Introduction to Operative Dentistry
•Download as PPTX, PDF•
16 likes•3,466 views

Operative dentistry deals with the diagnosis, prevention, and restoration of tooth structure to correct defects, restore function and aesthetics. The history of operative dentistry began with tooth extractions in the middle ages and has evolved to be more evidence-based and focused on minimally invasive techniques. It is indicated to treat conditions like dental caries, trauma, and developmental defects. Its main objectives are diagnosis, prevention, preservation and restoration of teeth. There are different systems for notation of individual teeth, with the most commonly used systems being the Universal system and FDI (Federation Dentaire Internationale) two-digit system.



































Introduction to Operative Dentistry
- 1. I N T R O D U C T I O N T O O P E R A T I V E D E N T I S T R Y B Y DR. NUHA ELKADIKI (MDS)
- 3. CONTENT OF LECTURE: 1. Definition of operative dentistry. 2. History and Epidemiology. 3. Indication of operative dentistry. 4. Objective of operative dentistry. 5. Tooth numbering system(tooth notation) : A. Universal numbering system. B. Palmer national numbering system. C. Federation Dentaire Internationale Numbering System (FDI).
- 4. 1. DEFINITION OF OPERATIVE DENTISTRY: Operative Dentistry is the art and science of the prevention, diagnosis, treatment and prognosis of defects in the enamel and dentin of individual teeth. Also known as Restorative Dentistry or Conservative Dentistry. According to Mosby's dental dictionary's, operative dentistry deal with the function and esthetic restoration of hard tissue of individual teeth.
- 5. 1. DEFINITION OF OPERATIVE DENTISTRY: • Such treatment should result in the restoration of proper tooth form, function, and esthetics while maintaining the physiologic integrity of the teeth in harmonious relationship with the adjacent hard and soft tissues. • all of which should enhance the general health and welfare of the patient.
- 8. 2. HISTORY AND EPIDEMIOLOGY Operative Dentistry was considered to be the entirety of the clinical practice of dentistry. Has been recognized as the foundation of dentistry and the base from which most other aspects of dentistry evolved.
- 9. 2. HISTORY AND EPIDEMIOLOGY The profession of dentistry was born during the early middle ages. Barbers was doing well for dentistry ,by removing teeth with complications .
- 10. 2. HISTORY AND EPIDEMIOLOGY The practice of these early dentists consisted mainly of tooth extraction and practice of dentistry during the founding year was not based on scientific knowledge. Baltimore College of Dental Surgery in 1840 ⇒ dental education. Harvard University in 1867 ⇒ dental program. In France, Louis Pasteur discovered the role of microorganisms in disease ⇒ have a significant impact on the developing dental + medical profession.
- 11. 2. HISTORY AND EPIDEMIOLOGY In 1898, Dr. G.V. Black is known as father of operative dentistry. In United States, G.V. Black became the foundation of the dental professions ⇒related the clinical practice of dentistry to a scientific basis.
- 12. 2. HISTORY AND EPIDEMIOLOGY The scientific foundation for operative dentistry was further expanded by Blacks son , Arthur Black. Others made significant contributions in the early development of Operative Dentistry: – Charles E. Woodbury – E.K. Wedelstaedt – Waldon I. Ferrier – George Hollenback
- 13. 2. HISTORY AND EPIDEMIOLOGY • In early part of 1900s ,progress in dental sciences and technologies was slow .many advance were made during the 1970s in materials and equipiements.by this time ,it was also proved that dental plaque was the causative agent for caries.
- 14. 2. HISTORY AND EPIDEMIOLOGY In the 1990s, oral health science ,started moving toward an evidence-based approach for treatment of decayed teeth. The recent concept of treatment of dental caries comes under minimally invasive dentistry. In December 1999 ,the world congress of minimally invasive dentistry (MID)was formed.
- 15. 2. HISTORY AND EPIDEMIOLOGY Current minimally intervention philosophy ,Follow three concepts of disease treatment: 1. Identify : identify and assess risk factors early. 2. Prevent :prevent disease by eliminating risk factors. 3. Restore: restore the health of the oral environment.
- 16. 3. INDICATION OF OPERATIVE DENTISTRY. Is indicated in following conditions : 1. Caries.
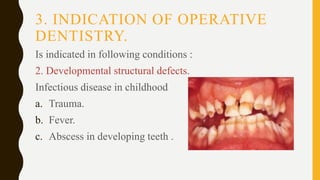
- 17. 3. INDICATION OF OPERATIVE DENTISTRY. Is indicated in following conditions : 2. Developmental structural defects. Infectious disease in childhood a. Trauma. b. Fever. c. Abscess in developing teeth .
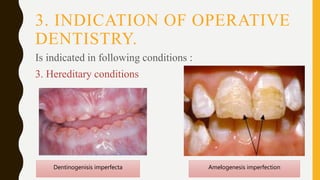
- 18. 3. INDICATION OF OPERATIVE DENTISTRY. Is indicated in following conditions : 3. Hereditary conditions Amelogenesis imperfectionDentinogenisis imperfecta
- 19. 3. INDICATION OF OPERATIVE DENTISTRY.
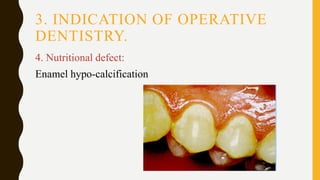
- 20. 3. INDICATION OF OPERATIVE DENTISTRY. 4. Nutritional defect: Enamel hypo-calcification
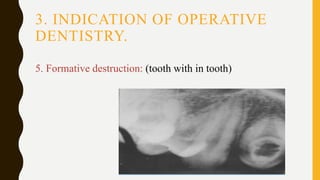
- 21. 3. INDICATION OF OPERATIVE DENTISTRY. 5. Formative destruction: (tooth with in tooth)
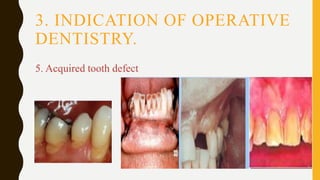
- 22. 3. INDICATION OF OPERATIVE DENTISTRY. 5. Acquired tooth defect
- 23. 3. INDICATION OF OPERATIVE DENTISTRY. 6. discoloration:
- 24. 3. INDICATION OF OPERATIVE DENTISTRY. 7. Accidental trauma:
- 25. 3. INDICATION OF OPERATIVE DENTISTRY. 8. Malformed tooth:
- 26. 3. INDICATION OF OPERATIVE DENTISTRY. 9. Esthetic improvement:
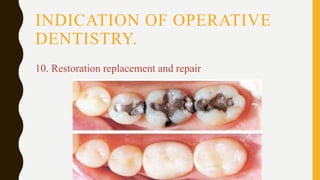
- 27. INDICATION OF OPERATIVE DENTISTRY. 10. Restoration replacement and repair
- 28. 4.OBJECTIVE OF OPERATIVE Operative dentistry have a five fundamental aims: A. Diagnosis . B. Prevention. C. Interception. D. Preservation. E. Restoration. F. Maintenance
- 29. 4. OBJECTIVE OF OPERATIVE A. Diagnosis: It’s the determination of the nature of the disease ,injury and congenital defects by examinations ,tests and investigations . Proper diagnosis is vital for treatment planning.
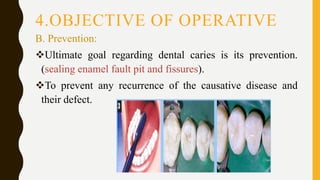
- 30. 4.OBJECTIVE OF OPERATIVE B. Prevention: Ultimate goal regarding dental caries is its prevention. (sealing enamel fault pit and fissures). To prevent any recurrence of the causative disease and their defect.
- 31. 4. OBJECTIVE OF OPERATIVE C. Interception: This procedure in operative dentistry refers to preventing further loss of tooth structure by stabilizing an active disease process.
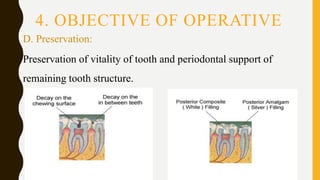
- 32. 4. OBJECTIVE OF OPERATIVE D. Preservation: Preservation of vitality of tooth and periodontal support of remaining tooth structure.
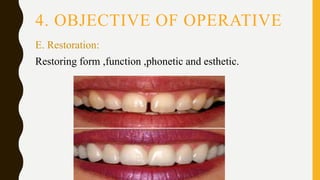
- 33. 4. OBJECTIVE OF OPERATIVE E. Restoration: Restoring form ,function ,phonetic and esthetic.
- 36. •To achieve the ultimate goals of operative dentistry, any restorative performance, requires: 1. Full knowledge about human anatomy and microbiology. 2. Posses a high developed technical skills. 3. Demonstrated artistic abelites.
- 39. 3. TOOTH NOTATION Several different systems are available for tooth reference; there are however three systems that most practitioners should be aware of in order to be familiar with the increasing internationalization of dental journals, conferences and other forms of communication. Most systems divide the mouth into four quadrants, which are indicated as if one is viewing the patient from the front:
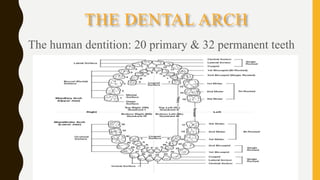
- 41. THE DENTAL ARCH The human dentition: 20 primary & 32 permanent teeth
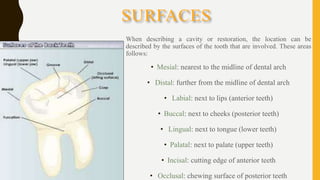
- 42. SURFACES When describing a cavity or restoration, the location can be described by the surfaces of the tooth that are involved. These areas follows: • Mesial: nearest to the midline of dental arch • Distal: further from the midline of dental arch • Labial: next to lips (anterior teeth) • Buccal: next to cheeks (posterior teeth) • Lingual: next to tongue (lower teeth) • Palatal: next to palate (upper teeth) • Incisal: cutting edge of anterior teeth • Occlusal: chewing surface of posterior teeth
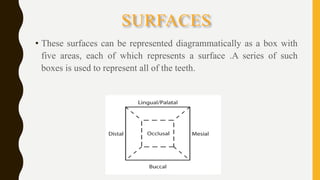
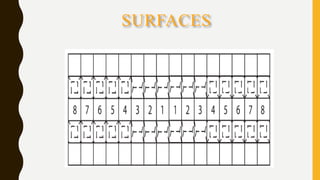
- 43. SURFACES • These surfaces can be represented diagrammatically as a box with five areas, each of which represents a surface .A series of such boxes is used to represent all of the teeth.
- 44. SURFACES
- 45. QUADRANTS
- 46. 3.TOOTH NOTATION: A. Palmer system : In 1861 Adolph Zsigmondy of Vienna introduced the symbolic system for permanent dentition. He then modified it for the primary dentition in 1874. The symbolic system is now commonly referred to as the Palmer notation system or Zsigmondy system. Also called Angular or Grid system. Oldest numbering system.
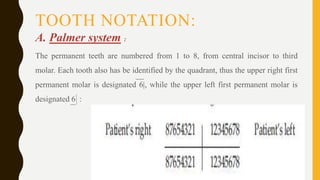
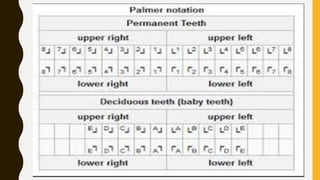
- 47. TOOTH NOTATION: A. Palmer system : The permanent teeth are numbered from 1 to 8, from central incisor to third molar. Each tooth also has be identified by the quadrant, thus the upper right first permanent molar is designated 6|, while the upper left first permanent molar is designated 6 :
- 48. TOOTH NOTATION; A. Palmer system : The primary (deciduous) teeth are represented by the letters A to E, from central incisor to second deciduous molar and also have to have a quadrant designation e.g. the upper right deciduous central incisor is A|.
- 50. 3. TOOTH NOTATION; Advantages of Palmer: 1. Simple to use. 2. No confusion between primary & permanent dentition. Disadvantage of palmer system: 1. Oral communication is difficult. 2. Opposing or contralateral teeth are indicated by same number or alphabet which is confusing.
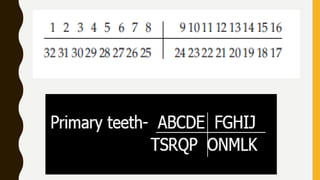
- 51. 3. TOOTH NOTATION; B. UNIVERSAL SYSTEM This system is commonly used in America. The teeth are given individual numbers from 1 to 32, starting with the upper right third molar and moving clockwise round the arch to the lower right third molar.
- 52. 3. TOOTH NOTATION; B. UNIVERSAL SYSTEM ADA officially recommended the Universal system in 1968. In this system for the permanent dentition the maxillary teeth are numbered through 1 to 16 beginning with upper right third molar. • The mandibular teeth are numbered through 17 to 32 beginning with lower left third molar. The universal system notation for primary dentition utilises upper case alphabets.
- 55. 3. TOOTH NOTATION; B. UNIVERSAL SYSTEM In this system, the teeth that should be there are numbered. If you are missing your third molars, your first number will be 2 instead of 1, acknowledging the missing tooth. If you’ve had teeth removed or teeth missing, the missing teeth will be numbered as well.
- 56. 3. TOOTH NOTATION; Advantages ADA 1. Each tooth has a separate unique letter or number to denote it. Disadvantage of ADA 1. Difficult to remember letters or numbers of individual teeth.
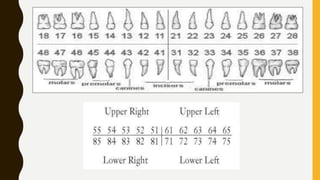
- 57. 3. TOOTH NOTATION; C. FDI system (Federation Dentaire Internationale)(Two Digit Notation): • The FDI system is a two digit system that has been adopted by WHO . • In this system the first digit indicates the quadrant and the second digit indicates the tooth within the quadrant. 1 to 4 and 5 to 8 as the first digit indicates permanent and primary dentition respectively. • 1 to 8 and 1 to 5 as the second digit indicates permanent and primary teeth respectively.
- 59. 3. TOOTH NOTATION; Advantages: 1. Each tooth has a separate number. 2. Simple to understand and teach. 3. Easy to pronounce in conversation. 4. Easy to transmit over computer & easy for charting. Disadvantage: May be confused with ADA numbers.