Knee joint assessment
•Download as PPTX, PDF•
4 likes•1,731 views

complete Knee joint assessment from physiotherapeutic point of view. Includes observation , palpation , assessment, special test, differential diagnosis of knee joint .
Report
Share










































































Knee joint assessment
- 1. Pt. Assessment of Knee Joint By :- Dr. Taniya verma ( PT) MPT-musculoskeletal
- 2. Knee joint • Tibiofemoral joint • Modified hinge joint having 3 degree of freedom • Resting position- 25 degree flexion • Closed pack position- full extension , lateral rotation of tibia • Capsular pattern – flexion, extension • Space between bones filled by menisci – medial (c shape) & lateral menisci ( O shape) ; thick along periphery and thinner along inner margin
- 3. • Patellofemoral joint • Thickest layer of cartilage in patella; has 5 facets- superior, inferior, lateral, medial and odd( frequently affected in patellofemoral syndrome) • malalignment of patellar movement can lead to patellofemoral arthralgia • Patella function as guide for quads tendon, decreases friction, control capsular tension in knee, act as bony shield for cartilage of femoral condyle
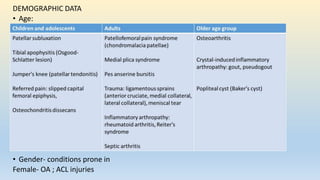
- 5. DEMOGRAPHIC DATA • Age: • Gender- conditions prone in Female- OA ; ACL injuries
- 6. CHIEF COMPLAINTS • IN PATIENT’S OWN WORD • Pain • Swelling : immediate, delayed • Stiffness • Deformity • Locking • Giving away • Limp • Loss of function
- 7. HISTORY OF PRESENT ILLNESS • ONSET OF PAIN • Date of injuy or when symptoms started • Gradual/Sudden • Progression- getting better/getting worse/no change • LOCATION OF PAIN • Anterior • Lateral • Medial • posterior
- 9. Lateral knee pain • IT band friction syndrome • Biceps femoris tendonitis • osteoarthritis • Poplitius tendonitis.
- 10. Medial knee pain
- 13. Mechanism of present illness-Helps predict injured structure • Contact or non contact injury? • If contact, what part of knee was contacted? • Anterior blow/ varus force/valgus force • Was foot of affected knee plated on the ground? (closed vs open chain injury ) • Bony avulsions- slow developing forces • Ligament tear- Rapidly developing forces • MCL injury- Valgus force • LCL injury- Varus force
- 15. • ACL INJURY • Common in wt.bearing, slight flexion and rotation • Anterior translator force on proximal tibia • Hyperextension injury
- 16. • PCL INJURY • Posterior translation of tibia • Pretibial trauma( Dashboard trauma)
- 17. • MENISCAL INJURY • Twisting force (injury with rotation of tibia) in weight bearing
- 18. • Any ‘clicking’ or ‘pop’ sound during injury? • Indicates ligament tear in knee joint • Any ‘give away’ or ‘catch’? • Give away= instability • Catch= (lock) meniscal injury • Swelling immediate or delayed • Synovial swelling= takes 8-24 hrs to develop • Immediate (0–2 hours) (hemarthrosis)= ACL rupture,patellar dislocation • Delayed (6-24 hrs)(effusion)= meniscus • No swelling = MCL sprain • Localized swelling- extracapsular injury • Generalised swelling- Intracapsular injury
- 19. • History of type of shoes patient normally uses?- flat/high heels • Functional ability of the patient? • Any disability in running, climbing stairs etc • SPORTS SPECIFIC HISTORY • Total duration of play • Total practice/ training session • Exercise porotocol- warmup/cool down • Competition. • Past history • Any previous injury indicates recurrent injuries around knee • Was the pain at the same site? • Similar nature? • Treatment given previously
- 20. PAIN ASSESSMENT • Site of pain – retropatellar? • Type of pain • Aching pain = degenerative pain • Sharp catching pain= mechanical problem • Arthritic pain= associated with stiffness and eases with movement • Pain at rest= is not mechanical pain • Pain during activity= sublaxation, patellar tracking disorder • Pain after activity= synovitis, tendinitis • Constant pain irrespective of activity= tumor? • Pain around knee= contusion, tear of ligament, muscle • Ask if patient has pain during any specific activity or position or movement.
- 21. BODY CHART
- 22. • Aggrevating/ relieving factors • Severity of pain • VAS/NPRS
- 23. OBSERVATIONS • VIEW FOR OBSERVATIONS • Standing • Anterior, posterior and lateral view • Sitting • Anterior and lateral view • Lying • Supine, side-lying and prone
- 24. • Patient should be exposed to see knee joint and a joint proximal and distal to it. ( hip and ankle) • Key points • Consent • Adequate explanation about the necessity of exposure during patient assessment and its benefits in the treatment • Confined place and environment to maintain patient’s privacy
- 25. Observation : anterior view ( standing) • Knee joint alignment • Genu valgum /genu varum/windstep deformity • Children at age of 18-19 months: genu varus which is normal • Age 3-4 knee attains valgum • Swelling • Quadriceps wasting?- disuse atrophy/quadriceps inhibition • Position of patella • Squinting of patella- medially facing patella
- 26. 1.VARUS / 2.VALGUS/ 3.WINDSWEPT DEFORMITY
- 27. Miserable malalignment syndrome. The patient often presents with medial parapatellar pain with no localizing findings or images indicating pathology: A, when viewed from the front, the squinting patella on the right is well visualized, with both femurs having greater than 50° anteversion; B, what the patient sees looking down her legs
- 28. Observation : lateral view ( standing) • Any discoloration / bruising/ abrasion/scars • Knee alignment • Genu recurvatum- hyperextension of knee • Position of patella • Patella alta- abnormal high position of patella (camel sign ) • Patella baja- abnormally low position of patella • Alignment of other joint- ankle ,hip and spine. • Lordosis of spine is related to degenerative changes in the knee ( spine-knee syndrome)
- 29. Camel sign- because of high patella ( one hump), the infrapatellar fat pad ( second hump) or inflamed infrapatellar bursae becomes more prominent
- 30. Observation : Posterior view ( standing) • Any abnormal swelling? • Baker’s cyst • Gastrocnemius- semimembranous bursae • Popletial artery aneurysm • Lymphadenopathy • Soft tissue tumor • Wasting of hamstring and calf
- 31. Observation :sitting (lateral and anterior view) • Observe for position of patella • Patella should face forward and should rest on the distal end of femur. • In patella alta= patella rest in anterior surface of femur • Frogeyes patella or grasshopper patella- patella face upward and outward away from each other • Grasshopper eyes or frog eyes is seen in patients whose patellae are proximally displaced (patella alta) and externally or laterally rotated (lateral patellar tilt) • Enlarged tibial tubercle= Osgood schlatter disease.
- 32. • Fig-pre patellar bursitis.
- 33. General observation • Built • Facial expressions • Posture • Guarding/splinting • Extra devices • Gait – antalgic/ hand to knee gait in quadriceps weakness
- 35. • located more distally than prepatellar bursitis and is often caused by frequent kneeling in an upright position
- 36. Pain and tenderness on the inside of your knee, approximately 2 to 3 inches below the joint, are common symptoms of pes anserine bursitis of the knee.
- 39. Osgood-Schlatter disease • It is an inflammation of the area just below the knee where the tendon from the kneecap (patellar tendon) attaches to the shinbone (tibia). • In Osgood-Schlatter disease, the enlarged, inflamed tibial tubercle is nearly always tender when pressure is applied.
- 40. PALPATION • ( WITH VARIOUS ANGLES OF KNEE FLEXION ) • Medio-patellar plica- on medial border of patella • Jumper’s knee- at the apex of patella ( patellar tendon) • Patellar tendinitis: palpate distally • Housemaid’s knee: prepatellar bursitis. • Patellar retinaculum :can be palpated on either side of patella • Quadriceps muscle: can be palpated for any strain,wasting or hard muscle(myositis ossificans) • MCL: along the medial aspect of knee. • Pes Anserine bursitis: medial and slight distal to tibial tuberosity.
- 41. • Temperature: proximal to distal • Tenderness: • For soft tissue and bony tenderness. • Knee flexed at 90’ – examined for tenderness along medial an lateral joint line. • Knee extended • Retropatellar area- by gliding movement of patella between thumb and index finger on medial and lateral facets, try to palpate undersurface of patella. • Patellofemoral crepitions. • Distal pulsations • Poplitieal pulse
- 42. Resisted isometric contractions • Extension of the knee • Flexion of the knee • Ankle dorsiflexion • Ankle plantar flexion
- 46. Muscle length testing • Rectus femoris ( ely test ) • Distal hamstring length test
- 47. Joint play movement • Backward movement of tibia on femur. ( similar to posterior drawer test) • Forward movement of tibia on femur (similar to the anterior drawer test) • Medial and lateral translation of tibia on femur. • Medial and lateral displacement of patella. • Anteroposterior Movement of Fibula on Tibia
- 49. Special test TEST FOR LIGAMENT STABILITY • One plane medial and lateral instability –valgus and varus stress test • One plane anterior and posterior instability- posterior sag sign, Lachman test, drawer sign, active drawer test • Anteromedial and anterolateral rotary instabilities - Lateral pivot shift maneuver, Jerk test of hughston; cross over test of Arnold, slocum test • Posteromedial and posterolateral rotary instabilities - Posteromedial pivot shift Jakob test (reverse pivot shift maneuver), Hughston posterolateral and posteromedial drawer sign . • Tests for meniscus injury- McMurray test , Apley’s test. • Plica test - Mediopatellar plica test • Tests for patellofemoral dysfunction - Clarke’s sign ; McConnell test for chondromalacia patella • Tests for swelling -Brush, stroke, or bulge test ; Fluctuation test ; Patellar tap test (ballotable patella) • Test for patellar dislocation- fairbank apprehension test
- 50. Valgus and Varus stress test
- 52. Lachman test
- 53. Drawer sign
- 55. Anterolateral instability • Lateral pivot shift test • Jerk test of hughston
- 56. Cross over test of Arnold slocum test
- 57. Jackob test (reverse pivot shift maneuver)
- 58. Postero-medial pivot shift test
- 59. Hughston’s posteromedial and posterolateral drawer test
- 60. Meniscus injury • McMurray test • Apley’s test
- 61. Mediopatellar plica test (Mital-hayden test)
- 62. CLARKE’S SIGN • PURPOSE -To assess for patellofemoral dysfunction. • PATIENT POSITION - supine with the knee extended. • EXAMINER POSITION -The examiner stands adjacent to the patient’s knee. • TEST PROCEDURE • The unaffected leg is tested first. The thenar web space of one of the examiner’s hands is placed slightly proximal to the upper pole or base of the patella. The examiner presses down several times with increasing force until pain is produced on the proximal aspect of the patella. The patient then is asked to contract the quadriceps muscles after the examiner pushes down. The test is repeated with the painful knee, and the amounts of pressure that cause pain are compared. • INDICATIONS OF A POSITIVE TEST A positive test result is indicated if the test causes retro patellar pain and the patient cannot hold a contraction. If the patient can complete and maintain the contraction without pain, the test result is considered negative, as long as the same test on the unaffected leg does not cause pain. • CAUTIONS • Because a positive test result can be obtained on anyone if sufficient pressure is applied to the patella, the amount of pressure applied must be carefully controlled and compared with the opposite side. This is best done by repeating the procedure several times, increasing the pressure each time and comparing the results with those on the unaffected side. • • To test different parts of the patella, the knee may be tested in 30°, 60°, and 90° of flexion and in full extension.
- 63. MCCONNELL TEST FOR CHONDROMALACIA PATELLA • The unaffected leg is tested first. After the examiner has positioned the knee at 120°, 90°, 60°, 30°, and 0° (full extension), the patient performs isometric quadriceps contractions with the femur laterally rotated, with each contraction held for 10 seconds. If pain is produced during any of the contractions, the patient’s leg is passively returned to full extension. The leg then is fully supported on the examiner’s knee, and the examiner pushes the patella medially. The medial glide is maintained while the knee is returned to the painful angle, and the patient performs an isometric contraction again, with the patella held medially. The two legs are compared. • If the pain is decreased when the patella is held medially, the pain is patellofemoral in origin.
- 64. BRUSH, STROKE, OR BULGE TEST for effusion • PURPOSE - To assess minimal effusion in the knee. • PATIENT POSITION -The patient lies supine. • EXAMINER POSITION - The examiner is positioned adjacent to the test knee. • TEST PROCEDURE • The examiner places one hand over the anteromedial tibia. Starting just below the joint line on the medial side of the patella and using the palm and fingers, the examiner strokes proximally toward the patient’s hip, as far as the suprapatellar pouch, two or three times. With the opposite hand, the examiner strokes down the lateral side of the patella. • INDICATIONS OF A POSITIVE TEST A positive test result is indicated when a wave of fluid passes along the medial side of the joint and bulges just below the medial distal portion or border of the patella during the down stroke. The wave of fluid may take up to 2 seconds to appear. • CLINICAL NOTES • Also called the wipe test, this test assesses minimal effusion. • Normally, the knee contains 1 to 7 ml of synovial fluid. This test can show as little as 4 to 8 ml of extra fluid within the knee.
- 65. Fluctuation test • PATIENT POSITION -supine. • EXAMINER POSITION -adjacent to the test knee. • TEST PROCEDURE - The examiner places the palm of one hand over the suprapatellar pouch and the palm of the other hand anterior to the joint at the joint line, with the thumb and index finger just beyond the margins of the patella.Pressing down with one hand and then the other, the examiner may feel the synovial fluid fluctuate under the hands and move from one hand to the other. • INDICATIONS OF A POSITIVE TEST- Increased fluctuation of fluid in the knee compared to the contralateral knee indicates significant effusion.
- 66. Patellar tap test • PATIENT POSITION -The patient lies supine. • EXAMINER POSITION -The examiner is positioned adjacent to the test knee. • TEST PROCEDURE - With the patient’s knee extended or flexed to discomfort, the examiner applies a slight tap or pressure over the patella. • INDICATIONS OF A POSITIVE TEST- When the tap is applied, the patella should be felt to fl oat; this is sometimes called the “dancing patella” sign.
- 67. FAIRBANK’S APPREHENSION TEST • PURPOSE -To assess for dislocation of the patella. SUSPECTED INJURY Dislocation or subluxation of the patella • PATIENT POSITION -The patient lies supine with the quadriceps muscles relaxed and the knee flexed to 30º over the examiner’s leg. • EXAMINER POSITION - The examiner sits directly adjacent to the test knee. • TEST PROCEDURE - The unaffected leg is tested first. The examiner’s thumbs are placed on the medial border of the patella, and the fingers are placed on the lateral aspect of the patient’s knee. The examiner carefully and slowly pushes the patella laterally with the thumbs. The two legs are compared. • INDICATIONS OF A POSITIVE TEST If the patient feels that the patella is going to dislocate, he or she will contract the quadriceps muscles to bring the patella “back into line.” This action indicates a positive test result. The patient also will have an apprehensive look.
- 68. Differential diagnosis by location •ANTERIOR- patellofemoral syndrome, bursitis, Osgood schalatter’s disease, patellar tendinitis, patellar fractur •MEDIAL- meniscus, MCL, OA, pes anserine bursitis •LATERAL- Meniscus, LCL, OA, iliotibal friction band syndrome, Fibular head dysfunction •POSTERIOR- Hamstring injury, Baker’s cyst, Neurovascular injury ( popliteal artery or nerve. )
- 72. Differential diagnosis by location anterior knee pain Condition Typical finding Tibial apophysitis Tendar and swollen tibial tuberosity Resisted active extension and passive hyperflexion of knee painful Patellar tendonitis Tender patellar tendon; resisted knee extension painful Slipped capital femoral epiphysis Displacement of epiphysis of femoral head in radiographs; passive hip IR painful PFPS Slight effusion along with patellar crepitus on ROM; reproduction of patient’s pain by applying direct pressure at anterior aspect of patella ACL injury Positive anterior drawers test; Lachman test
- 73. Medial knee pain Condition Typical findings Medial plica syndrome Tenderness near medial patellar retinaculum that worsen with knee flexion MCL tear Laxity; regional pain with valgus stress testing Meniscal tear Tenderness over medial joint line; positive McMurry test OA Regional medial knee pain; tender joint line; decreased ROM; degenerative changes in radiograph Pes anserine bursitis Tenderness 2-4 cm below medial joint line; painful resisted knee flexion in prone position Medial collateral ligament sprain Point tenderness at medial joint line; positive valgus stress test
- 74. Lateral knee pain Condition typical findings Iliotibial band tendonitis Tenderness at lateral epicondyle of femur approx. 3 cm proximal to the joint line Positive noble test Lateral collateral ligament sprain Point tenderness at lateral joint line; positive varus stress testing
- 75. Posterior knee pain Conditions Typical findings Popliteal cyst Palpable fullness at medial aspect of popletial area, at or near the origin of medial head of gastrocnemius Hamstring tendonitis Localized tenderness over medial hamstring tendon insertion
- 76. Comparison of clinical features of 3 common cause of anterior knee pain Signs Patellofemoral pain Patellar tendinopathy Fat pad impingement Onset Running ( esp. downhill) Steps/hills Wt. bearing act. involving knee flexion Act. Involving jumping/changing directions Often but not always, sudden onset with hyperextension injury Pain Non specific/vague Med./lat./infrapatellar Increased by act. That load PFJ Around inferior pole of patella Inc. by jumping & early to mid squat Around inferior pole of patella Inc. by prolonged standing, stairs, knee extension Inspection Generally normal Or VMO wasting Generally quadriceps wasting Puffiness may be apparent around tendon which may make pole of patella appear to be displaced posteriorly Swelling May have small effusions, Rare, tendon may be May have a puffy
- 77. Signs Patellofemoral pain Patellar tendinopathy Fat pad impingement Clicks Occasional No No Crepitus Occasionally under patella No No Giving way Occasional Occasionally due to quadriceps inhibition No Knee ROM Usually normal May be decreased Usually normal, No pain with overpressure Active extension may be painful in acute fat pad impingement Passive overpressure into ext. is painful PFJ movement May be restricted n any direction ( commonly medial glide due to tight lateral structure) May have normal PFJ biomechanics Normal or posteriorly displaced inferior pole of patella. Functional testing Squats, stairs may aggravates PFJ taping should decrease pain Decline squats aggravates pain PFJ taping has less effect Aggravates by squats PFJ taping should decrease pain if inferior pole of patella is tilted up.
- 78. References :- • David J. Magee-orthopedic physical assessment 5th edition • Peter brunker and karim khan- clinical sports medicine .3rd edition • Muscle Function Testing : Vladimir Janda • Measurement of Joint Motion A Guide to Goniometry : Cynthia C norkin ( third edition )