Lower Limb BONES
Lower Limb BONES
Download as pptx, pdf, or txt
You might also like
- Skeletal System Grade 4Document3 pagesSkeletal System Grade 4Joi Ereseht90% (10)
- Upper Limb: Organization FunctionDocument33 pagesUpper Limb: Organization FunctionAhmed Nabiel El-Jaliel100% (1)
- 2.bones of The Lower Limbs PDFDocument14 pages2.bones of The Lower Limbs PDFYahya Alkamali100% (1)
- Muscles of The Upper LimbDocument17 pagesMuscles of The Upper LimbJhanelle S. Dixon-LairdNo ratings yet
- Brachial PlexusDocument98 pagesBrachial PlexussandeepNo ratings yet
- ComplaintDocument6 pagesComplaintCarlos AparicioNo ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Anatomy of The ARMDocument17 pagesAnatomy of The ARMJacob MasikaNo ratings yet
- Femoral Sheath and Femoral TriangleDocument23 pagesFemoral Sheath and Femoral TriangleSamiha Haq100% (2)
- Joints of Lower Limb 2017Document77 pagesJoints of Lower Limb 2017yasrul izadNo ratings yet
- Gluteal RegionDocument34 pagesGluteal Regionlion2chNo ratings yet
- Popliteal Fossa and LegDocument40 pagesPopliteal Fossa and LegRaj Shekhar SinghNo ratings yet
- Hip Joint PDFDocument11 pagesHip Joint PDFStephen Subiera MiayoNo ratings yet
- Femoral Region, Anterior and Medial Compartments of The ThighDocument49 pagesFemoral Region, Anterior and Medial Compartments of The ThighNolanNo ratings yet
- The Shoulder Anatomy & Approaches: Abdulaziz F. Ahmed, MBBS PGY-2Document61 pagesThe Shoulder Anatomy & Approaches: Abdulaziz F. Ahmed, MBBS PGY-2Abdulaziz Al-Akhras100% (1)
- Osteology of The Upper Limb LectureDocument40 pagesOsteology of The Upper Limb LectureFavour OnyeaboNo ratings yet
- A Sole 16 12 14Document51 pagesA Sole 16 12 14Mariam AymanNo ratings yet
- Clinical Anatomy of The Esophagus and StomachDocument82 pagesClinical Anatomy of The Esophagus and StomachmackieccNo ratings yet
- Neck SummaryDocument9 pagesNeck SummaryCarleta StanNo ratings yet
- Triangles of Neck (Anatomy)Document36 pagesTriangles of Neck (Anatomy)Dr Tahira Nihal100% (1)
- Gross Anatomy of Posterior Compartment of The ThighDocument20 pagesGross Anatomy of Posterior Compartment of The ThighOnah ArinzeNo ratings yet
- 3 Shoulder Joint - Chapter Summary - Anatomy of The Shoulder Joint by Snell Medicine LectureDocument76 pages3 Shoulder Joint - Chapter Summary - Anatomy of The Shoulder Joint by Snell Medicine LectureRobin TolentinoNo ratings yet
- Brachial Plexus InjuryDocument20 pagesBrachial Plexus InjurySuci PramadianiNo ratings yet
- Joint of Lower LimbDocument16 pagesJoint of Lower LimbZA ID100% (1)
- Upper LimbDocument31 pagesUpper LimbNandhana Kattuparambil SunojNo ratings yet
- Applied Anatomy of Upper Limb Part OneDocument66 pagesApplied Anatomy of Upper Limb Part Oneprinceej100% (3)
- Upper Limb MnemonicsDocument29 pagesUpper Limb MnemonicsdyaNo ratings yet
- L14-Arteries of The Lower Limb-DoneDocument47 pagesL14-Arteries of The Lower Limb-Doneyakuza444No ratings yet
- 4 AxillaDocument31 pages4 AxillaRamesh KumarNo ratings yet
- 7th Week Femoral Sheath, Femoral Triangle and Adductor CanalDocument17 pages7th Week Femoral Sheath, Femoral Triangle and Adductor CanalShah NawazNo ratings yet
- Popliteal Fossa: Dr.P.Sasikala, Assistant Professor of AnatomyDocument18 pagesPopliteal Fossa: Dr.P.Sasikala, Assistant Professor of AnatomySasikala Mohan100% (1)
- Gluteal Region, Posterior Compartment of The Thigh and Popliteal FossaDocument4 pagesGluteal Region, Posterior Compartment of The Thigh and Popliteal FossaSteph SantosNo ratings yet
- Foot and Ankle Bones and JointsDocument43 pagesFoot and Ankle Bones and Jointshannah murphyNo ratings yet
- Lower Limb Anatomy TablesDocument8 pagesLower Limb Anatomy Tableskep1313No ratings yet
- Anatomy of The LiverDocument25 pagesAnatomy of The Liverapi-354184238100% (1)
- AXILLADocument8 pagesAXILLAImmunity RABOTANo ratings yet
- Radioanatomy of Shoulder Joint-Dr - NaziyaDocument82 pagesRadioanatomy of Shoulder Joint-Dr - Naziyaraghavmaster100% (1)
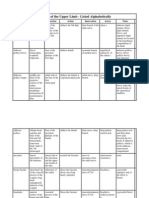
- Topographical Anatomy of The Lower Limb - Listed AlphabeticallyDocument3 pagesTopographical Anatomy of The Lower Limb - Listed AlphabeticallySaba Adde Duhera-HamidovicNo ratings yet
- Colorectal MalignancyDocument108 pagesColorectal MalignancySatishht SatishNo ratings yet
- Bones of Upper and Lower Limbs - RevisionDocument15 pagesBones of Upper and Lower Limbs - RevisionChess Nuts100% (1)
- Anatomy of Upper Limb-1 EDITAN HEMATDocument49 pagesAnatomy of Upper Limb-1 EDITAN HEMATFriska Penri UtamiNo ratings yet
- Gross Anatomy of The Pelvis & Perineum DR Ogedengbe O.ODocument162 pagesGross Anatomy of The Pelvis & Perineum DR Ogedengbe O.OKolawole Adesina KehindeNo ratings yet
- Lower Limb & HipDocument9 pagesLower Limb & HipENo ratings yet
- Anatomi Lower LimbDocument55 pagesAnatomi Lower LimbWagiono SuparanNo ratings yet
- Anterior Triangle of The Neck IIDocument49 pagesAnterior Triangle of The Neck IIvrajNo ratings yet
- Anatomy of ArmDocument22 pagesAnatomy of Armromaisa akhtarNo ratings yet
- General Anatomy of The Human BodyDocument18 pagesGeneral Anatomy of The Human BodyVarenLagartoNo ratings yet
- Hip Complex BioDocument18 pagesHip Complex BioVijay PradeepNo ratings yet
- Muscle Origin Insertion Action Nerve: SartoriusDocument3 pagesMuscle Origin Insertion Action Nerve: SartoriusJim VargheseNo ratings yet
- Elbow Joint & Anastomosis Around Elbow Joint: ObjectivesDocument7 pagesElbow Joint & Anastomosis Around Elbow Joint: Objectiveschittsat39610% (1)
- Tips For Studying MusclesDocument2 pagesTips For Studying Musclesapi-19510625100% (11)
- Popliteal FossaDocument4 pagesPopliteal FossaHassan MohamedNo ratings yet
- Muscles of The BackDocument38 pagesMuscles of The BackPrashanth KumarNo ratings yet
- Sole of The FootDocument51 pagesSole of The FootObinna AdolalomNo ratings yet
- Hip & Thigh MusclesDocument34 pagesHip & Thigh MusclesJeffrey Schrank100% (1)
- Thorax AllDocument174 pagesThorax Allravindra sharmaNo ratings yet
- Femoral TriangleDocument4 pagesFemoral TriangleHassan MohamedNo ratings yet
- Anatomy - NotesDocument149 pagesAnatomy - Noteshusayn12No ratings yet
- Compartment of ThighDocument48 pagesCompartment of Thighhalarajeh2004No ratings yet
- The Shoulder JointDocument17 pagesThe Shoulder JointBhargav100% (1)
- ANKLE JOINT &joints of FootDocument35 pagesANKLE JOINT &joints of Foothhaanniiss3870No ratings yet
- 1 Lower Limb BONESDocument79 pages1 Lower Limb BONESZaid AbdulqadirNo ratings yet
- Maxillary Immediate Denture A Case ReportDocument4 pagesMaxillary Immediate Denture A Case ReportarinazakiyyaNo ratings yet
- HMA GM SheetDocument6 pagesHMA GM SheetdjbartboNo ratings yet
- Accident Incidents Data AnalysisDocument1 pageAccident Incidents Data AnalysissaqibNo ratings yet
- Wide Receiver Route Running Techniques-ClinicDocument18 pagesWide Receiver Route Running Techniques-Clinictgrider100% (1)
- Assessing The Musculoskeletal & Neurological SystemDocument34 pagesAssessing The Musculoskeletal & Neurological SystemalelichengNo ratings yet
- MEESAFE Poor LightingDocument2 pagesMEESAFE Poor LightingRacNo ratings yet
- Low-Level Laser Therapy by Philip OdegardDocument2 pagesLow-Level Laser Therapy by Philip OdegardLinda SwansonNo ratings yet
- Round Star v. Creativity Soccer Stars - SUPER SOCCER STARS Trademark Non-Compete Complaint PDFDocument31 pagesRound Star v. Creativity Soccer Stars - SUPER SOCCER STARS Trademark Non-Compete Complaint PDFMark JaffeNo ratings yet
- Use This Thermometer and Take His Fever/heat/temperatureDocument6 pagesUse This Thermometer and Take His Fever/heat/temperatureRobbyAlivianNo ratings yet
- wk2 FinTypes - of - Traction PDFDocument47 pageswk2 FinTypes - of - Traction PDFclaire yowsNo ratings yet
- When Should I Use Tranexamic Acid For Children?: DR Andrea Kelleher Consultant Adult and Paediatric Cardiac AnaesthetistDocument27 pagesWhen Should I Use Tranexamic Acid For Children?: DR Andrea Kelleher Consultant Adult and Paediatric Cardiac AnaesthetisteyyuninNo ratings yet
- Sports Med Cloze PassageDocument2 pagesSports Med Cloze Passageamacqueen123No ratings yet
- (ARTHREX) - ProStop - (Técnica)Document6 pages(ARTHREX) - ProStop - (Técnica)João Pedro de AguiarNo ratings yet
- Shadowrun Anarchy Narration AidDocument4 pagesShadowrun Anarchy Narration AidDon GuapoNo ratings yet
- Janome 1600P Sewing Machine Instruction ManualDocument23 pagesJanome 1600P Sewing Machine Instruction ManualiliiexpugnansNo ratings yet
- Carpal Instability - 2Document71 pagesCarpal Instability - 2mohammad farhanNo ratings yet
- PE PT 2 Question Paper 12 STDDocument3 pagesPE PT 2 Question Paper 12 STDrenu jhaNo ratings yet
- Driving in Qatar - at A Glance PDFDocument6 pagesDriving in Qatar - at A Glance PDFlinkdanuNo ratings yet
- First Aid, Disaster Management and Emergency SafetyDocument44 pagesFirst Aid, Disaster Management and Emergency SafetyJohn Rey PetalioNo ratings yet
- Child Abuse: Dr. Rasha Salama PHD Community Medicine Suez Canal University EgyptDocument55 pagesChild Abuse: Dr. Rasha Salama PHD Community Medicine Suez Canal University EgyptKhan BahiNo ratings yet
- BLOOD SUPPLY OF LOWER LIMB ReviewsDocument29 pagesBLOOD SUPPLY OF LOWER LIMB ReviewsAdewunmi ToluNo ratings yet
- WREN Hydraulic Torque Wrench Manual - LOWDocument20 pagesWREN Hydraulic Torque Wrench Manual - LOWMohd ZaidNo ratings yet
- Types of DisabilityDocument2 pagesTypes of DisabilityUmraz BabarNo ratings yet
- Day 2 - Back ExamDocument20 pagesDay 2 - Back ExamTingting GeNo ratings yet
- JSA 45 - Valve BoxupDocument18 pagesJSA 45 - Valve BoxupgolusinghdataNo ratings yet
- Sample Nursing ExaminationsDocument58 pagesSample Nursing ExaminationsKars AtacadorNo ratings yet
- Techniques For Moving An Injured or Ill Person PDFDocument3 pagesTechniques For Moving An Injured or Ill Person PDFMonykha Plaza IbarraNo ratings yet
- 2004 Infiniti G35 PDFDocument272 pages2004 Infiniti G35 PDFLakiLakicNo ratings yet