Exercise for impaired balance by DR. H.Bilal Malakandi, PT
•Download as PPTX, PDF•
102 likes•17,271 views

Introduction to Balance and its concepts, Impaired balance and then management of impaired balance. Based on Therapeutic Exercise Foundations and Techniques
Report
Share
















































































Exercise for impaired balance by DR. H.Bilal Malakandi, PT
- 1. Exercise for Impaired Balance Chapter 8 Therapeutic Exercise Foundations and Techniques Prepared by: Dr. Hazrat Bilal Malakandi, PT DPT (IPMR, KMU), MSPT (KMU), CHPE (KMU)
- 3. Objectives of the lecture • At the end of the lecture students will be able to – Define balance and other key terms – Describe limits of stability and its boundaries – Describe the process of balance control – Describe different sensory systems – Define and describe sensory organization for balance control – Define different types of balance control – Describe motor strategies for balance control
- 4. – Describe impaired balance and its causes – Describe deficits with aging – Enlist risk factors for falls in elders – Perform examination and evaluation of impaired balance – Describe exercise for static balance control, dynamic balance control, anticipatory balance control, reactive balance control and balance during functional activities – Describe different factors affecting balance – Describe Tai Chi for balance control
- 6. Balance and key terms definitions • Balance – Balance, or postural stability, is a generic term used to describe the dynamic process by which the body’s position is maintained in equilibrium. – Equilibrium means that the body is either at rest (static equilibrium) or in steady-state motion (dynamic equilibrium). – Balance is greatest when the body’s center of mass (COM) or center of gravity (COG) is maintained over its base of support (BOS).
- 7. • Center of mass – The COM is a point that corresponds to the center of the total body mass and is the point where the body is in perfect equilibrium. • Center of gravity – The COG refers to the vertical projection of the center of mass to the ground. – In the anatomical position, the COG of most adult humans is located slightly anterior to the second sacral vertebra or approximately 55% of a person’s height.
- 9. • Momentum – Momentum is the product of mass times velocity. – Linear momentum relates to the velocity of the body along a straight path. – Angular momentum relates to the rotational velocity of the body. • Base of support – The BOS is defined as the perimeter of the contact area between the body and its support surface; foot placement alters the BOS and changes a person’s postural stability.
- 10. • Limits of stability – “Limits of stability” refers to the sway boundaries in which an individual can maintain equilibrium without changing his or her BOS – Changing depending on the tasks – For normal adults, the anteroposterior sway limit is approximately 12⁰ from the most posterior to most anterior position. – Lateral stability varies with foot spacing and height; adults standing with 4 inches between the feet can sway approximately 16⁰ from side to side.
- 11. Boundaries of the limits of stability while standing, walking, and sitting.
- 12. • Ground reaction force – the contact between our bodies and the ground due to gravity (action forces) is always accompanied by a reaction from it, the so-called ground reaction force. • Center of pressure – The center of pressure (COP) is the location of the vertical projection of the ground reaction force. – It is equal and opposite to the weighted average of all the downward forces acting on the area in contact with the ground. – COP is a reflection of the body’s neuromuscular responses to imbalances of the COG.
- 13. Balance Control • Balance is a complex motor control task involving – the detection and integration of sensory information to assess • the position and motion of the body in space and • the execution of appropriate musculoskeletal responses to control body position within the context of the environment and task. • Balance control requires the interaction of the nervous and musculoskeletal systems and contextual effects
- 14. Interactions of the musculoskeletal and nervous systems and contextual effects for balance control
- 15. Sensory Systems and Balance Control • Visual System • Somatosensory system • Vestibular system
- 16. Visual System • The visual system provides information regarding 1) the position of the head relative to the environment 2) the orientation of the head to maintain level gaze 3) the direction and speed of head movements because as your head moves, surrounding objects move in the opposite direction.
- 17. • Visual stimuli can be used to improve a person’s stability when – proprioceptive or vestibular inputs are unreliable by fixating the gaze on an object. • Conversely, visual inputs sometimes provide inaccurate information for balance control, such as – when a person is stationary and a large object such as a nearby bus starts moving, causing the person to have an illusion of movement.
- 18. Somatosensory System • The somatosensory system provides information about the – position and motion of the body parts relative to • each other • support surface. • Information from mechanoreceptors are the dominant inputs for maintaining balance when support surface is firm, flat and fixed •
- 19. Mechanoreceptors – Muscle spindles and Golgi tendon organs • sensitive to muscle length and tension – Joint receptors • sensitive to joint position, movement and stress – Skin mechanoreceptors • sensitive to vibration, light touch, deep pressure, skin stretch
- 21. Vestibular System • The vestibular system provides information – about the position and movement of the head – with respect to gravity and inertial forces. • Receptors in the semicircular canals (SCCs) – detect angular acceleration of the head – Sensitive to fast head movements • Receptors in the otoliths (utricle and saccule) – detect linear acceleration and head position with respect to gravity – Responds to slow head movements
- 22. • The vestibular system can give no information about the position of the body. • The vestibular system uses motor pathways – originating from the vestibular nuclei for • postural control and • coordination of eye and head movements.
- 23. Sensory Organization for Balance Control • Somatosensory information has the fastest processing time for rapid responses – followed by visual and vestibular inputs • When sensory inputs from one system are inaccurate owing to environmental conditions or injuries – that decrease the information-processing rate – the CNS must suppress the inaccurate input and – select and combine the appropriate sensory inputs from the other two systems. • This adaptive process is called sensory organization.
- 24. Types of Balance Control • Static balance control – to maintain a stable antigravity position while at rest such as when standing and sitting • Dynamic balance control – to stabilize the body • when the support surface is moving or • when the body is moving on a stable surface – such as sit-to-stand transfers or walking • Automatic postural reactions – to maintain balance in response to unexpected external perturbations, • such as standing on a bus that suddenly accelerates forward
- 25. • Feedforward, or open loop motor control – Utilized for movements that occur too fast to rely on sensory feedback • Anticipatory control – Involves activation of postural muscles in advance of performing skilled movements • Closed loop control – utilized for precision movements that require sensory feedback – e.g., maintaining balance while sitting on a ball or standing on a balance beam
- 26. Movement systems
- 28. Motor Strategies for Balance Control • Three strategies – Ankle Strategy (Anteroposterior Plane) – Hip Strategy – Stepping Strategy
- 29. Ankle Strategy (Anteroposterior Plane) • In quiet stance and during small perturbations movements at the ankle act to – restore a person’s COM to a stable position. • For small external perturbations that cause loss of balance in a forward direction – muscle activation usually proceeds in a distal to proximal sequence – i.e. activation begins in gastrocnemius followed by the hamstrings and finally paraspinal muscle.
- 30. • In response to backward instability – muscle activity begins in the anterior tibialis – followed by the quadriceps and abdominal muscles.
- 31. Hip Strategy • Hip strategy is employed for – rapid and/or large external perturbations – movements executed with the COG near the limits of stability • The hip strategy uses rapid hip flx or ext – to move the COM within the BOS.
- 32. • In response to a forward body sway – muscles are typically activated in a proximal to distal sequence • Abdominals followed by activation of the quadriceps. • Backward body sway results in – activation first of the paraspinals followed by the hamstrings.
- 33. Stepping Strategy • If a large force displaces the COM beyond the limits of stability – a forward or backward step is used to enlarge the BOS and regain balance control • Example of a stepping strategy – The uncoordinated step that follows a stumble on uneven ground
- 34. Ankle, hip, and stepping strategies used by adults to control body sway.
- 35. Factors Influencing Selection of Balance Strategies • Speed and intensity of the displacing forces • Characteristics of the support surface • Magnitude of the displacement of the COM • Subject’s awareness of the disturbance • Subject’s posture at the time of perturbation • Subject’s prior experiences
- 37. Impaired balance
- 38. Impaired balance • Impaired balance can be caused by injury or disease to any structures involved in the three stages of information processing. i.e. – sensory input – sensorimotor integration – motor output generation
- 39. • Sensory input – Proprioceptive deficits have been implicated as contributing to balance impairments following lower extremity and trunk injuries or pathologies – Decreased joint position sense has been reported in individuals with • recurrent ankle sprains • knee ligamentous injuries • degenerative joint disease • low back pain.
- 40. – It is unclear whether decreased joint position sense is due to changes in • joint receptors or in • muscle receptors. – Somatosensory, visual, or vestibular deficits may impair balance and mobility. – Reduced somatosensation in the lower extremities caused by • peripheral polyneuropathies – in the aged and in individuals with diabetes are associated with » balance deficits » an increased risk for falls
- 41. • Visual loss or specific deficits in acuity, contrast sensitivity, peripheral field vision, and depth perception caused by disease, trauma, or aging can impair balance and lead to falls.
- 42. – Individuals with damage to the vestibular system due to viral infections, traumatic brain injury (TBI), or aging may experience • vertigo (a feeling of spinning) and • postural instability. – Patients with severe bilateral loss of vestibular function are unable to use hip strategies, although ankle strategies are unaffected
- 44. • Sensorimotor Integration –Damage to the basal ganglia, cerebellum, or supplementary motor area • impair processing of incoming sensory information • resulting in difficulty adapting sensory information in response to environmental changes.
- 45. –When stance is perturbed by platform translations, patients with • Parkinson’s disease tend to have a smaller than normal amplitude of movement due to co-activation of muscles on both sides of the body, • cerebellar lesions typically demonstrate larger response amplitudes
- 46. • Biomechanical and Motor Output Deficits – Deficits in the motor components of balance control can be caused by • Musculoskeletal – Poor posture, joint ROM limitations, decreased muscle performance • Neuromuscular system impairments – impaired motor coordination, pain
- 47. – Postural malalignment • such as the typical thoracic kyphosis of the elderly, that shifts the COM away from the center of the BOS • increases a person’s chance of exceeding his or her limits of stability – Impaired ROM or muscle strength at one joint can alter posture and balance movements throughout the entire limb.
- 48. – In individuals with neurological conditions (e.g., stroke, traumatic brain injury, Parkinson’s disease) • failure to generate adequate muscle forces due to – abnormal tone – impaired coordination of motor strategies • may limit the person’s ability to recruit muscles required for balance.
- 49. Deficits with Aging • In persons over age 65, falls are common and are a major cause of – morbidity – mortality – reduced functioning – premature nursing home admissions. • Declines are found with aging in all – sensory systems • somatosensory, vision, vestibular – three stages of information processing • sensory processing, sensorimotor integration, motor output
- 53. Examination and Evaluation of Impaired Balance • The key elements include the following – A thorough SE & OE – History of falls – Assessments to identify different impairments contributing to balance deficits • sensory input, sensory processing, biomechanical and motor – Assessment of Eye and Head Movement Functions – Assessment of Cerebellar Function – Assessment of Walking Function
- 54. – Tests and observations to determine the impact of balance control system deficits on functional performance – Environmental assessments to determine fall risk hazards in a person’s home
- 55. Balance training • Static balance control • Reactive balance control • Sensory organization • Balance during functional activities
- 56. Static balance control • Activities to promote static balance control include – sitting, half-kneeling, tall kneeling, and standing postures on a firm surface. • More challenging activities include practice in the tandem and single-leg stance.
- 57. • Progress these activities by – working on soft surfaces (e.g., foam, sand, grass) – narrowing the base of support – moving the arms – closing the eyes
- 59. Provide resistance via handheld weights or elastic resistance.
- 61. Add a secondary task to further increase the level of difficulty
- 62. Dynamic balance control • To promote dynamic balance control, interventions may involve the following. – Maintain equal weight distribution and upright trunk postural alignment while on moving surfaces, such as • sitting on a therapeutic ball • standing on wobble boards • bouncing on a minitrampoline
- 64. – Progress the activities by movements such as • shifting the body weight • rotating the trunk • moving the head or arms
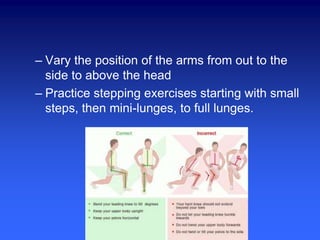
- 65. – Vary the position of the arms from out to the side to above the head – Practice stepping exercises starting with small steps, then mini-lunges, to full lunges.
- 66. – Progress the exercise program to include hopping, skipping, rope jumping, and hopping down from small stool while maintaining balance. – Perform arm and leg exercises while standing with • normal stance • tandem stance • single leg stance
- 67. Balance while standing on wobble boards Balance while standing on wobble boards with arm movements
- 68. Balance while standing on wobble boards with arms above the head One-legged stance with resisted shoulder extension using elastic resistance
- 69. Anticipatory Balance Control • Have the patient practice anticipatory balance control by performing the following. – Reach in all directions to touch or grasp objects, catching a ball, or kicking a ball. – Use different postures for variation (e.g., sitting, standing, kneeling) and throwing or rolling the ball at different speeds and heights.
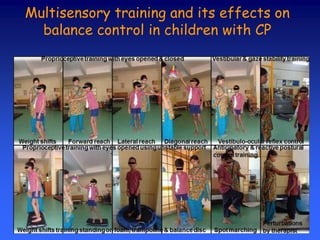
- 70. Multisensory training and its effects on balance control in children with CP
- 71. – Use functional tasks • in different postures at varying speeds • maneuver through an obstacle course.
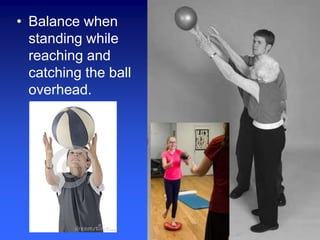
- 72. • Balance when standing while reaching and catching the ball overhead.
- 73. Reactive Balance Control • Have the patient train reactive balance control with the following activities. – Gradually increase the amount of sway when standing in different directions – To emphasize training of the ankle strategy, have the patient practice while standing on one leg with the trunk erect.
- 74. – To emphasize training of the hip strategy • Walk on balance beams or lines drawn on the floor • Perform tandem stance and single-leg stance with trunk bending • Stand on a mini-trampoline
- 75. – To emphasize the stepping strategy, have the patient practice stepping up onto a stool
- 76. – To increase the challenge during these activities, add anticipated and unanticipated external forces. For example, • have the patient lift boxes that are identical in appearance but of different weights • throw and catch balls of different weights and sizes • while on a treadmill, suddenly stop/start the belt or increase/decrease the speed.
- 77. Balance During Functional Activities • Focus on activities similar to the functional limitations identified in the evaluation. – For example, if reaching is limited, the patient should work on activities such as • reaching for a glass in a cupboard • reaching behind • catching a ball
- 78. • Perform two or more tasks simultaneously – increases the level of task complexity • Practicing recreational activities the patient enjoys, such as golf, increases motivation for practice while challenging balance control
- 79. Functional balance during a golf swing
- 82. Health and Environmental Factors • Low Vision • Sensory Loss • Medications
- 83. • Low Vision – encourage regular eye examinations – Wearing a hat and sunglasses in bright sunlight – making sure lights are on when walking about the house at night – avoid using bifocal glasses when walking because • Single lens glasses are safest for improving depth perception and contrast sensitivity, especially on stairs
- 84. • Sensory Loss – For individuals with sensory loss in the legs • caution them to take extra care – when walking on soft carpet or uneven ground • use a cane or other device if necessary – wear firm rubber shoes with low heels – Regular medical examinations • blood glucose levels – Seek medical attention if they experience any symptoms of dizziness.
- 85. • Medications – Patients should be educated about the influence of certain medications • such as sedatives and antidepressants – if such medications are used at night as a sleep aid • patients should take extra precautions when getting up to use the bathroom
- 86. Tai Chi for Balance Training • Popular traditional Chinese exercise • Consisting of a sequence of whole-body movements that are performed – in a slow, relaxed manner with an emphasis on • awareness of posture alignment and • synchronized breathing • The slow, continuous, even rhythm of the movements facilitates – sensorimotor integration – awareness of the external environment
- 87. • Continuous weight shifting from one leg to the other facilitates – anticipatory balance control – motor coordination – lower-extremity strength • Finally, the large dynamic, flowing and circular movements of the extremities promote joint ROM and flexibility.
Editor's Notes
- https://www.facebook.com/hazrat.bilal.malakandi.uthmankhel
- http://wordpress.mrreid.org/2014/09/12/the-difference-between-centre-of-mass-and-centre-of-gravity/
- http://www.oandp.org/olc/lessons/html/SSC_10/section_07.asp?frmCourseSectionId=ACCAA1B7-285D-4735-875D-2AEEF6CA9D6A
- http://www.oandp.org/olc/lessons/html/SSC_10/section_07.asp?frmCourseSectionId=ACCAA1B7-285D-4735-875D-2AEEF6CA9D6A
- http://www.oandp.org/olc/lessons/html/SSC_10/section_07.asp?frmCourseSectionId=ACCAA1B7-285D-4735-875D-2AEEF6CA9D6A
- http://www.oandp.org/olc/lessons/html/SSC_10/section_07.asp?frmCourseSectionId=ACCAA1B7-285D-4735-875D-2AEEF6CA9D6A
- http://www.oandp.org/olc/lessons/html/SSC_10/section_07.asp?frmCourseSectionId=ACCAA1B7-285D-4735-875D-2AEEF6CA9D6A
- Morbidity is a term used to describe how often a disease occurs in a specific area Mortality definition, the state or condition of being subject to death Mortality rate, or death rate, is a measure of the number of deaths (in general, or due to a specific cause) in a particular population, Sensorimotor integration is defined as the capability of the central nervous system to integrate different sources of stimuli, and parallelly, to transform such inputs in motor actions.
- http://balanceandmobility.com/for-patients/testing-balance-disorders/ SE = subjective examination, OE = objective examination sensory input proprioceptive, visual, vestibular sensory processing sensorimotor integration, anticipatory and reactive balance control biomechanical and motor postural alignment, muscle strength and endurance, joint ROM and flexibility, motor coordination, pain Sensory processing disorder is a condition in which the brain has trouble receiving and responding to information that comes in through the senses.
- http://www.topendsports.com/testing/balance.htm
- https://www.youtube.com/watch?v=vw2mNolzvwk http://www.jbiomech.com/article/S0021-9290(16)30048-3/abstract http://doc.utwente.nl/78511/
- https://www.youtube.com/watch?v=h7Djqpsyus4 https://www.youtube.com/watch?v=UQ6-7TrmKxU
- http://www.ijcpjournal.org/article.asp?issn=2395-4264;year=2015;volume=1;issue=2;spage=101;epage=107;aulast=Patel
- https://www.facebook.com/hazrat.bilal.malakandi.uthmankhel