


















Geriatric nursing
- 1. BY: MAMTA PARIHAR MSC. NURSING 1ST YEAR GERIATRIC NURSING
- 2. Robert browning. “Grow old along with me! The best is yet to be”
- 3. INTRODUCTION:- Aging, the normal process of time- related change, begins with birth and continues throughout life. Gerontological nursing is the specialty of nursing pertaining to older adults who work in collaboration with older adults, their families, and communities to support healthy aging, maximum functioning, and quality of life.
- 4. DEFINITIONS: - Geriatrics: the study of old age that includes the physiology, pathology, diagnosis, and management of the disorders and diseases of older adults Gerontology: the combined biologic, psychologic, and
- 5. Gerontology /geriatric nursing: The term gerontological nursing, which replaced the term geriatric nursing in the 1970s, is seen as being more consistent with the specialty's broader focus on health and wellness, in addition to illness. The field of nursing that specializes in the nursing process as it relates to the assessment, nursing diagnosis, planning, implementation, and evaluation of older adults in all environments including acute, intermediate, and skilled care as well as
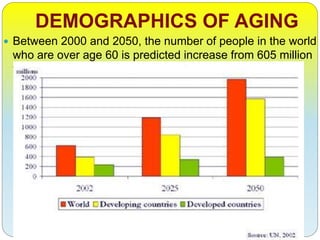
- 6. DEMOGRAPHICS OF AGING Between 2000 and 2050, the number of people in the world who are over age 60 is predicted increase from 605 million to 2 billion.
- 8. These data are showing that: The proportion of older adults is already high and continuing to increase in more developed countries. The share of India’s population ages 60 and older is projected to climb from 8% in 2010 to 19% in 2050, according to the United Nations Population Division (UN 2011). By mid-century, India’s 60 and older population is expected to encompass 323 million people, a number greater than the
- 9. The increasing number of old people is like a challenge and opportunity both……. Aging is a process not a disease……
- 10. FACTORS INFLUENCING AGING Heredity Nutrition Health status Life experiences Environment Activity Stress produce unique
- 11. CHANGES 1. Physiological 2. Psychosocial 3. Cognitive
- 12. PHYSIOLOGICAL CHANGES 1.Cardiovascular system 2.Respiratory Systems 3.Integumentary System 4.Musculoskeletal System 5.Genitourinary Systems 6.Reproductive System 7.Gastrointestinal System 8.Nervous System 9.Special Senses
- 13. PSYCHOSOCIAL CHANGES: Retirement and Social isolation Sexuality Elder neglect Elder abuse Housing and environment Death Stress and Coping in the Older Adult
- 14. COGNITIVE CHANGES Delirium: or an acute confusional state, is a potentially reversible cognitive impairment that is often due to a physiological cause Depression: It is the most common affective or mood disorder of old age and is often responsive to treatment. Its classification and diagnosis vary according to the number, severity, and duration of symptoms. Dementia: Dementia is generalized impairment of intellectual functioning that interferes with social and occupational functioning
- 15. PHARMACOLOGIC ASPECTS OF AGING Absorption: Reduced gastric acid; increased pH (less acid), Reduced gastrointestinal motility; prolonged gastric emptying Distribution: Decreased albumin sites, Reduced cardiac output, Impaired peripheral blood flow, Increased percentage of body fat, Decreased lean body mass Metabolism: Decreased cardiac output and decreased, perfusion of the liver Excretion: Decreased renal blood flow; loss of
- 16. THE COMMON AGE RELATED PROBLEMS Osteoarthritis Osteoporosis Cardiovascular disease Alzheimer‘s Diabetes
- 18. MYTH: FACT: Most older people are pretty much alike. They are a very diverse age group. They are generally alone and lonely. Most older adults maintain close contact with family. They are sick, frail, and dependent on others. Most older people live independently. They are often cognitively impaired For most older adults, if there is decline in some intellectual abilities, it is not severe enough to cause problems in daily living. They are depressed. Community dwelling older adults have lower rates of diagnosable depression than younger adults. They become more difficult and rigid with advancing years. Personality remains relatively consistent throughout the lifespan. They barely cope with the inevitable declines associated with aging. Most older people successfully adjust to the challenges of aging. AGING: MYTH VS. FACT
- 19. DEVELOPMENT OF GERONTOLOGICAL NURSING 1950- 1st Gerontological nursing text published, Geriatrics recognized as an area of specialization in nursing. 1961- ANA recommends specialty group for geriatric nurses. 1966- Formation of geriatric nursing division of ANA 1969- Development of standards for geriatric nursing practice
- 20. Cont…. 1976- ANA changes name from Geriatric Nursing division to Gerontological nursing division. 1981- First international conference on Gerontological nursing. 1982- Development of Robert Wood Johnson teaching Home Nursing Program. 1984- Formation of National Gerontological Nursing Association.
- 21. SCOPE Gerontological nurses work in a variety of settings, including acute care hospitals, rehabilitation, nursing homes (also known as long term care homes and skilled nursing facilities), assisted living facilities, retirement homes, community health agencies, and the patient's
- 22. TRAINING AND EDUCATION Gerontological nursing includes generalist and specialist practice. National nursing organizations such as the American Nurses Credentialing Center, the Canadian Nurses Association offer certification in gerontological nursing. In order to be certified, the nurse must have a minimum academic preparation, experience as a
- 23. Developmental Theories of aging Acc to Erikson (1963) theorized that a person’s life consists of eight stages, Each stage representing a crucial turning point in the life span stretching from birth to death with its own developmental conflict to be resolved. According to Erikson, the major developmental task of old age is to either achieve ego integrity or suffer despair. Achieving ego integrity requires accepting one’s lifestyle, believing that one’s choices were the best that could be made at a particular time, and being in control of one’s life. Despair results when an older person feels dissatisfied and disappointed with his or her life, and would live differently if given another chance.
- 24. Cont…. Havighurst (1972) also suggested a list of developmental tasksbthat occur during a lifetime. The tasks of the older person includebadjusting to retirement after a lifetime of employment with a possible reduction of income, decreases in physical strength and health, the death of a spouse, establishing affiliation with one’s age group, adapting to new social roles in a flexible way, and establishing satisfactory physical living arrangements.
- 25. Cont… Combining the concepts of both Erikson and Havighurst suggests the following developmental tasks for the older adult: (1) Maintenance Of Self-worth, (2) Conflict Resolution, (3) Adjustment To The Loss Of Dominant Roles, (4) Adjustment To The Deaths Of Significant Others, (5) Environmental Adaptation, And (6) Maintenance Of Optimal Levels Of Wellness.
- 26. PRINCIPLES OF GERONTOLOGICAL NURSING PRACTICE Aging is a natural process common to all living organisms. Various factors influence the aging process. Unique data and knowledge are used in applying the nursing process to the older populations. The elderly share similar self-care and human needs with all other human beings. Gerontological nursing strives to help older adults achieve optimum levels of physical, psychological, social and spiritual and
- 27. Ana standards of gerontological nursing practice (nursing care) I. Assessment II. Diagnosis III. Outcome identification IV. Planning V. Implementations VI. Evaluation VII. Research VIII. Resource Utilization
- 28. Life Care Plans for older adults Evaluation of the older ADLs Complete history Family issues Vocational/educational history Projected physical and occupational therapy needs Future medical care Personal items Diagnostic testing Medical equipment and supply needs Recreational equipment
- 29. ROLE OF DIFFERENTE AGENCIES The Role of the Family Community Support Services Home Health Care Safety and Comfort in the Home Environment Hospice Services
- 31. HEALER Overcome or cope with disease restore function and purpose in life and mobilize internal and external resources. Recognizes that most human beings value health, are responsible and active participants in their health maintenance and illness management, and desires harmony and wholeness with their environment. Holistic approach is essential viewed in context of their biological, emotional, social, cultural and spiritual
- 32. CAREGIVER Conscientious application of Nursing process to care of elders. Inherent in this role is the active participation of older adults and their significant others and promotion of highest degree of self care in elderly. Providing care, efficiency and best interest that rob them of their existing
- 33. EDUCATOR Formal and informal opportunities to share knowledge, skills related to care of older adults. Educating others including normal aging, pathophysiology, geriatric pharmacology and resources. Essential to this role is effective communication involving listening, interacting, clarifying, coaching, validating and evaluating.
- 34. ADVOCATE Advocacy including aiding older adults in asserting their rights and obtaining required services, facilitating a community or other group’s effort to affect change and achieve benefits for older adults.
- 35. INNOVATOR Assumes an inquisitive style, making conscious decisions and efforts to experiment for an end result to improved gerontological practices.
- 38. SUMMARY GERIATIC NURSING: it is the field of nursing that specializes in the care of the elderly. Older people have increasingly been the focus of health and social care policy. Health and social care policy impacts significantly on older people, and in particular on their continuing care needs. Changes in the boundaries of health provision and pressures for cost containment have profoundly affected older people as well as service providers.