Estimating risk
•Download as PPTX, PDF•
18 likes•6,028 views

This document provides definitions and examples of key concepts for estimating risk from epidemiological studies, including probability, odds, relative risk, and absolute risk. It discusses how relative risk is calculated from cohort and case-control study designs. Relative risk compares the risk of an outcome between exposed and unexposed groups to determine if exposure is associated with increased risk. The odds ratio, which estimates relative risk, is presented as the measure used to assess association in case-control studies. Examples are provided to demonstrate calculating and interpreting these risk measures.
Report
Share














































Estimating risk
- 1. Estimating Risk Dr. Tarek Tawfik Amin 12/18/2013 Dr. Tarek Tawfik
- 2. Objectives • By the end of this session, attendees should be able to: 1- Differentiate between probability, Odd, and risk with it variants. 2- Recall the basics for calculating Odds and relative risk and interpret the results. 3- Define the indications of applying the risk parameters.
- 3. Definitions of terms: Probability, risk and Odd • Probability: Is the proportion (%) of times an event would occur if an observation was repeated many times. • Risk: Is the probability of an event among those experiencing the event divided by the number who could experience it (at risk). • Odds: Probability of an event divided by the probability of the event not happening.
- 4. Probability Proportion (%) 0-1 (100%) The 10 year probability of OP hip fracture among those aged 70 years is 0.23 (23%). Odds (chance) Risk Ratio Probability/(1probaility) 0 to infinity The Odds for OP hip fracture is 0.23/(1.0.23)=0.30 Ratio (rate) 0 to infinity No denominator Denominator Incidence of OP hip fracture among those aged 70 years. Attack rate is an other example
- 5. Risk
- 6. A-Absolute Risk The incidence of a disease in a population is termed absolute risk. Can indicate the magnitude of risk in a group of people with a certain exposure, but: It does not take into consideration the risk of disease in the nonexposed individuals, It does not indicate whether the exposure is associated with an increased risk of disease. Absolute risk doe not stipulate an explicit comparison. Rubella in 1st trimester: what is the risk that my child will be malformed? Abortion will be decided on the basis of this information. 12/18/2013 Dr. Tarek Tawfik
- 7. B-Relative risk: Determination that a certain disease is associated with a certain exposure. By using the (case-control) and cohort studies we can assess whether there is an excess risk of disease in persons who have been exposed. Comparing different risks among different groups to assess the presence of excessive risk (the incidence rate „attack rates‟ and the difference in the risks). Estimation of relative risks are vital in determining who will be at a higher risk following the exposure. 12/18/2013 Dr. Tarek Tawfik
- 8. Relative Risk (concept) o Case-control and cohort studies are designed to determine whether there is an association between exposure to a factor and development of a disease. If an association exists, how strong is it? o In cohort study: what is the ratio of the risk of disease in exposed individuals to the risk of disease in nonexposed individuals? (RR=relative risk). Risk in exposed (incidence in the exposed) Relative risk (RR) = Risk in non-exposed (incidence in the non-exposed)
- 9. Basic Structure of cohort study Diseased Disease-free The Relative Risk is calculated for exposure Develop Disease (a) Sample Exposed to factor Develop Disease (c) Diseasefree Unexposed to factor Disease-free (d) Future time Present time Starting point Disease-free (b) Follow Comparing the incidence of disease in each group Population
- 10. Basic structure of case-control design Population Diseased Unexposed to factor (b) Diseased (cases) Sample The Odds “chance of exposure Is calculated between both groups Exposed to factor (a) Disease-free Exposed to factor (c) Disease-free (controls) Unexposed to factor (d) Trace Past time Present time Starting point
- 11. The following table depicts the outcomes of isoniazid/placebo trial among children with HIV (death within 6 months). What is the risk of dying? Interventions Dead (within Alive Total 6 months) Placebo 21 110 131 Risk=21/131=0.160 Isoniazid 11 121 132 Risk=11/132=0.083 Absolute risk difference (ARD)=risk in placebo-risk in isoniazid= 0.077 Net relative risk (NRR)=risk in placebo/risk in isoniazid= 1.928 Relative risk reduction (RRR)=risk in placebo-risk in isoniazid/risk in placebo= 0.48 Number needed to treat (NNT)=1/ARD=1/0.077=13
- 12. Relative risk (RR) Mammography Breast cancer No breast cancer Total Positive a-10 b-90 100 Negative c-20 d-998980 100,100 In Cohort design RR= a/(a+b)÷c/(c+d) 10/(100) ÷20(100,100)=0.1/0.0002= 500
- 13. The relative risk (RR) Lung cancer Smokers Non 18 6 No lung cancer 582 1194 Risk for smokers=18/600=0.03 Risk for non-smokers=6/1200=0.005 RR=0.03/0.005=6 Total 600 1200
- 14. Interpreting the Relative Risk (measure the strength of the association) If RR = 1 If RR > 1 If RR < 1 Risk in exposed equal to risk in nonexposed (no association). Risk in exposed greater than risk in nonexposed (positive association; possibly causal). Risk in exposed less than risk in nonexposed (negative association; possibly protective).
- 15. Calculating the Relative Risk in Cohort Studies Then follow to see whether Disease develops a First select a+b b c d Totals a+b Incidence rate of disease a a+b Exposed No exposed a Disease does not develop = incidence in exposed c c+d c+d c c+d = incidence in non-exposed
- 16. Hypothetical Cohort 3,000 smokers and 5,000 non-smokers to investigate the relation of smoking to the development of coronary heart disease (CHD) over a 1-year period. Develop CHD Do not develop CHD Totals Incidence per 1,000/year Smoke cigarettes 84 2,916 3,000 28.0 Do not smoke cigarettes 87 4,913 5,000 17.4 Incidence among the exposed= 84/3,000 = 28.0 per 1,000 Relative risk = Incidence in exposed Incidence in non-exposed = Incidence among the non-exposed = 87/5000 =17.4 per 1,000 28.0/17.4 = 1.61
- 17. Example: the British Heart Study A large cohort study of 7735 men aged 40-59 years randomly selected from general practices in 24 British towns, with the aim of identifying risk factors for ischemic heart disease. At recruitment to the study, the men were asked about a number of demographic and lifestyle, including information on cigarette smoking habits. Of the 7718 men who provided information on smoking status, 5899 (76.4 %) had smoked at some stage during their lives (including those who were current smokers and those who were ex-smokers). Over subsequent 10 years, 650 of these 7718 men (8.4 %) had a myocardial infarction (MI). 12/18/2013 Dr. Tarek Tawfik
- 18. MI in subsequent 10 years Yes No Total Ever smoked 563 (9.5%) 5336 (90.5%) 5899 Never smoked 87 (4.8%) 1732 (95.2%) 1819 Total 650 (8.4%) 7068(71.6%) 7718 Smoking status at baseline The estimated relative risk= (563/5899) (87/1819) = 2.00 CI = 1.60-2.49 (does not include 1) The middle aged man who has ever smoke is twice as likely to suffer a MI over the next 10 years period as a man who has never smoked.
- 19. Odds ratio
- 20. The Odds ratio (relative odds) In order to calculate a relative risk, we must have values for the incidence in the exposed and non-exposed, as can be obtained in the cohort study. In a case-control study, however, we do not know the incidence in the exposed population or the incidence in the non-exposed population because we start with diseased people (cases) and non-diseased people (controls). Hence, we can not estimate the RR in case-control study directly and we implement another measure of association called Odds ratio.
- 21. Defining the Odds ratio in Cohort and Case-control studies. Suppose we betting on a horse named Little Beauty, which has a 60% probability of wining the race (P). Little Beauty, therefore has a 40 % probability of losing (1-P). What are the odds that the horse will win the race? The odds is defined as: the ratio of the number of ways the event can occur to the number of ways the event can not occur. Probability that Little Beauty will win the race Odds = Probability that Little Beauty will lose the race Odds = P/(1-P) or 60 %/40 % = 1.5:1 = 1.5 Probability of wining is 60 %, while the odds (chance) of wining is 1.5 times. 12/18/2013 Dr. Tarek Tawfik
- 22. Odds ratio (OR) o An odds ratio (OR) is a measure of association between an exposure and an outcome. o The OR represents the odds that an outcome will occur given a particular exposure, compared to the odds of the outcome occurring in the absence of that exposure. o Odds ratios are most commonly used in casecontrol studies, however they can also be used in cross-sectional and cohort study designs as well (with some modifications and/or assumptions).
- 23. OR • • • • Rare disease assumption (prevalence < 10%). Case control-design Regression analysis Meta-analysis
- 24. Calculation Case control study Exposed Non-exposed Diseased None Total Cases+ exposed (a) Exposed+ not diseased (b) a+b Cases-not exposed (c) Not exposed+ not diseased (d) c+d Odds ratio= a/c÷b/d= ad/bc Prevalence among the diseased/prevalence among the non-diseased OR=1 Exposure does not affect odds of outcome OR>1 Exposure associated with higher odds of outcome OR<1 Exposure associated with lower odds of outcome
- 25. Odds ratio Case control study Lung cancer No lung cancer Total Smoking a-80 b-30 110 None c-20 d-70 90 80x70=5600 30x20=600 5600/600=9.3 Or 80/20÷30/70=9.3
- 26. The Odds ratio (OR) Lung cancer Smokers Non 80 20 No lung cancer 30 70 Odds for smokers=80/30=2.67 Odds for non-smokers=20/70=0.29 OR=80*70/30*20=9.33 Total 110 90
- 27. Odds Ratios in Case-Control and Cohort Studies Cohort Exposed Not exposed Develop disease Do not develop disease a c Odds ratio= Odds that an exposed person Develops disease Odds that a non-exposed Person develops disease = a/b c/d = ad bc b d Case-control Cases Controls History of exposure a b No history of exposure c d Odds ratio = Odds that a case was exposed Odds that a control was exposed = a/c b/d = ad bc
- 28. Example: HRT A total of 1327 women aged 50 to 81 years with hip fractures, who lived in a largely urban area in Sweden, were investigated in this un-matched case-controls study. They were compared with 3262 controls within the same age range selected from the National register. Interest was centered on determining whether postmenopausal hormone replacement therapy (HRT) substantially reduced the risk of hip fracture. The results in the table show the number of women who were current users of HRT and those who had never used or formerly used HRT in cases and controls.
- 29. Current users of HRT Never used HRT/ former user of HRT Total With hip fracture (cases) 40 (14%) 1287 (30%) 1327 Without hip fracture (controls) 239 3023 3262 Total 279 4310 4589 The observed Odds ratio = (40X3023) (239X1287) =0.39 C.I = 0.28 to 0.56 A postmenopausal woman in this age range in Sweden who was a current user of HRT thus had 39 % of the risk of hip fracture of a woman who had never used or formerly used HRT Being current user of HRT reduced the risk of hip fracture by 61%.
- 30. When is the Odds Ratio a Good Estimate of the Relative Risk? In case-control, only the odds ratio can be calculated as a measure of association, whereas in a cohort, either the relative risk or the odds ratio is a valid measure of association. Nevertheless, estimate of RR can be used in interpreting casecontrol study in the following occasions: When the cases are representative, with regard to history of exposure, of all people with disease in the population from which the cases are drawn. When the controls are representative with regard to history of exposure, of all people without the disease in the population from which the cases were drawn. When the disease being studied dose not occur frequently.
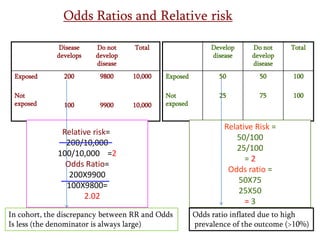
- 31. Odds Ratios and Relative risk Disease develops Exposed Not exposed Do not develop disease Total 200 9800 10,000 10,000 100 9900 Develop disease Do not develop disease Total Exposed 50 50 100 Not exposed 25 75 100 Relative risk= 200/10,000 100/10,000 =2 Odds Ratio= 200X9900 100X9800= 2.02 In cohort, the discrepancy between RR and Odds Is less (the denominator is always large) Relative Risk = 50/100 25/100 =2 Odds ratio = 50X75 25X50 =3 Odds ratio inflated due to high prevalence of the outcome (>10%)
- 33. Remember The relative odds (odds ratio) is a useful measure of association in both case-control and prospective studies “Cohort”. In a cohort study, the relative risk can be calculated directly. In a case-control study, the relative risk cannot be calculated directly, so that the relative odds or odds ratio (cross-product ratio) is used as an estimate of the relative risk when the risk of the disease is low. 12/18/2013 Dr. Tarek Tawfik
- 34. Calculating the Odds ratio in a Matched Pairs CaseControl Study. According to the type of exposure, case-control study can be classified into four groups: - pairs in which both cases and controls were exposed. Concordant pairs - pairs in which neither the cases nor the controls were exposed. - pairs in which the case was exposed but the control was not. Discordant pairs - pairs in which the control was exposed and the case was not. 12/18/2013 Dr. Tarek Tawfik
- 35. 2X2 table Control Cases Exposed Not exposed Exposed a Both the case and control were exposed b The case was exposed and the control was not Not exposed c The case was not exposed and the control was exposed d Neither the case nor the control was exposed Calculation entail the discordant pairs only (b and c), we ignore the concordant pairs, because they do not contribute to our knowledge of how cases and controls differ in regard to past history of exposure. The odds ratio will then equals = b /c
- 36. Case-control study of brain tumors in children. o A number of studies have suggested that children with higher birth weights are at increased risk for childhood cancer. o In the next analysis, exposure is defined as birth weight greater than 8 lbs. Normal control Cases 8+ lbs < 8lbs 8+ lbs 8 18 26 < 8 lbs 7 38 45 Total 15 56 71 Odds ratio = 18/7 = 2.57 2= 4.00 P = 0.046 12/18/2013 Total Dr. Tarek Tawfik
- 37. Attributable Risk How much of the disease that occurs can be attributed to a certain exposure? Attributable risk is defined as the amount or proportion of disease incidence (or disease risk) that can be attributed to a specific exposure. How much of lung cancer risk experienced by smokers can be attributed to smoking? More important than RR as it addresses important clinical practice and public health. How much of the risk (incidence) of disease can we hope to prevent if we are able to eliminate exposure to the agent in question? 12/18/2013 Dr. Tarek Tawfik
- 38. Attributable Risk for the Exposed Group Level of risk 12/18/2013 Exposed Group Background risk In non Exposed group Dr. Tarek Tawfik
- 39. Incidence due to exposure Incidence not due to exposure In exposed group In the nonexposed group
- 40. Calculations The incidence of a disease that is attributable to the exposure in the exposed group can be calculated as follow: (incidence in the exposed group) - (incidence in the non-exposed group) Then, what proportion of the risk in exposed persons is due to the exposure? (incidence in the exposed group) - (incidence in the non-exposed group) incidence in the exposed group 12/18/2013 Dr. Tarek Tawfik
- 41. Attributable Risk for the Total Population What proportion of the disease incidence in a total population (both exposed and non-exposed) can be attributable to a specific exposure? What would be the total impact of a prevention program on the community? Calculations entail: (Incidence in the total population) – (incidence in non-exposed group „background risk‟). In proportion: (Incidence in the total population) – (incidence in non-exposed group „background risk‟). Incidence in total population 12/18/2013 Dr. Tarek Tawfik
- 42. Example for calculating the attributable risk in the exposed group Smoking status Develop CHD Do not develop CHD Total Incidence per 1,000 per year Smoke cigarettes 84 2,916 3,000 28.0 Do not smoke cigarettes 87 4,913 5,000 17.4 Incidence among smokers = 84/3,000 = 28.0 per 1,000 Incidence among non smokers = 87/5,000 = 17.4 per 1,000 The AR = (incidence in exposed group) – (incidence in the non exposed group) = 28.0 – 17.4 /1,000 = 10.6 /1,000???? In proportion = The AR = (incidence in exposed group) – (incidence in the non exposed group) /( incidence in exposed group) = 28.0 – 17.6/ 28.0 = 10.6/28.0 = 0.379 = 37.9 %?????
- 43. What does this mean? The attributable risk = 10.6 /1,000, it means that 10.6 of the 28.0/1,000 incident cases in smokers are attributable to the fact that these people smoke. Thus if we had an effective smoking cessation campaign, we could prevent 10.6 of the 28/1,000 incident cases of CHD that smokers experience. In proportion, 37.9 % of the morbidity from CHD among smokers may be attributable to smoking and could presumably be prevented by eliminating smoking. 12/18/2013 Dr. Tarek Tawfik
- 44. Attributable risk in total population The incidence in the total population can be calculated by subtracting the background risk. (incidence in the total population) – (incidence in the non-exposed group), for calculation we must know the incidence of the disease in the total population (which we often do not know), or all of the following three values, from which we can then calculate the incidence in the total population: The incidence among exposed. The incidence among the non-exposed. The proportion of the total population that exposed (frequently assumed or judged). 12/18/2013 Dr. Tarek Tawfik
- 45. AR in total population. Assuming that the incidence in the total population of smoking is 44% (and therefore the proportion of non-smokers is 56%). The incidence in the total population can then be calculated as follows: (incidence in smokers)(% of smokers in the population) + (incidence in non-smokers)(% of non-smokers in population). = (28.0/1,000)(0.44)+(17.4/1,000)(0.56)= 22.1/1,000 Then the AR= 22.1/1,000 – 17.4/1,000 = 4.7/1,000. It means that, if we an effective prevention program, how much reduction in the incidence of the CHD could be anticipated. 12/18/2013 Dr. Tarek Tawfik
- 46. AR in total population Proportion of incidence in the total population = (incidence in the total population) – (incidence in the nonexposed group)/ incidence in the total population = 22.117.4/22.1= 21.3%. Thus, 21.3 % of the incidence of CHD in this total population can be attributed to smoking, and if an effective prevention program eliminated smoking, the best we could hope to achieve would be a reduction of 21.3 % in the incidence of CHD in the total population which consisting of both smoking and non-smoking. 12/18/2013 Dr. Tarek Tawfik
- 47. Thank you