Muscle Energy Technique (MET)

Muscle energy techniques (MET) involve voluntary muscle contractions by the patient against a counterforce applied by the practitioner. The goal is to move restrictive barriers and normalize muscle and fascial restrictions. Key elements include controlled joint positioning, patient-applied muscle contractions in a specific direction, and operator counterforce. MET can be used to lengthen shortened muscles, strengthen weakened muscles, reduce pain and edema, and increase joint mobility. It relies on principles like post-isometric relaxation and reciprocal inhibition. Careful technique and patient/practitioner coordination are important for success. MET can help many somatic dysfunctions but requires an understanding of indications and contraindications.

























Muscle Energy Technique (MET)
- 1. MUSCLE ENERGY TECHNIQUES Dr Venus Pagare MET Venus Pagare5/5/2014
- 2. History • Fatherof MET • Dr. Fred L. Mitchell MET Venus Pagare5/5/2014
- 3. • Muscle energy technique is a manual medicinetreatment procedure that involves voluntary contraction of patientmuscle in: –a preciselycontrolled direction –at varyinglevelsof intensity –againsta distinctlyexecutedcounterforce appliedby theoperator. MET Venus Pagare5/5/2014
- 4. • Activetechniqueas patient contributes correctiveforce • Activating force is classified as intrinsic : patient is responsiblefor dosage applied MET Venus Pagare5/5/2014
- 5. Basic Elements 1. Patient-activemusclecontraction 2. Controlled joint position 3. Muscle contraction in a specific direction 4. Operator-applied distinct counterforce 5. Controlled contraction intensity MET Venus Pagare5/5/2014
- 6. Barrier Concept Physiologic barrier Elastic barrier Anatomic barrier Restrictive barrier MET Venus Pagare5/5/2014
- 7. • Barrier: 1st sign of palpated or sensed resistance to freemovements • When motion is lost withinrange, barrier that preventsmovement in direction of motionlossis defined as “restrictive barrier” • MET works to moverestrictivebarrier as far into the directionof motion loss as possible MET Venus Pagare5/5/2014
- 9. Principles of MET Postisometric relaxation (PIR) Reciprocal inhibition (RI) MET Venus Pagare5/5/2014
- 10. Post-isometric Relaxation • After a muscle is contracted,it is automatically in a relaxed statefor a brief,latent period MET Venus Pagare5/5/2014
- 11. Method For hypertonicmuscle • Taken to the lengthenposition • 20%of strength contraction for 5-7 seconds • 3-5 times MET Venus Pagare5/5/2014
- 12. Reciprocal Inhibition When one muscleis contracted, itsantagonist is automaticallyinhibited. MET Venus Pagare5/5/2014
- 13. Types of contractions in MET • Isometric contraction : hypertonicshortened muscle • Isotonic contraction : inhibited weakened muscles –Concentric contraction: mobilizea joint against its motion barriers –Eccentric contraction –Isolytic contraction : fibrosed muscle MET Venus Pagare5/5/2014
- 14. • During an isometric contraction, distancebetween origin and the insertionof muscle is maintained at a constantlength. • A fixed tension developsin muscleas patient contractsmuscleagainst an equal counterforce applied by operator • Preventingshortening of muscle from origin to insertion. MET Venus Pagare5/5/2014
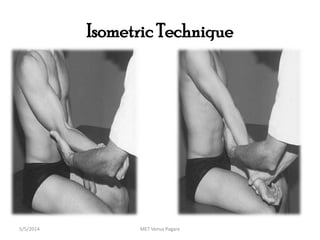
- 15. Isometric Technique MET Venus Pagare5/5/2014
- 16. • A concentricisotonic contractionoccurs when muscle tension causes origin and insertionto approximate. MET Venus Pagare5/5/2014
- 17. Isolytic • Non-physiological event • Patientattempts concentriccontractionbut an external force is applied by operatorin opposite direction • Useful in cases with marked degree of fibrotic change. MET Venus Pagare5/5/2014
- 18. • Used cautiously to lengthena severely contractured or hypertonic muscle as ruptureof musculotendinous junctionand insertionof tendon into bone or muscle fibers can occur. MET Venus Pagare5/5/2014
- 19. USES • Lengthen a shortened, contractured,or spastic muscle • Strengthen a physiologically weakened muscle /s • Reduce pain • Stretch tight fascia • Reduce localized edema • Mobilizean articulationwith restrictedmobility MET Venus Pagare5/5/2014
- 20. Elements of Muscle Energy Procedures 1. Patient : active muscle contraction 2. Controlled joint position 3. Controlled contraction intensity 4. Muscle contraction in a specific direction 5. Operator-applied distinct counterforceMET Venus Pagare5/5/2014
- 21. Guidelines • 3-5 repetitions for 7-10 secondseach • 20-50% of muscle strength • Isometric contraction should not be too hard • Aftersustained but lightcontraction, a momentary pauseshould occur • Isotonic contractions requiresforceful contraction MET Venus Pagare5/5/2014
- 22. Breathing during met • Inhale slowlyas isometric contraction buildsup • Hold the breath during 7-10 sec • Releasethe breath as they slowlyceasethe contraction • Inhale and exhale fully once more following cessationof all efforts MET Venus Pagare5/5/2014
- 23. Key points Accuratelyassesstheresistant barrier Engageeachmotionbarrier in samefashion MET Venus Pagare5/5/2014
- 24. Isometric v/s Isotonic Procedures Isometric Isotonic Careful positioning Careful positioning Lightto moderatecontraction Hardto maximalcontraction Unyieldingcounterforce Counterforcepermits controlledmotion Relaxation after contraction Relaxation after contraction Repositioning Repositioning MET Venus Pagare5/5/2014
- 25. Errors By Patient Contractionis toohard Contractinwrongdirection ContractiOnisnotsustainedfor longenough Individualdoesn’trelaxcompletely aftercontraction Startingor finishingcontractiontoohastilyMET Venus Pagare5/5/2014
- 26. Errors By Therapist Inaccuratecontrolof jointpositioninrelationto barrierto movement Counterforce : incorrectdirection Inadequate patient instructions Movingto a new joint position toosoonafter contraction MET Venus Pagare5/5/2014
- 27. Not waiting forrefractoryperiodfollowingan isometriccontraction beforemuscle can be stretched to a newresting length Not maintainingstretchpositionforappropriate period of time MET Venus Pagare5/5/2014
- 28. Successful Muscle Energy Technique Control Balance Localization MET Venus Pagare5/5/2014
- 29. MET Indications Wheneversomatic dysfunctionis presentand/orwhenever there is a need to • Normalizeabnormal neuromuscular relationships • Improve local circulationand respiratory function • Lengthenand/ornormalizerestricted/hypertonic muscles and fascia • Mobilize restricted joint(s) • Movementrestrictiondue to muscletightness • Musclehyperactivity • Acute injuries • Myofascial restricitions,muscleimbalanceMET Venus Pagare5/5/2014
- 30. MET Contraindications Appliedthoughtfully Avoidin : Fracture Severe Sprain Severe Strain Open wounds Metabolic bone or other disease eg. osteoporosis Uncooperative,unresponsive, unconscious patients or those that can not or will not follow directionsMET Venus Pagare5/5/2014
- 31. REFERENCES Greenman’s Principle of manual medicine. 4th edition. Lisa DeStefano Muscle Energy Techniques. 2nd edition. Leon Chaitow MET Venus Pagare5/5/2014