Penile Ca
Penile Ca
Download as pptx, pdf, or txt
You might also like
- Small Animal OncologyDocument315 pagesSmall Animal OncologyMetka Trampuš100% (2)
- Extravasation Guidance PDFDocument24 pagesExtravasation Guidance PDFAdiAri RosiuNo ratings yet
- Diabetic Foot and Foot Debridement TechniqueDocument14 pagesDiabetic Foot and Foot Debridement TechniqueSidan EmozieNo ratings yet
- The 4th Edition of The Head and Neck WHO Blue BookDocument11 pagesThe 4th Edition of The Head and Neck WHO Blue Bookjarzcorpify100% (2)
- 40 Phimosis 1Document8 pages40 Phimosis 1Navis Naldo AndreanNo ratings yet
- Anatomy of Male Rep. SysDocument89 pagesAnatomy of Male Rep. Syszodo_izyanNo ratings yet
- Anatomy Urinary and Male Genital SystemDocument87 pagesAnatomy Urinary and Male Genital SystemHananya ManroeNo ratings yet
- Skin Cancer TBL 2 2f3Document19 pagesSkin Cancer TBL 2 2f3api-356476029No ratings yet
- Anorectal Malformatio N: Dr. O. Sankoh M.D. House Officer Pediatric SurgeryDocument123 pagesAnorectal Malformatio N: Dr. O. Sankoh M.D. House Officer Pediatric SurgeryMohamed KamaraNo ratings yet
- Malignant Disease of The JawsDocument26 pagesMalignant Disease of The JawsRawda NajjarNo ratings yet
- Dr. Dimyati Achmad SPB (K) Onk. (The Management of Thyroid Nodule 2022)Document41 pagesDr. Dimyati Achmad SPB (K) Onk. (The Management of Thyroid Nodule 2022)dewiswahyu100% (1)
- Total Penectomy Urooncology 12thDocument10 pagesTotal Penectomy Urooncology 12thdr. Joko WibowoNo ratings yet
- Clinical Review - Full PDFDocument6 pagesClinical Review - Full PDFDewi WulansariNo ratings yet
- Skin TumorsDocument56 pagesSkin TumorsAriba Asif100% (1)
- Circumcision in Baby BoysDocument6 pagesCircumcision in Baby BoysJbl2328No ratings yet
- SoTM StaplingDocument20 pagesSoTM StaplingIndrawan Buleth100% (1)
- By: Shrijan Timalsina, Samir Ghimire For-Dr - UMSD, DR - RJ Urosurgery Surgery DepartmentDocument30 pagesBy: Shrijan Timalsina, Samir Ghimire For-Dr - UMSD, DR - RJ Urosurgery Surgery DepartmentSamir GhimireNo ratings yet
- Ca PenisDocument25 pagesCa Penisrajan kumar100% (2)
- BPHDocument10 pagesBPHMichelle SalimNo ratings yet
- VaricoceleDocument19 pagesVaricoceleMariam AntonyNo ratings yet
- Management of Penile FractureDocument4 pagesManagement of Penile Fracturemissvi86No ratings yet
- Orbitotomi MedscapeDocument9 pagesOrbitotomi MedscapeBonita AsyigahNo ratings yet
- Wiringtechniquesinmaxillofacialsurgery 121205104837 Phpapp01Document41 pagesWiringtechniquesinmaxillofacialsurgery 121205104837 Phpapp01Dhini AnggrianiNo ratings yet
- Endometrial CancerDocument9 pagesEndometrial CancerAhmed Butt100% (1)
- SMS Medical College, Jaipur Department of UrologyDocument29 pagesSMS Medical College, Jaipur Department of UrologyNarendraNo ratings yet
- Intestinal Stomas PDFDocument10 pagesIntestinal Stomas PDFAmyandNo ratings yet
- BiopsyDocument49 pagesBiopsyShruti GargNo ratings yet
- Neligan Mandible FractureDocument17 pagesNeligan Mandible FractureRibka TheodoraNo ratings yet
- What's New in Skin Cancer TreatmentDocument56 pagesWhat's New in Skin Cancer TreatmentNational Press Foundation100% (1)
- HaematuriaDocument25 pagesHaematuriaAhmed BassettNo ratings yet
- Complications of PCNL: DR - Sanjay S Deshpande Sidheshwar Urological Society SolapurDocument20 pagesComplications of PCNL: DR - Sanjay S Deshpande Sidheshwar Urological Society SolapurAlat MasakNo ratings yet
- Laparoscopic Resection of Rectal CancerDocument4 pagesLaparoscopic Resection of Rectal CancerhoangducnamNo ratings yet
- Tg13: Updated Tokyo Guidelinesfor Acute CholecystitisDocument59 pagesTg13: Updated Tokyo Guidelinesfor Acute CholecystitisDeoValendraNo ratings yet
- Fournier's Gangrene EmergencyDocument4 pagesFournier's Gangrene EmergencyLalo ZaraloNo ratings yet
- Bladder InjuriesDocument13 pagesBladder InjuriesSchoeb MuhammadNo ratings yet
- Clinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaDocument17 pagesClinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaAlivia HanumNo ratings yet
- Descending Necrotizing MediastinitisDocument21 pagesDescending Necrotizing MediastinitisLaksmi Dewi SaputriNo ratings yet
- Dokumen - Tips RirsDocument98 pagesDokumen - Tips RirsBela RonaldoeNo ratings yet
- Breast Reconstruction After Mastectomy For Breast Tumor: About 24 CasesDocument6 pagesBreast Reconstruction After Mastectomy For Breast Tumor: About 24 CasesIJAR JOURNALNo ratings yet
- Wound de His Cence FinalDocument26 pagesWound de His Cence Finaldanil armandNo ratings yet
- Chapter 5 ATLSDocument27 pagesChapter 5 ATLSUlfaa MutiaaNo ratings yet
- Prevention of Pin Site Infection in External FixatioDocument11 pagesPrevention of Pin Site Infection in External FixatioKim Gabrielle Exene LeeNo ratings yet
- Basic Surgical SkillDocument19 pagesBasic Surgical Skillshadhana sivakumarNo ratings yet
- Microtia Recon Slides 0410Document31 pagesMicrotia Recon Slides 0410Josue Salinas SantosNo ratings yet
- Hernia - Hernioplasty With Bilayer Polypropylene Mesh PDFDocument4 pagesHernia - Hernioplasty With Bilayer Polypropylene Mesh PDFAnonymous YLmmme4XX0No ratings yet
- Cystostomy NewDocument32 pagesCystostomy Newkuncupcupu1368No ratings yet
- Diagnostic Tools in ObgynDocument27 pagesDiagnostic Tools in ObgynHenok Y KebedeNo ratings yet
- Microsoft Word - Neutropenic FeverDocument1 pageMicrosoft Word - Neutropenic FeverJoão Paulo GregorioNo ratings yet
- FibromaDocument2 pagesFibromaDevita Indyana PutriNo ratings yet
- 2014-06-03-Anterior Abdominal Wall Slides PDFDocument18 pages2014-06-03-Anterior Abdominal Wall Slides PDFGrigore PopaNo ratings yet
- Incision and DrainageDocument33 pagesIncision and DrainagemathisyncNo ratings yet
- Cafe Au Lait SpotsDocument2 pagesCafe Au Lait SpotsDanushNo ratings yet
- Aseptic TechniqueDocument37 pagesAseptic Techniquejiregna eticha dakoNo ratings yet
- 23.04.12 - Should Circumcision Be Banned - EnglishDocument3 pages23.04.12 - Should Circumcision Be Banned - Englishchristobran100% (1)
- The Transverse Rectus Abdominus Myocutaneous (Tram) FlapDocument25 pagesThe Transverse Rectus Abdominus Myocutaneous (Tram) FlapyahyaNo ratings yet
- Breast DiseasesDocument35 pagesBreast Diseasesheba1997bshNo ratings yet
- Penile Cancer 2010Document28 pagesPenile Cancer 2010raghavagummadiNo ratings yet
- NEW-EVLT Phlebology LaserDocument5 pagesNEW-EVLT Phlebology LaserJesús JoveNo ratings yet
- Basics - of - CT Scan (Lovish Vij Eic 2 101285007)Document39 pagesBasics - of - CT Scan (Lovish Vij Eic 2 101285007)Nav Gulshan100% (1)
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Acute Appendic ItsDocument24 pagesAcute Appendic ItsDr-Wisam Mhmd AliNo ratings yet
- FibroidDocument15 pagesFibroidNirupama KsNo ratings yet
- Tumor Palpebra 2Document6 pagesTumor Palpebra 2santiNo ratings yet
- 1-Minute Animation - What Is A Cancer Stem CellDocument7 pages1-Minute Animation - What Is A Cancer Stem CellEwerson MatiaNo ratings yet
- CPC RIK 5 Jurnal EngDocument6 pagesCPC RIK 5 Jurnal EngFellita Ratri ANo ratings yet
- Guyabano Fruit Acknowledged As A Miracle Cure For CancerDocument3 pagesGuyabano Fruit Acknowledged As A Miracle Cure For CancerZena BezabihNo ratings yet
- Journal Reading Firstiafina Tiffany - CompressedDocument14 pagesJournal Reading Firstiafina Tiffany - CompressedFirstiafina TiffanyNo ratings yet
- Thesis Statement For Informative Speech On Breast CancerDocument6 pagesThesis Statement For Informative Speech On Breast Cancerlucienicolasstockton100% (1)
- Malignant Tumors FESSHDocument40 pagesMalignant Tumors FESSHProfesseur Christian DumontierNo ratings yet
- Dr. Alban-ODP 2016 SarcomaDocument37 pagesDr. Alban-ODP 2016 SarcomaAfraDewitaNo ratings yet
- Brittni Mckane Clin Onc AssignDocument18 pagesBrittni Mckane Clin Onc Assignapi-569589889No ratings yet
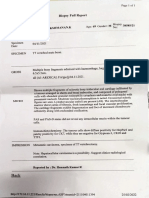
- Biopsy Report LakshmananDocument1 pageBiopsy Report LakshmananRJIO NAGPURNo ratings yet
- Lactating Adenoma A Case ReportDocument3 pagesLactating Adenoma A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Connective Tissue NeoplasmsDocument70 pagesConnective Tissue NeoplasmsB AlhashimiNo ratings yet
- Pancreas: Kurt'S NotesDocument3 pagesPancreas: Kurt'S NotesfadoNo ratings yet
- Skin PathologyDocument1 pageSkin PathologySean KeenanNo ratings yet
- Vulva CancerDocument2 pagesVulva CancerLim Hui ZhuanNo ratings yet
- Eye Pathology: Dr. Jusuf FantoniDocument8 pagesEye Pathology: Dr. Jusuf Fantonitutor tujuhNo ratings yet
- Pancreas-And Pylorus-Preserving Duodenectomy For Advanced Familial Duodenal PolyposisDocument7 pagesPancreas-And Pylorus-Preserving Duodenectomy For Advanced Familial Duodenal PolyposisRafaella dos Santos RamosNo ratings yet
- Basal Cell CarcinomaDocument21 pagesBasal Cell CarcinomaRicky ChanNo ratings yet
- Lung Cancer EgansDocument15 pagesLung Cancer Eganslady birdNo ratings yet
- Braquiterapia Baja DosisDocument9 pagesBraquiterapia Baja Dosisb4tipibeNo ratings yet
- Rubin - Ovarian Cancer 2ed PDFDocument207 pagesRubin - Ovarian Cancer 2ed PDFfdroooNo ratings yet
- Breast Surgeon in Pune - Dr. Swati SuradkarDocument8 pagesBreast Surgeon in Pune - Dr. Swati SuradkarSwati SuradkarNo ratings yet
- 基于机器学习的前列腺癌内脏转移预测模型的建立及验证 张泽郡Document50 pages基于机器学习的前列腺癌内脏转移预测模型的建立及验证 张泽郡cinkiahuaNo ratings yet
- Contoh Exp4Document7 pagesContoh Exp4Salsabila DindaNo ratings yet
- A Review of The Role of Carcinoembryonic Antigen IDocument12 pagesA Review of The Role of Carcinoembryonic Antigen IMarcellia AngelinaNo ratings yet
- Freeman 1962Document5 pagesFreeman 1962Cata RodriguezNo ratings yet
- CV Jatin S GandhiDocument5 pagesCV Jatin S GandhiSanjoy SanyalNo ratings yet