Download as PPT, PDF, TXT or read online from Scribd
Download as ppt, pdf, or txt
You are on page 1/ 35
DR K BEMAUL-SUKHU
Epidemiology • 30 % of adults meet criteria for a diagnosis of hypertension • Seventy-three million Americans are hypertensive • 20 % of hypertensive patients are unaware of their condition • In the US hypertension is the second leading cause of CKD • In 2010, hypertension was said to have caused 32,000 new cases of kidney failure
Source: United States Renal data system, Centre of Disease Control and Prevention More common in blacks, Filipinos, and Native Americans and less in whites and Mexican Americans, rates increase with age, and is greater in the southeastern United States.
Hypertension is more common in men (though menopause tends
to decrease this difference) and in those of low socioeconomic status.
WHO has identified hypertension as the leading cause of
cardiovascular mortality Hypertension (HTN) sometimes called arterial hypertension, is a chronic medical condition in which the blood pressure in the arteries is elevated. Regulation Endogenous regulation of arterial pressure is not completely understood, but the following mechanisms of regulating arterial pressure have been well- characterized: Baroreceptor reflex Baroreceptors (carotid sinuses, aortic arch) detect changes in bp. These send signals to the medulla via the ANS, adjusts the MAP by altering the total peripheral resistance , rate & force of cardiac contractions
Baroreceptors (venae cavae ,pulmonary veins, atria) regulate secretion of
ADH/Vasopressin, renin and aldosterone
Renin-angiotensin system (RAS)
Juxtaglomerular cells sense the decrease in bp and release renin.
Converts angiotensinogen to angiotensin I
Angiotensin I flows in the bloodstream until it reaches the capillaries of the lungs where angiotensin converting enzyme (ACE) acts on it to convert it into angiotensin II.
Angiotensin II vasoconstrictor thus increases bloodflow to the heart and subsequently the preload, ultimately increasing the co. increases in the release of aldosterone from the adrenal glands.
Aldosterone further increases the Na+ and H2O reabsorption in the distal convoluted tubule Decrease in GFR is sensed as a decrease in Na + levels by the macula densa.
increases Na+ reabsorption.
macula densa releases adenosine which causes constriction of the afferent
arterioles. RAS is targeted -ACE inhibitors and ARB.
Aldosterone system -spironolactone, an aldosterone antagonist.
Fluid retention -diuretics; the antihypertensive effect of diuretics is due
to its effect on blood volume. baroreceptor reflex is not targeted in HTN because if blocked, individuals may suffer from orthostatic hypotension & syncopy. HTN is classified as either primary (essential) or secondary hypertension: 90–95% of cases are categorized as "primary HTN" which means high blood pressure with no obvious underlying medical cause. Remaining 5–10% of cases (secondary HTN) are caused by other conditions that affect the kidneys, arteries, heart or endocrine system. Essential Hypertension
•tends to be familial and is likely to be the consequence of an interaction between environmental and genetic factors
Non modifiable risk factors Modifiable risk factors
Age ≥ 55 yrs Sendentary lifestyle Male sex High fat high cholesterol diet FHx of premature CAD Smoking < 55 yrs in men Abdominal obesity < 65 yrs in women Impaired glucose tolerance Dyslipidemia Stress Secondary hypertension
Kidney diseases or endocrine diseases.
Renal artery stenosis- abdominal bruit
Aortic coarctation -decreased bp in the lower extremities and/or delayed or absent femoral arterial pulses. Cushing's syndrome -truncal obesity, glucose intolerance, moon face, a hump of fat behind the neck/shoulder, and purple stretch marks Pheochromocytoma- Labile or paroxysmal HTN, associated headache, palpitations, pallor, sweat Primary Hyperaldosteronism Thyroid disease. Drugs – steroids, oral contraceptives, decongestants Secondary Hypertension Investigate for secondary hypertension in the following situations
Sudden onset of hypertension or worsening in patient > 55yrs
or < 30yrs Serum creatinine increase by more than 30% after starting ACE inhibitor or ARB Hypokalemia of < 3.5 without an obvious cause or < 3.0 with diuretic use Paroxysmal hypertension > 180/110 systolic Hypertension with headaches, sweating or panic attack Hypertension triggered by beta-blockers or micturition Incidentally discovered adrenal mass Severely elevated blood pressure ( 180 / 110—termed malignant or accelerated hypertension) is referred to as a "hypertensive crisis", as blood pressure at this level confers a high risk of complications. People with bp in this range may have no symptoms, but are more likely to report headaches (22% of cases) and dizziness than the general population. May include visual deterioration or SOB due to heart failure or a general feeling of malaise due to RF. Hypertensive emergency: diagnosed when there is evidence of direct damage to one or more organs as a result of severely elevated blood pressure greater than 180/120 mmHg. Encephalopathy-brain swelling and dysfunction, characterized by headaches, AMS. Retinal papilloedema and/or fundal hemorrhages and exudates. Chest pain may indicate heart muscle damage (MI), aortic dissection. Sob, cough, and the expectoration of blood-stained sputum are characteristic signs of pulmonary edem due to LVF AKI and microangiopathic hemolytic anemia . In these situations, rapid reduction of the blood pressure is mandated to stop ongoing organ damage In contrast there is no evidence that blood pressure needs to be lowered rapidly in hypertensive urgencies where there is no evidence of target organ damage and over aggressive reduction of blood pressure is not without risks.
Use of oral medications to lower the BP gradually over 24 to 48h is
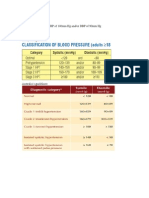
advocated in hypertensive urgencies. Systolic pressure Diastolic pressure JNC7 mmHg mmHg Normal 90–119 60–79
High normal or prehypertensio n 120–139 80–89
Stage 1 140– 90–99 hypertension 159
Stage 2 ≥160 ≥100 hypertension Isolated systolic ≥140 <90 hypertension Signs and symptoms Rarely symptomatic, and its identification is usually through screening. May report headaches (particularly at the back of the head, in the morning), as well as lightheadedness, vertigo, tinnitus (buzzing or hissing in the ears), altered vision or fainting episodes. On physical examination, hypertension may be suspected on the basis of the presence of hypertensive retinopathy Classically, the severity of the hypertensive retinopathy changes is graded from grade I–IV, although the milder types may be difficult to distinguish from each other. Ophthalmoscopy findings may also give some indication as to how long a person has been hypertensive System Tests
Microscopic urinalysis, Renal proteinuria, BUN and/or creatinine Serum sodium, potassium, Endocrine calcium, TSH Fasting blood glucose, Metabolic HDL, LDL, and total cholesterol, triglycerides
blood pressure. Their potential effectiveness is similar to and at times exceeds a single medication. Prevention Lifestyle changes are recommended to lower blood pressure, before starting drug therapy. 2004 British Hypertension Society guidelines/ consistent with those outlined by the US National High BP Education Program in 2002 for the primary prevention of hypertension: body weight for adults (e.g BMI 20–25 kg/m2) Na intake to <100 mmol/ day (<6 g of sodium chloride or <2.4 g of Na/day) regular aerobic physical activity such as brisk walking (≥30 min per day, 4- 7 days/ wk) limit alcohol-< 3 units/day M & < 2 units/day F diet rich in fruit & vegetables (at least 5 portions/ day); A drink is defined:
13.6 g of pure ethanol
44ml or 1.5 oz of 40% proof liquor 12 oz of 355 ml of beer or I glass of wine 148 ml or 5 oz of 12 % wine.
Canadian guidelines suggests a more aggressive approach to Sodium :
< 1200mg for > 70yrs olds 1300mg for 51 – 70 yr olds 1500 mg for ≤ 50yrs DASH diet (Dietary Approaches to Stop Hypertension) nuts, whole grains, fish, poultry, fruits and vegetables lowers blood pressure. A major feature of the plan is limiting intake of sodium, although the diet is also rich in potassium, magnesium, calcium, as well as protein. Programs aimed to reduce psychological stress: yoga, relaxation and other forms of meditation do not appear to reduce blood pressure, and, of the techniques with supportive evidence, there is limited information on whether the modest reduction in blood pressure results in prevention of cardiovascular disease. Several exercise regimes—including isometric resistance exercise, aerobic exercise, resistance exercise and device-guided breathing—may be useful in reducing blood pressure. Benefits of Smoking Cessation
Daytime blood pressure was reduced by about 3.6
mmHg one week after quitting smoking Heart rate decreased by about 7 beats/min after smokers quit for one week The above difference is the effect of quitting and not the same for those who never smoked
Am J Hypertens. 2001 Sep;14(9 Pt 1):942-9.
If drug treatment is initiated JNC-7 recommends that the physician not only monitor for response to treatment but should also assess for any side effects resulting from the medication.
Reduction of the blood pressure by 5 mmHg can decrease the risk of
stroke by 34%, of ischaemic heart disease by 21%, and reduce the likelihood of dementia, heart failure, and mortality from cardiovascular disease The Cochrane collaboration, WHO & US guidelines supports low dose thiazide-based diuretic as first line treatment.
UK guidelines emphasise CCB > 55 yrs /African/Caribbean family origin,
with ACE-I as first line for younger people.
Compared to placebo and other anti-hypertensive drugs as first-line
therapy for hypertension, beta-blockers have greater benefit in stroke reduction. Elderly Tx moderate- severe HTN decreases death rates & cardiovascular morbidity & mortality in 60yrs & older.
Goal as <150/90 mm Hg with thiazide diuretic, CCB, ACEI, or ARB being
the first line medication in the US, & in the revised UK guidelines CCB are advocated as first line with targets of clinic readings <150/90, or <145/85 on ambulatory or home Bp monitoring Medication Therapy
Recommended if systolic BP > 140mmHg or diastolic >
90mmHg with lifestyle modification
Or systolic > 140mmHg & diastolic > 90 mmHg with
target organ damage or diagnosed CAD
DM systolic BP > 130 mmHg & diastolic > 80mmHg
Medication Therapy Isolated systolic HTN and widened pulse pressure (SBP ≥ 160 mmHg and DBP ≤ 70 mmHg)
One or more associated conditions or evidence of end-organ damage
high absolute risk for cardiovascular disease assessed according to clinical
indicators or the risk calculator Specific Agents in Special Patient Populations Getting to Target • Only 30 % would reach target with one agent
• Close to 60% of patients would require 2 or more agents to reach targets
• Combinations of ACE-I with thiazide diuretics preferred
• Avoid combinations of ACE inhibitors & ARBs
• Avoid combination of non-dihydropyridine CCB with BB
Prognosis HTN is the most important, preventable risk factor for premature death worldwide. It increases the risk of IHD, CVA, PVD, and other cardiovascular diseases, including HF, aortic aneurysms, diffuse atherosclerosis, and PE. Risk factor for cognitive impairment, dementia, and CRF. Hypertensive retinopathy and hypertensive nephropathy.