


































Health Assessment Lecture.pdf
- 1. HEALTH ASSESSMENT Afnan Tunsi BSN, RN, MSc.
- 2. Learning Outcomes After completion of this lecture, the student will be able to: Identify purposes of the physical examination. Explain the four techniques used in physical examination. Identify the steps in head examination procedure. Describe suggested sequencing to conduct a head physical health examination. Identify the steps in neck examination procedure. Describe suggested sequencing to conduct a neck physical health examination. 2 Monday, January 05, 2015 A. Tunsi
- 3. Assessing a client’s health status is a major component of nursing care and has three aspects: (a) the nursing health history (b) the physical assessment, and (c) diagnostic testing. The focus of this chapter will be on the physical assessment and diagnostic testing that is required to diagnose a client’s condition. 3 Monday, January 05, 2015 A. Tunsi Health Assessment
- 4. A complete health assessment is conducted in a systematic and efficient manner starting at the head and proceeding downward (head- to-toe assessment). However, nurses could assess a specific body area instead of the entire body. These specific assessments are made in relation to client complaints, the nurse’s own observation of problems, the client’s presenting problem, nursing interventions provided, and medical therapies. 4 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment
- 5. Purpose of physical examination: • To obtain baseline data about the client’s functional abilities. • To supplement, confirm, or disprove data obtained in the nursing history. • To obtain data that will help establish nursing diagnoses and plans of care. • To evaluate the progress of a client’s health problem. • To make clinical judgments about a client’s health status. • To identify areas for health promotion and disease prevention. 5 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment
- 6. 6 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment
- 7. • Clients need an explanation of the physical assessment because they are anxious about what the nurse will find. • The nurse should explain when and where the assessment will take place, why it is important, and what will happen. • Instruct the client that all information is kept confidential. • Health assessments are usually painless; however, it is important to determine in advance any positions that are contraindicated for a particular client. • The nurse assists the client as needed. • Clients should empty their bladders before the assessment to help them feel more relaxed. • When assessing adults it is important to recognize that people of the same age differ markedly.. 7 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment Preparing the Client
- 8. • Be aware of normal physiologic changes that occur with age. • Be aware of stiffness of muscles and joints • Expose only areas of the body to be examined. • Assume the required positions. • Be aware of cultural differences. Arrange for an interpreter if the client’s language differs from that of the nurse. • Ask clients how they wish to be addressed, such as Mrs or Miss. • Adapt assessment techniques to any sensory impairment; for example, make sure eyeglasses or hearing aids are nearby. • If clients are elderly and/or weak it is wise to plan several assessment times in order to not overtire them. 8 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment Preparing the Client
- 9. • The time for the physical assessment should be convenient to both the client and the nurse. • The environment needs to be well lighted and the equipment should be organized for efficient use. • The room should be warm enough to be comfortable for the client. • Providing privacy is important. • Cultural background of the client should be taken into consideration. • Culture, age, and gender of both the client and the nurse influence how comfortable the client will be and what special arrangements might be needed. 9 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment Preparing the Environment
- 10. • Several positions are frequently required during the physical assessment. • It is important to consider the client’s ability to assume a position. • The client’s physical condition, energy level, and age should also be taken into consideration. • Some positions are embarrassing and uncomfortable and therefore should not be maintained for long time. • The assessment is organized so that several body areas can be assessed in one position, thus minimizing the number of position changes needed. 10 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment Positioning
- 11. 11 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment
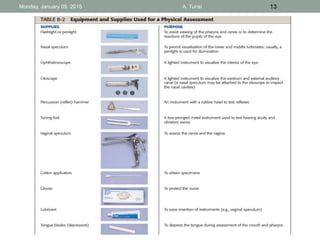
- 12. • Drapes should be arranged so that the area to be assessed is exposed and other body areas are covered. • Exposure of the body is frequently embarrassing to clients. • Drapes provide not only a degree of privacy but also warmth. • Drapes are made of paper, cloth, or bed linen. 12 Monday, January 05, 2015 A. Tunsi Physical HealthAssessment Draping Instrumentation • All equipment required for the health assessment should be clean, in good working order, and readily accessible.
- 13. 13 Monday, January 05, 2015 A. Tunsi
- 14. 14 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment • Four primary techniques are used in the physical assessment: • Inspection • Palpation • Percussion • Auscultation
- 15. Inspection: • Inspection is the visual assessment; that is, assessing by using the sense of sight or vision. • The nurse inspects with the naked eye and with a lighted instrument. • In addition to visual observations, the use of olfactory (smell) and auditory (hearing) senses to observe the condition of various body parts is considered inspection. • Lighting must be sufficient for the nurse to see clearly. • When using the auditory senses it is important to have a quiet environment for accurate hearing. • Observe for color, size, location, texture, symmetry, odors, and sounds. 15 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
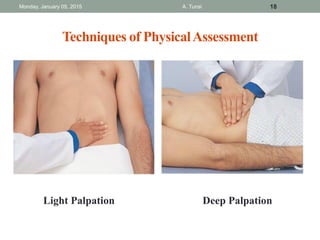
- 16. Palpation: • Palpation is the examination of the body using the sense of touch. • The pads of the fingers are used because their concentration of nerve endings makes them highly sensitive to tactile discrimination. • There are two types of palpation: light and deep. • Light palpation (superficial palpation) should always precede deep palpation because heavy pressure on the fingertips can dull the sense of touch. • For light palpation, the nurse extends the dominant hand’s fingers parallel to the skin surface and presses gently while moving the hand in a circle. 16 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
- 17. Palpation: • With light palpation, the skin is slightly depressed. • If it is necessary to determine the details of a mass, the nurse presses lightly several times rather than holding the pressure. • Deep palpation is usually not done during a routine examination and requires significant practitioner skill. • It is performed with extreme caution because pressure can damage internal organs. • It is usually not indicated in clients who have acute abdominal pain or pain that is not yet diagnosed. • Deep palpation is done with one hand or with two. The top hand applies pressure while the lower hand remains relaxed to perceive the tactile sensations. 17 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
- 18. 18 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment Light Palpation Deep Palpation
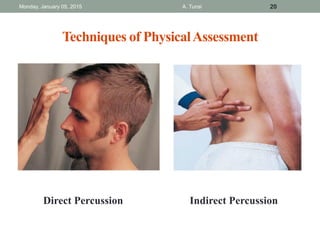
- 19. Percussion: • Percussion is the act of striking the body surface to elicit sounds that can be heard or vibrations that can be felt. • There are two types of percussion: direct and indirect. • In direct percussion, the nurse strikes the area to be percussed directly with the pads of the fingers. • The strikes are rapid, and the movement is from the wrist. • Indirect percussion is the striking of a finger (usually the middle finger) held against the body area to be assessed. • The motion comes from the wrist; the forearm remains stationary. The blows must be firm, rapid, and short to obtain a clear sound. • Percussion is used to determine the size and shape of internal organs by establishing their borders. It indicates whether tissue is fluid filled, air filled, or solid. 19 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
- 20. 20 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment Direct Percussion Indirect Percussion
- 21. Percussion: • Percussion elicits five types of sound. • Flatness is an extremely dull sound produced by very dense tissue such a muscle or bone. • Dullness is a thudlike sound produced by dense tissue such as the liver, spleen or heart. • Resonance is a hollow sound such as that produced by lungs filled with air. • Hyperresonance is not produced in the normal body. It is described as booming and can be heard over an emphysematous lung. • Tympany is a musical or drumlike sound produced from an air-filled stomach. 21 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
- 22. Percussion: 22 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
- 23. Auscultation: • Auscultation is the process of listening to sounds produced within the body. • In auscultation, the nurse uses both direct auscultation by listening to body sounds with the unaided ear, and indirect auscultation by using a stethoscope. • The stethoscope has both a flat disc diaphragm and a bell-shaped amplifier. • The diaphragm best transmits high-pitched sounds (e.g., bronchial sounds), and the bell best transmits low-pitched sounds such as some heart sounds. 23 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
- 24. Auscultation: • Auscultated sounds are described according to their pitch, intensity, duration, and quality. • The pitch is the number of vibrations per second (frequency). • The intensity (amplitude) refers to the loudness or softness of a sound. • The duration of a sound is its length (long or short). • The quality of sound is a subjective description of a sound, for example, whistling, gurgling, or snapping. 24 Monday, January 05, 2015 A. Tunsi Techniques of PhysicalAssessment
- 25. Health assessment begins with a general survey that involves: • Observation of the client’s general appearance and mental status • Measurement of vital signs, height, and weight. Many components of the general survey are assessed while taking the client’s health history, such as the client’s body build, posture, hygiene, and mental status. 25 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 1. General Survey
- 26. 1.1 Appearance and Mental Status: • The general appearance and behavior of an individual must be assessed in relationship to culture, educational level, socioeconomic status, and current circumstances. The client’s age, sex, and race are also useful factors in interpreting findings that suggest increased risk for known conditions. • To assess general appearance and mental status: 1. Observe body build, height, and weight in relation to the client’s age, lifestyle, and health. 2. Observe client’s posture and gait, standing, sitting, and walking. 3. Observe client’s overall hygiene and grooming. 4. Note body and breath odor in relation to activity level. 26 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 1. General Survey
- 27. 1.1 Appearance and Mental Status: 5. Observe for signs of distress in posture or facial expression. 6. Note obvious signs of health or illness (e.g., in skin color orn breathing). 7. Assess the client’s attitude. 8. Note the client’s affect/mood; assess the appropriateness of the client’s responses. 9. Listen for quantity of speech (amount and pace), quality (loudness, clarity, inflection), and organization (coherence of thought, overgeneralization, vagueness). 10. Listen for relevance and organization of thoughts. 27 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 1. General Survey
- 28. 1.2 Vital Signs: Vital signs are measured (a) to establish baseline data against which to compare future measurements and (b) to detect actual and potential health problems. 28 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 1. General Survey
- 29. 1.3 Height and Weight: • Measuring the weight and height provides important assessment data on the client’s general health status. • Weight and height are usually measured when a client is admitted to a health institution, and often regularly. • The nurse measures height with a measuring stick attached to weight scales or to a wall. • The client should remove the shoes and stand erect and the body against the measuring stick. The nurse raises the L-shaped sliding arm on the weight scale until it rests on top of the client’s head, or places a ruler on the client’s head. • The edge of the ruler should abut the measuring guide. 29 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 1. General Survey
- 30. 1.3 Height and Weight: • If the client is a child under the age of 2 years, measure height in the supine position with knees fully extended. • To measure weight the nurse should use the same scale each time, take the measurements at the same time each day, and make sure the client has on a similar kind of clothing and no footwear. • Clients who cannot stand are weighed on chair or bed scales. 30 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 1. General Survey
- 31. 3.1 Skull and Face: • The skull can be of variable size and shape according to the client’s age and body build. • The skull is made up of many bones, namely: frontal, parietal, occipital, mastoid process, mandible, maxilla, and zygomatic. • Many disorders cause a change in facial shape or condition. For example, kidney or heart disease can cause edema of the eyelids, hyperthyroidism can cause a protrusion of the eyeballs (exophthalmos), and increased adrenal hormone production can cause a round face (moon face) 31 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Head
- 32. 3.1 Skull and Face: 32 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Head
- 33. 3.2 Eyes and Vision: • An eye assessment should be carried out as part of the client’s initial physical examination; • periodic reassessments need to be made for clients in long-term care. • The nurse should start an eye assessment by examining the external structures and ocular movement. • Then examination of the visual acuity (the degree of detail the eye can determine in an image) and visual fields (the area an individual can see when looking straight ahead). 33 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Head
- 34. 3.2 Eyes and Vision: 34 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Head
- 35. 3.3 Ears and Hearing: • Assessment of the ear includes direct inspection and palpation of the external ear, inspection of the remaining parts of the ear by an otoscope, and determination of auditory acuity. • The ear is usually assessed during an initial physical examination; periodic reassessments may be necessary for long- term clients or those with hearing problems. • The ear is divided into three parts: external ear, middle ear, and inner ear. 35 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Head
- 36. 3.4 Nose and Sinuses: • A nurse can inspect the nasal passages very simply with a flashlight or a penlight. However, in specialist environments such as an ear, nose, and throat facility, a nasal speculum can be used to assess the nasal cavity. • Assessment of the nose includes inspection and palpation of he external nose; patency of the nasal cavities; and inspection and palpation of the facial sinuses. 36 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Head
- 37. 3.5 Mouth and Oropharynx: • The mouth and oropharynx are composed of a number of structures: lips, inner and buccal mucosa, the tongue and floor of the mouth, teeth and gums, hard and soft palate, uvula, salivary glands, tonsillar pillars, and tonsils. • The nurse inspects and palpates the client’s mouth and oropharynx using a penlight. However, detailed assessment is usually performed by an expert such as the dentist. 37 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Head
- 38. • Examination of the neck includes the muscles, lymph nodes, trachea, thyroid gland, carotid arteries, and jugular veins. • Areas of the neck are defined by the sternocleidomastoid muscles, which divide each side of the neck into two triangles: the anterior and posterior. 38 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Neck
- 39. • The trachea, thyroid gland, anterior cervical nodes, and carotid artery lie within the anterior triangle. • The greatest number of lymph nodes are located in the head and neck. • Therefore, the nurse should carefully inspect and palpate the lymph nodes in both sides of the neck. 39 Monday, January 05, 2015 A. Tunsi Sequence to conduct PhysicalAssessment 3. The Neck
- 40. References Monday, January 05, 2015 A. Tunsi 40 Kozier, B., Erb, G., Berman, A., Snyder, S., Abdalrahim, M., Abu-Moghli, F., Saleh M. (2012). Fundamentals of Nursing: Concepts, Process, and Practice. Essex, England: Pearson Education Limited.