Spiritualitas
Spiritualitas
Download as ppt, pdf, or txt
You might also like
- Religious Education Revision Booklet 2021Document108 pagesReligious Education Revision Booklet 2021kmakabe78No ratings yet
- 15 Quranic Passages o Levels Islamiyat Igcse GceDocument12 pages15 Quranic Passages o Levels Islamiyat Igcse Gcehasan mazahar67% (3)
- Religious Education For TavongaDocument102 pagesReligious Education For TavongaTlotlo carvin NthokgoNo ratings yet
- Fundamentals of Nursing Nclex RNDocument71 pagesFundamentals of Nursing Nclex RNspartacuslivesNo ratings yet
- Assignment in Spirituality: Submitted By: Jerald AquinoDocument14 pagesAssignment in Spirituality: Submitted By: Jerald AquinoJerald AquinoNo ratings yet
- Cultural Diversity: in Health CareDocument17 pagesCultural Diversity: in Health Careasta cloverNo ratings yet
- Funds Final BlueprintDocument5 pagesFunds Final BlueprintAudry GuillermoNo ratings yet
- World BeliefsDocument5 pagesWorld BeliefsSam BeltranNo ratings yet
- Religion Culture and NursingDocument27 pagesReligion Culture and NursingAdam Catane PalenNo ratings yet
- Running Head: Religion and Theology 1Document8 pagesRunning Head: Religion and Theology 1Sam OburuNo ratings yet
- TOPIC 12 RELIGION RELIGION ETHICS TRANSCULTURAL NURSING HandoutsDocument8 pagesTOPIC 12 RELIGION RELIGION ETHICS TRANSCULTURAL NURSING HandoutsSarmiento, Jovenal B.No ratings yet
- Assessing Spirituality and Religious Practices: Sherwyn U. Hatab RNDocument42 pagesAssessing Spirituality and Religious Practices: Sherwyn U. Hatab RNSherwyn Uy HatabNo ratings yet
- UTS Module 9-11Document22 pagesUTS Module 9-11mikaela thereseNo ratings yet
- Module 1Document12 pagesModule 1lesedimosarweNo ratings yet
- Spiritual AssessmentDocument4 pagesSpiritual AssessmentCharm ArroyoNo ratings yet
- Use of Religious Coping in Patients With CancerDocument10 pagesUse of Religious Coping in Patients With Cancersugarwhan39No ratings yet
- Euthanasia and ReligionDocument3 pagesEuthanasia and ReligionNavi VojNo ratings yet
- Ajayi Kirika Mavole Tradiitional Healing Practices YorubaDocument9 pagesAjayi Kirika Mavole Tradiitional Healing Practices YorubaJohnson MavoleNo ratings yet
- Health Care and Religious BeliefsDocument50 pagesHealth Care and Religious BeliefsLLyreONo ratings yet
- BuddhismDocument6 pagesBuddhismrpnguyenNo ratings yet
- Prayers and Rituals at a Time of Illness and Dying: The Practices of Five World ReligionsFrom EverandPrayers and Rituals at a Time of Illness and Dying: The Practices of Five World ReligionsRating: 4 out of 5 stars4/5 (2)
- Buddhism On Health and IllnessDocument7 pagesBuddhism On Health and IllnessKaren Angela PanganibanNo ratings yet
- Health Beliefs 2Document7 pagesHealth Beliefs 2api-283946728No ratings yet
- Nursing Role in Spiritual CareDocument51 pagesNursing Role in Spiritual CareKristian Dave Diva100% (2)
- Final Spiritual in NursingDocument2 pagesFinal Spiritual in NursingJinna JaneNo ratings yet
- Cultural Diversity in NursingDocument7 pagesCultural Diversity in NursingIconMaicoNo ratings yet
- Faith Healing Term PaperDocument4 pagesFaith Healing Term Paperafdtfngqb100% (1)
- Module 1 UBCV - SummerDocument27 pagesModule 1 UBCV - SummerjiyonpugiNo ratings yet
- Yr 11 Sor Preliminary Ibook 2015Document27 pagesYr 11 Sor Preliminary Ibook 2015jobinNo ratings yet
- Cultural Aspects of Death and DyingDocument4 pagesCultural Aspects of Death and DyingAliza BatongbakalNo ratings yet
- What Is Expected of Pastoral Care Practices?Document2 pagesWhat Is Expected of Pastoral Care Practices?Amanuel DiribaNo ratings yet
- Judaism Ha Group ProjectDocument14 pagesJudaism Ha Group Projectapi-546488467No ratings yet
- Islamic Medical Ethics: Kassim BaddarniDocument29 pagesIslamic Medical Ethics: Kassim BaddarniMuhammad Al Mutaaly BasriNo ratings yet
- Islam - BioethicsDocument29 pagesIslam - BioethicstrianaamaliaNo ratings yet
- Research Philo of Religion by Kenneth Ekene OnwusakaDocument15 pagesResearch Philo of Religion by Kenneth Ekene OnwusakaKenneth OnwusakaNo ratings yet
- Module 1 - Final VersionDocument24 pagesModule 1 - Final Versionktkutlo6No ratings yet
- Psychiatric Care in Asia Spirtuality and Religious Connotations - Chaudhry 2008Document8 pagesPsychiatric Care in Asia Spirtuality and Religious Connotations - Chaudhry 2008Mércia FiuzaNo ratings yet
- Exposing the Spiritual Roots of DiabetesDocument99 pagesExposing the Spiritual Roots of DiabetesSowmya PagadalaNo ratings yet
- Spiritual Aspect of Self (Vanessa).PDFDocument39 pagesSpiritual Aspect of Self (Vanessa).PDFadrianalexlauritoNo ratings yet
- CULMINATING - Week 1-2 - Topic 1 - INTRO TO WORLDDocument70 pagesCULMINATING - Week 1-2 - Topic 1 - INTRO TO WORLDlovelyn.capundanNo ratings yet
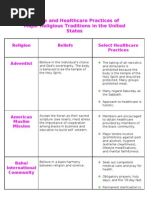
- Beliefs and Healthcare Practices of Major Religious Traditions in The United StatesDocument7 pagesBeliefs and Healthcare Practices of Major Religious Traditions in The United Statesilagan_tjNo ratings yet
- Secrets of Longevity, 2nd edition: Hundreds of Ways to Live to Be 100—The Bestselling Guide, Revised and ExpandedFrom EverandSecrets of Longevity, 2nd edition: Hundreds of Ways to Live to Be 100—The Bestselling Guide, Revised and ExpandedNo ratings yet
- HandOuts - Introduction To World Religions and Belief SystemsDocument4 pagesHandOuts - Introduction To World Religions and Belief SystemsRonibeMalinginNo ratings yet
- Spiritual Self 0Document32 pagesSpiritual Self 0alberthillaryeNo ratings yet
- Introduction To World Religions and Belief Systems 2Document15 pagesIntroduction To World Religions and Belief Systems 2edwin t. salvanera100% (1)
- Religious Education Notes-1Document100 pagesReligious Education Notes-1palesambalie828No ratings yet
- Week-1-WRDocument24 pagesWeek-1-WRriyopomporinNo ratings yet
- Religious Education NotesDocument101 pagesReligious Education NotestsholofelobapingNo ratings yet
- DocumentDocument5 pagesDocumenthauwau yusufNo ratings yet
- Healing From Within: Spirituality and Mental Health: Mental Health Is Much More Than The Absence of Mental IllnessDocument18 pagesHealing From Within: Spirituality and Mental Health: Mental Health Is Much More Than The Absence of Mental IllnessRista RiaNo ratings yet
- LESSON 2 - Effects of ReligionDocument2 pagesLESSON 2 - Effects of ReligionVictor Noel AlamisNo ratings yet
- Religious Practices Associated With Death and DyingDocument6 pagesReligious Practices Associated With Death and DyingSonny MadambaNo ratings yet
- Sunnah Health and Fitness PDFDocument108 pagesSunnah Health and Fitness PDFHealer Rahman AcupuncturistNo ratings yet
- Why ReligionDocument45 pagesWhy ReligionEbuddhsimNo ratings yet
- Additional Notes on Cultural PracticesDocument6 pagesAdditional Notes on Cultural PracticesJoana DupagonNo ratings yet
- Psychology of Spirituality and ReligionDocument23 pagesPsychology of Spirituality and ReligionXavier StaggNo ratings yet
- Fifth EditionDocument94 pagesFifth EditionkatkaisaraNo ratings yet
- REDocument104 pagesREmonamatiludo17No ratings yet
- Finals Week 1Document51 pagesFinals Week 1Lena Janelle LlamesNo ratings yet
- 035 Fatir-EngDocument49 pages035 Fatir-EngChern YuanNo ratings yet
- Tariqah Muhammadiyyah - EnglishDocument121 pagesTariqah Muhammadiyyah - Englishskquadri7100% (1)
- 99 Names of Allah & AyatsDocument6 pages99 Names of Allah & AyatssanNo ratings yet
- AmanullahDocument3 pagesAmanullahfaseeharain4586No ratings yet
- Dalail Al-Khayrat Hizb MondayDocument3 pagesDalail Al-Khayrat Hizb MondayShaiful BahariNo ratings yet
- Surah Al-Ghaafir (The Forgiver) : in The Name of Allah, The Beneficent, The MercifulDocument86 pagesSurah Al-Ghaafir (The Forgiver) : in The Name of Allah, The Beneficent, The MercifulMuhammad Farooq SaeedNo ratings yet
- The Gift of Durood and Salaam PDFDocument219 pagesThe Gift of Durood and Salaam PDFB Aris Wahyu Munandar100% (1)
- Traps of IblisDocument1 pageTraps of IblisMuhammed HishamNo ratings yet
- A Muslim's Character by Sheikh Muhammad Al-GhazaliDocument219 pagesA Muslim's Character by Sheikh Muhammad Al-Ghazalipurwantoasmuallaf100% (1)
- Darussalaam English .Document51 pagesDarussalaam English .Abu Ammar AsrafNo ratings yet
- ReportIqtisad G1Document26 pagesReportIqtisad G1KU MUHAMMAD ADLI SYAHMINo ratings yet
- The Islamic Will and TestamentDocument17 pagesThe Islamic Will and TestamentNasrin AktherNo ratings yet
- Surah Hujurat: The Name: Al-HujuratDocument12 pagesSurah Hujurat: The Name: Al-HujuratShehzad AliNo ratings yet
- Ash Shifa Shareef of Qadi Iyad Ibn Musa Al Yahsubi Radi Allahu AnhuDocument279 pagesAsh Shifa Shareef of Qadi Iyad Ibn Musa Al Yahsubi Radi Allahu AnhuZubair Ahmed100% (2)
- What Women Want?Document5 pagesWhat Women Want?Itz'a No-oneNo ratings yet
- SufsimDocument19 pagesSufsimkarayam2013No ratings yet
- Allama Iqbal Open UniversityDocument20 pagesAllama Iqbal Open UniversitySaba TanveerNo ratings yet
- The Holy Prophet (Salallaho Alaihi Wasallam) Is AliveDocument2 pagesThe Holy Prophet (Salallaho Alaihi Wasallam) Is AliveYaaRasoolallahNo ratings yet
- Seerah of The Prophet Mohammed (54) The Slander of Aisha, by Sheikh Yasir QadhiDocument7 pagesSeerah of The Prophet Mohammed (54) The Slander of Aisha, by Sheikh Yasir QadhiArslan TajammulNo ratings yet
- Prophet Muhammad in The BibleDocument21 pagesProphet Muhammad in The BibleleahdyanneNo ratings yet
- AssignmenNO ZUlfiqar AliDocument9 pagesAssignmenNO ZUlfiqar AliSAJJAD KHANNo ratings yet
- حضور ﷺکی زندگی کا ازدواجی پہلوDocument14 pagesحضور ﷺکی زندگی کا ازدواجی پہلوMuhammad NabeelNo ratings yet
- Allah means literally God in ArabicDocument17 pagesAllah means literally God in ArabicTausifNo ratings yet
- Islamic KnowledgeDocument16 pagesIslamic KnowledgeAlham DulillahNo ratings yet
- Sharah Aqeeda-e-TahawiyyahDocument202 pagesSharah Aqeeda-e-TahawiyyahaemNo ratings yet
- Overview of Surah BaqarahDocument5 pagesOverview of Surah BaqarahmieNo ratings yet
- Secrets of The DajjaalDocument9 pagesSecrets of The Dajjaalnisar.matadarNo ratings yet
- The Imperfection of The Q'uranDocument12 pagesThe Imperfection of The Q'urangretathungbergthugshakerNo ratings yet