplicationDocument3 pagesConnections: Nursing Practice ApplicationadadanNo ratings yet
- Bronchial Asthma and Acute AsthmaDocument38 pagesBronchial Asthma and Acute AsthmaFreddy KassimNo ratings yet
- Farmakoterapi Asma Dan COPD - 2Document32 pagesFarmakoterapi Asma Dan COPD - 2Camboy D' JablezNo ratings yet
- Asthma Update: Thomas C. Bent, MD, FAAFP Infant, Child and Adolescent CourseDocument48 pagesAsthma Update: Thomas C. Bent, MD, FAAFP Infant, Child and Adolescent CourseSusie Marsick MartinNo ratings yet
- Farmakoterapi Asma Dan COPDDocument32 pagesFarmakoterapi Asma Dan COPDArif StOneNo ratings yet
- Clinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena AnjumDocument66 pagesClinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena Anjumgurrya786No ratings yet
- Parenteral Nutrition Basic IVT Nov 2008Document53 pagesParenteral Nutrition Basic IVT Nov 2008Crystal Mae Castrodes DaquipilNo ratings yet
- BRONCHIAL ASTHMA Presentation2Document40 pagesBRONCHIAL ASTHMA Presentation2Shami PokhrelNo ratings yet
- Acute Exacerbation of AsthmaDocument31 pagesAcute Exacerbation of AsthmaMuneeb YounisNo ratings yet
- Asthma EmergencyDocument20 pagesAsthma EmergencyJanice Shaileen KrishnaNo ratings yet
- BPOC in Medicina PrimaraDocument3 pagesBPOC in Medicina PrimaraAlina GheNo ratings yet
- Rotherham CCG Asthma Guidelines FINAL MMC Version V6.1Document6 pagesRotherham CCG Asthma Guidelines FINAL MMC Version V6.1Verónica Rojas NavaNo ratings yet
- Asthma DarshDocument33 pagesAsthma DarshNOWMANI A/P MUNUSAMY KPM-GuruNo ratings yet
- Niv in CopdDocument54 pagesNiv in Copdmahmod omerNo ratings yet
- عناية م 4Document85 pagesعناية م 4tbtv5wnm9jNo ratings yet
- Asthma: Diagnosis and Treatment GuidelineDocument27 pagesAsthma: Diagnosis and Treatment GuidelineDinar Riny Nv100% (1)
- Definition of Asthma: Controller) Medication Usually Prescribed inDocument5 pagesDefinition of Asthma: Controller) Medication Usually Prescribed inpiterwiselyNo ratings yet
- AsthmaDocument52 pagesAsthmaSummaiya AdnanNo ratings yet
- Membantu Pasien Dengan Gejala Dan Membawaa Produk ObatDocument13 pagesMembantu Pasien Dengan Gejala Dan Membawaa Produk ObatMisgi Candra DasaNo ratings yet
- Acute Severe Asthma (Status Asthmaticus)Document20 pagesAcute Severe Asthma (Status Asthmaticus)blok etikakedokteranNo ratings yet
- Pembimbing Dr. Arif Santoso, PHD, SP.P (K) Dr. Gunawan NursidDocument22 pagesPembimbing Dr. Arif Santoso, PHD, SP.P (K) Dr. Gunawan NursidgunawanNo ratings yet
- Asthmareview 240419194256 Ed3f497bDocument20 pagesAsthmareview 240419194256 Ed3f497bLamrani Fatima zahraNo ratings yet
- Olanzapine For Nausea and VomitingDocument42 pagesOlanzapine For Nausea and Vomitingsitiradziah subariNo ratings yet
- AsthmaDocument18 pagesAsthmaELDHOSE RAJUNo ratings yet
- Acute Asthma Exacerbations in Children PDFDocument17 pagesAcute Asthma Exacerbations in Children PDFmorksoldatNo ratings yet
- Guide For Diagnosis and Treatment: Bronchial Asthma in Children 6 Years. Update 2016. Executive SummaryDocument3 pagesGuide For Diagnosis and Treatment: Bronchial Asthma in Children 6 Years. Update 2016. Executive SummaryLuis MtzNo ratings yet
- Seminar Asthma PDFDocument39 pagesSeminar Asthma PDFAriff Mahdzub0% (1)
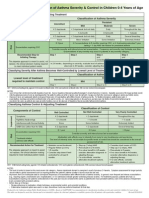
- NAEPP EPR-3 Classifi Cation of Asthma Severity & Control in Children 0-4 Years of AgeDocument1 pageNAEPP EPR-3 Classifi Cation of Asthma Severity & Control in Children 0-4 Years of AgeAdriel Chandra AngNo ratings yet
- ROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)Document45 pagesROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)rojosonNo ratings yet
- Reversible Airflow ObstructionDocument2 pagesReversible Airflow Obstruction85robertNo ratings yet
- Journal Reading AsthmaDocument12 pagesJournal Reading AsthmaMuhammad Ihsan AuliaNo ratings yet
- PROFESSOR ALAWLAQI BR.ASTHMADocument8 pagesPROFESSOR ALAWLAQI BR.ASTHMAMotea AlawlaqiNo ratings yet
- Asthma in Children My PresentationDocument49 pagesAsthma in Children My PresentationPutra Skate100% (4)
- BMC-NursingInitiatedSepsisProtocolDocument4 pagesBMC-NursingInitiatedSepsisProtocolemergenciashucssNo ratings yet
- Management of Asthma Exacerbations: Key Points: Early Treatment Is Best. Important Elements IncludeDocument47 pagesManagement of Asthma Exacerbations: Key Points: Early Treatment Is Best. Important Elements IncludeEmilio Fernandez CenturiónNo ratings yet
- It's All About Asthma Control: New Guidelines, New Treatment ApproachDocument16 pagesIt's All About Asthma Control: New Guidelines, New Treatment ApproachAli HaiderNo ratings yet
- Drug Study and NCP!Document8 pagesDrug Study and NCP!Abegail Abaygar100% (1)
- Conceptmaptext For EpDocument9 pagesConceptmaptext For Epapi-272402391No ratings yet
- Treatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsDocument65 pagesTreatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsLloyd Daniel BarrantesNo ratings yet
- Gina At-A-Glance Asthma Management Reference: OR ReproduceDocument4 pagesGina At-A-Glance Asthma Management Reference: OR ReproduceJeremy JasonNo ratings yet
- Generic Name:: Action: Indications: Adverse EffectsDocument6 pagesGeneric Name:: Action: Indications: Adverse EffectsuserringpointNo ratings yet
- Patient Management Flow Chart: Appt W/ Bronchoscopist PFT/ P&H/StabilityDocument7 pagesPatient Management Flow Chart: Appt W/ Bronchoscopist PFT/ P&H/StabilityKinnari PatelNo ratings yet
- Guidelines & Protocols: Advisory CommitteeDocument12 pagesGuidelines & Protocols: Advisory Committeedr_mahmudNo ratings yet
- Acute Exacerbation of AsthmaDocument21 pagesAcute Exacerbation of AsthmaMary AdetunjiNo ratings yet
- Session3 PPTDocument17 pagesSession3 PPTOsama HassanNo ratings yet
- Medical Management in GuillaIn Barre SyndromeDocument10 pagesMedical Management in GuillaIn Barre SyndromeRasilia MascarenhasNo ratings yet
- Managing Asthma During Pregnancy and Lactation: Mary Mcmahon, RNC, MsDocument61 pagesManaging Asthma During Pregnancy and Lactation: Mary Mcmahon, RNC, MsIlya RosdianaNo ratings yet
- Bronchial Asthma Final CompilationDocument51 pagesBronchial Asthma Final CompilationNurdalila ZabaNo ratings yet
- Bronchial Asthma in Children FdneDocument36 pagesBronchial Asthma in Children FdneRonit ChandNo ratings yet
- Modified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolDocument4 pagesModified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolElena DolcanNo ratings yet
- Daily Assessment of PatientsDocument9 pagesDaily Assessment of PatientsCarlos ZepedaNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Analysis / Inference Planning Intervention / Rationale EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Analysis / Inference Planning Intervention / Rationale EvaluationMon ManguilinNo ratings yet
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- Programas de La Carrera de Medicina de La Universidad de AzerbaijanDocument9 pagesProgramas de La Carrera de Medicina de La Universidad de AzerbaijanCarlos Gmo E. RamírezNo ratings yet
- Makino Edge-2 Pre-Installation ChecklistDocument120 pagesMakino Edge-2 Pre-Installation ChecklistViệt NguyễnNo ratings yet
- Desktop Surveillance Assessment (SHCO) Issue 1Document24 pagesDesktop Surveillance Assessment (SHCO) Issue 1Nidhi VijanNo ratings yet
- A Formal Model of ProcrastinationDocument8 pagesA Formal Model of ProcrastinationMagalyfloresgNo ratings yet
- Basic Measurements of EpidemiologyDocument51 pagesBasic Measurements of Epidemiologysunielgowda100% (1)
- Career Guide For International Students Graduate Diploma in TeachingDocument11 pagesCareer Guide For International Students Graduate Diploma in Teachingsandy mooNo ratings yet
- Resume - Vahideh Abrzadeh BayramiDocument3 pagesResume - Vahideh Abrzadeh Bayramimohammadrezahajian12191No ratings yet
- Electronic Document Management System (EDMS) Implementation: Implications For The Future of Digital Transformation in Philippine HealthcareDocument10 pagesElectronic Document Management System (EDMS) Implementation: Implications For The Future of Digital Transformation in Philippine HealthcareEthan OuroNo ratings yet
- A1 Wholesale PriceDocument2 pagesA1 Wholesale PriceNebiyat KitawNo ratings yet
- Sabias Que El Pan Es AzulDocument4 pagesSabias Que El Pan Es AzulPedroNo ratings yet
- Hospital A Complex EntityDocument4 pagesHospital A Complex EntitySamNo ratings yet
- DC2018 0223Document3 pagesDC2018 0223juris surgeonNo ratings yet
- Week 3Document8 pagesWeek 3Jhona Marie FuellasNo ratings yet
- Pemanfaatan Herbal Vagina Practice Dalam Budaya Wanita Madura Terhadap Flora Normal VaginaDocument7 pagesPemanfaatan Herbal Vagina Practice Dalam Budaya Wanita Madura Terhadap Flora Normal VaginaLeni listyowatiNo ratings yet
- Dysarthria PackDocument17 pagesDysarthria PackJayashri PrabakaranNo ratings yet
- Breaking The Silence Addressing Sexual Misconduct in HealthcareDocument36 pagesBreaking The Silence Addressing Sexual Misconduct in HealthcareMiguel Ángel Vallejos SánchezNo ratings yet
- Dilg Doh Jao 2020 0001Document31 pagesDilg Doh Jao 2020 0001Novie FeneciosNo ratings yet
- Study Guide Template EDITEDDocument5 pagesStudy Guide Template EDITEDRico EsponillaNo ratings yet
- Health Module For First QuarterDocument22 pagesHealth Module For First QuarterLorjnn LapinigNo ratings yet
- SGD Saipem Camp Accomodation and Building Facilities Job Safety Analysis Project Operational CampDocument3 pagesSGD Saipem Camp Accomodation and Building Facilities Job Safety Analysis Project Operational CampsalahnNo ratings yet
- Nilai Praktik BING 3Document23 pagesNilai Praktik BING 3Karin RinNo ratings yet
- (Fall 2011) CAS213 Persuasive Speech Outline - Go Greek: Eat Greek YogurtDocument5 pages(Fall 2011) CAS213 Persuasive Speech Outline - Go Greek: Eat Greek YogurtLaura Wake-RamosNo ratings yet
- Employee InvolvementDocument6 pagesEmployee InvolvementHarini Priyanka DravidaNo ratings yet
- 5 Steps To Developing An Abundance MindsetDocument8 pages5 Steps To Developing An Abundance MindsetCarlos HenryNo ratings yet
- Louise Kevin C. Belen Bsed-1K Activity 1. Presidential Decree No. 603 - Children and Youth Welfare CodeDocument16 pagesLouise Kevin C. Belen Bsed-1K Activity 1. Presidential Decree No. 603 - Children and Youth Welfare CodeLouise Kevin C. BelenNo ratings yet
- The Knowing Organization As Learning Organization: Chun Wei ChooDocument9 pagesThe Knowing Organization As Learning Organization: Chun Wei ChooMaristelaMesquitaNo ratings yet
- Willan V Willan DigestDocument1 pageWillan V Willan DigestIssa WagaNo ratings yet
- Pre-Final Examination in Physical Education and HealthDocument4 pagesPre-Final Examination in Physical Education and HealthJacquilou SalalimaNo ratings yet