Cardiovascular System
Cardiovascular System
Download as pptx, pdf, or txt
You might also like
- Exam Qs C-172 Poh Supplement ThielertDocument108 pagesExam Qs C-172 Poh Supplement ThielertSaheb SinghNo ratings yet
- 5 Essential Guides To Bead StitchingDocument31 pages5 Essential Guides To Bead StitchingKarla100% (18)
- Cardiovascular Examination FinalDocument28 pagesCardiovascular Examination FinalAllen Caine Taabbil100% (1)
- Practical of Arterial Pulse For 1st Year Mbbs StudentsDocument7 pagesPractical of Arterial Pulse For 1st Year Mbbs StudentsMudassar Roomi67% (6)
- WorksheetDocument6 pagesWorksheetJon BennettNo ratings yet
- 7 Speed DSG VW 0AM - 0CW - DQ200 and Repair Measures - Sheng Hai Au182338Document12 pages7 Speed DSG VW 0AM - 0CW - DQ200 and Repair Measures - Sheng Hai Au182338Nitin Patil100% (2)
- Hvorslevs ParametersDocument19 pagesHvorslevs ParametersWaqas HassanNo ratings yet
- Examination and Investigation of The Cardiovascular System (CVS)Document27 pagesExamination and Investigation of The Cardiovascular System (CVS)Jake MillerNo ratings yet
- Cardiac ExaminationDocument21 pagesCardiac ExaminationPraneetha NouduriNo ratings yet
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument46 pagesCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaNo ratings yet
- General Examination v7Document64 pagesGeneral Examination v7Fariha RabiaNo ratings yet
- Cardiovascular System, Questioning and Examination of Patients With Pathology of The Cardiovascular System.Document20 pagesCardiovascular System, Questioning and Examination of Patients With Pathology of The Cardiovascular System.ASAP teleNo ratings yet
- CVS ExaminationDocument72 pagesCVS ExaminationDivya JyothiNo ratings yet
- Cardiovascular Examination OSCE Guide2Document33 pagesCardiovascular Examination OSCE Guide2محمد حميدNo ratings yet
- Cardiovascular Assessment (1) - StudentsDocument70 pagesCardiovascular Assessment (1) - Studentsraima ayazNo ratings yet
- Skills in CV1Document7 pagesSkills in CV1dtimtimanNo ratings yet
- Cardiovascular AssessmentDocument73 pagesCardiovascular AssessmentmatthewsarfrazbhattiNo ratings yet
- Cardiovascular Examination:: General InspectionDocument6 pagesCardiovascular Examination:: General InspectionPhysician AssociateNo ratings yet
- 1-7 Levick and Dwight - CardiovascularDocument7 pages1-7 Levick and Dwight - Cardiovascularrahmawati aliwarmanNo ratings yet
- CardiacassessmentDocument40 pagesCardiacassessmentsasNo ratings yet
- CynosisDocument16 pagesCynosisvdevrvdhtvdrvdutrrytdNo ratings yet
- Assessment of Artery and VeinDocument60 pagesAssessment of Artery and VeinEARL GERALD RICAFRANCANo ratings yet
- Systematic Examination of Cardiovascular SystemDocument25 pagesSystematic Examination of Cardiovascular Systemmaliknaz567No ratings yet
- Presentation B. INGGRIS FIKS BUK PUPUTDocument52 pagesPresentation B. INGGRIS FIKS BUK PUPUTRosy OktaridaNo ratings yet
- 3&4&5-Assessment of Peripheral Vascular SystemDocument43 pages3&4&5-Assessment of Peripheral Vascular SystemKhaled Mohamed AssemNo ratings yet
- Assessment Cardiac SystemDocument51 pagesAssessment Cardiac Systemejarnmd100% (2)
- Cardiology (1)Document133 pagesCardiology (1)Ryan KadavilNo ratings yet
- Semi CoaDocument19 pagesSemi Coa31 PASION, ROCHELLE C.No ratings yet
- 1.Arterial PulseDocument23 pages1.Arterial Pulsesalihvm100No ratings yet
- Cardiovascular Physical Examination.pptxDocument74 pagesCardiovascular Physical Examination.pptxNneoma OsakweNo ratings yet
- Cardiovascular History Taking and Physical ExaminationsDocument35 pagesCardiovascular History Taking and Physical ExaminationsEndalk AsfawNo ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- Paediatric Cardiovascular Examination OSCE GuideDocument24 pagesPaediatric Cardiovascular Examination OSCE GuideJeremiah KollieNo ratings yet
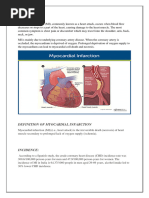
- Myocardial InfarctionDocument42 pagesMyocardial Infarctionarif mahammad bhuniyaNo ratings yet
- VSD NotesDocument7 pagesVSD Noteshyamaemartinez101No ratings yet
- Cardiovascular System Physical Examination ApproachDocument41 pagesCardiovascular System Physical Examination Approachlampido90No ratings yet
- CVS ExaminationDocument72 pagesCVS ExaminationPrashanthBhatNo ratings yet
- mod-3-NCM-118Document40 pagesmod-3-NCM-118Rebb PikitpikitNo ratings yet
- Congenital Heart Defects Ii-1Document46 pagesCongenital Heart Defects Ii-1berdonfelix495No ratings yet
- Review of Literature A. Overview of Cardiovascular System: Mitral Valve InsufficiencyDocument10 pagesReview of Literature A. Overview of Cardiovascular System: Mitral Valve InsufficiencyCha AlegriaNo ratings yet
- CM3 - Cu13 Assessment of Peripheral Vascular SystemDocument12 pagesCM3 - Cu13 Assessment of Peripheral Vascular Systemeli pascualNo ratings yet
- 50 Nursing Mnemonics and Acronyms You Need To Know NowDocument29 pages50 Nursing Mnemonics and Acronyms You Need To Know NowNaveen ShrivasNo ratings yet
- Assessment of CvsDocument70 pagesAssessment of CvsTouseeq ManzoorNo ratings yet
- Cardiovascular Exam: Examination Includes The FollowingDocument37 pagesCardiovascular Exam: Examination Includes The FollowingyayayanizaNo ratings yet
- 6 Peripheral Musculoskeletal SystemDocument15 pages6 Peripheral Musculoskeletal SystemGLORY MI SHANLEY CARUMBANo ratings yet
- Clinical Examination of CVSDocument33 pagesClinical Examination of CVSmahnoorNo ratings yet
- Heart and Central VesselDocument33 pagesHeart and Central Vesselseanandreigregorio.samaniegoNo ratings yet
- Assessment of The Normal Cardiovascular SystemDocument2 pagesAssessment of The Normal Cardiovascular SystemAieNo ratings yet
- Cardiovascular System (1)Document6 pagesCardiovascular System (1)amz7rewardsNo ratings yet
- Cardiovascular SystemDocument44 pagesCardiovascular SystemGatar Alnada AlhabibNo ratings yet
- Pericardial EffusionDocument26 pagesPericardial EffusionjsenocNo ratings yet
- Ha Lec 12 13Document23 pagesHa Lec 12 13Althea Sachi CruzNo ratings yet
- Cardiovascular Notes - Paediatrics ExaminationDocument5 pagesCardiovascular Notes - Paediatrics ExaminationPraveenNo ratings yet
- The Cardiovascular System Examination DR ALI SHEIKHDocument50 pagesThe Cardiovascular System Examination DR ALI SHEIKHRayyanNo ratings yet
- cardiovascular examination v1Document12 pagescardiovascular examination v1Fariha RabiaNo ratings yet
- MTE DR Mefri Cardiac ExaminationDocument36 pagesMTE DR Mefri Cardiac ExaminationMuhammad Thariq Isnaini100% (1)
- IM 3A PE Cardiology Dr. JumangitDocument12 pagesIM 3A PE Cardiology Dr. JumangitCzara DyNo ratings yet
- CVS OsceDocument19 pagesCVS OsceAbby LiewNo ratings yet
- Atrial Septal Defects: Presented by Dr. Maysa Abdul Haq Directed by Dr. Ali Halabi Jordan Hospital 11-9-2005Document36 pagesAtrial Septal Defects: Presented by Dr. Maysa Abdul Haq Directed by Dr. Ali Halabi Jordan Hospital 11-9-2005Joe JosephNo ratings yet
- Cardiovascular Assessment DDocument8 pagesCardiovascular Assessment Davinash dhameriyaNo ratings yet
- Congenital Disorder ASD VSDDocument50 pagesCongenital Disorder ASD VSDSachin DwivediNo ratings yet
- Assessment of Cardiovascular SystemDocument5 pagesAssessment of Cardiovascular SystemAnamika ChoudharyNo ratings yet
- Congenital Heart DiseaseDocument17 pagesCongenital Heart DiseaseMihraban OmerNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- w4 - Sommerfeld's Model (II)Document21 pagesw4 - Sommerfeld's Model (II)Chairoh IraNo ratings yet
- 44 ZA E InternalDocument13 pages44 ZA E InternalRohit RajNo ratings yet
- 19 Klusakova PDFDocument25 pages19 Klusakova PDFAlaa AmroNo ratings yet
- Ans. 60 Minutes: Maths ProblemsDocument6 pagesAns. 60 Minutes: Maths Problemsapi-3835727No ratings yet
- PROFESSIONAL ServicesDocument22 pagesPROFESSIONAL Serviceshashirali12No ratings yet
- Bangladesh Pharmaceutical Market: Rank Company Value (CR) TK Share GR% Total Pharma Market 8,047.85 100.00 24.63Document2 pagesBangladesh Pharmaceutical Market: Rank Company Value (CR) TK Share GR% Total Pharma Market 8,047.85 100.00 24.63Khadija NafeesNo ratings yet
- Best Practices Desaereator 1 PDFDocument34 pagesBest Practices Desaereator 1 PDFWayne GajadharNo ratings yet
- PST Lesson Plan 9 (Q1-Non Mendelian Inheritance PatternDocument10 pagesPST Lesson Plan 9 (Q1-Non Mendelian Inheritance PatternJeffrey Jr. DanoNo ratings yet
- Opening LetterDocument6 pagesOpening LetterAhmad Fauzi HamdiNo ratings yet
- Software Requirements Specification: Gem ProjectDocument75 pagesSoftware Requirements Specification: Gem ProjectDebanil MajumderNo ratings yet
- Station Operation #: Exhibit 3 Netbook Assembly LineDocument11 pagesStation Operation #: Exhibit 3 Netbook Assembly LineTathagataNo ratings yet
- Battered Women Syndrome As A Legal DefenseDocument7 pagesBattered Women Syndrome As A Legal Defensesir3tanNo ratings yet
- Mr.Dat_E12_U56Document11 pagesMr.Dat_E12_U56Thủy Tiên Nguyễn LêNo ratings yet
- Assignment BEGC103 (July 2024 - Jan 2025) Indian Writing in EnglishDocument4 pagesAssignment BEGC103 (July 2024 - Jan 2025) Indian Writing in Englishmaddy.cyber0No ratings yet
- MAT Minimum Alternate Tax - 8 Marks (A) (I) Basic: Simple Hai !Document3 pagesMAT Minimum Alternate Tax - 8 Marks (A) (I) Basic: Simple Hai !srushti thoratNo ratings yet
- Sacchi Dan andDocument2 pagesSacchi Dan andVINAYNo ratings yet
- E P, P D: Dmond Anariti HDocument6 pagesE P, P D: Dmond Anariti HArisa LicoNo ratings yet
- WDL11 DR B 4104Document1 pageWDL11 DR B 4104vengat.jdwatersNo ratings yet
- Ensayos de George Orwell 1984Document6 pagesEnsayos de George Orwell 1984oppfvxmpd100% (2)
- Final Exam 2010 SolnDocument7 pagesFinal Exam 2010 SolnSimon AlmeidaNo ratings yet
- Regional Variations in Climate and Malaria Transmission in Uganda (WWW - Kiu.ac - Ug)Document5 pagesRegional Variations in Climate and Malaria Transmission in Uganda (WWW - Kiu.ac - Ug)publication1No ratings yet
- Natural Language Processing in Investigative JournalismDocument53 pagesNatural Language Processing in Investigative JournalismJonathan StrayNo ratings yet
- Consortium Tech SheetDocument7 pagesConsortium Tech SheetmehNo ratings yet
- Nino Ivanidze Focus On The Learner New Part 2Document8 pagesNino Ivanidze Focus On The Learner New Part 2Nino Ivanidze0% (1)
- Max 30100Document20 pagesMax 30100Sagor Saha0% (1)