Otosclerosis
•Download as PPT, PDF•
18 likes•6,533 views

Otosclerosis is a metabolic bone disease that causes abnormal bone growth in the ossicles of the middle ear, commonly fixing the stapes bone. It most often presents between ages 15-45 and risk factors include family history and metabolic abnormalities. Symptoms include hearing loss and tinnitus. Diagnosis involves audiometry, otoscopic examination, and CT scan. Treatment options include stapedotomy or stapedectomy surgery as well as hearing aids or fluoride therapy for non-surgical candidates or those who decline surgery. The goal of treatment is to restore hearing by improving sound conduction through the middle ear.
Report
Share


















Otosclerosis
- 1. OtosclerosisOtosclerosis Mr. Ashok bishnoiMr. Ashok bishnoi Lecturer JINRLecturer JINR
- 2. Definition:-Definition:- It is metabolic bone disease ofIt is metabolic bone disease of the ossicles in which normalthe ossicles in which normal bone is replaced by abnormalbone is replaced by abnormal “spongy bone” causing fixation“spongy bone” causing fixation of the stapes bone.of the stapes bone.
- 3. Incidence:-Incidence:- AgeAge The incidence of otosclerosis increases withThe incidence of otosclerosis increases with age.age. The most common age group presenting withThe most common age group presenting with hearing loss from otosclerosis is 15-45 years,hearing loss from otosclerosis is 15-45 years,
- 4. EtiologyEtiology . Unknown. Unknown Risk factors-Risk factors- Family historyFamily history Metabolic, enzyme abnormalatyMetabolic, enzyme abnormalaty Infectious, virus was identified in theInfectious, virus was identified in the lesionlesion AutoimmuneAutoimmune,,
- 5. PathophysiologyPathophysiology Due to etiological factorsDue to etiological factors Distruction of normal bone release enzymesDistruction of normal bone release enzymes Vestibular & cochlear function impairmentVestibular & cochlear function impairment CalcificationCalcification(deposition of calcium in the tissue)(deposition of calcium in the tissue) Fixation of stapes boneFixation of stapes bone Immobilization of footplate in oval window
- 6. Clinical manifestation:-Clinical manifestation:- Hearing lossHearing loss Schwartz’s signSchwartz’s sign (Normal appearing tympanic membrane(Normal appearing tympanic membrane (a pink colour is noted through the tympanic membrane)(a pink colour is noted through the tympanic membrane) Absent acoustic reflexAbsent acoustic reflex TinitusTinitus Quiet well modulated voiceQuiet well modulated voice
- 7. Diagnostic evaluation:-Diagnostic evaluation:- HistoryHistory Physical examinationPhysical examination Schwartze sign is observed in 10% ofSchwartze sign is observed in 10% of patients).patients). Rinne test: negativeRinne test: negative Weber test:Weber test: AudiometryAudiometry Otoscopic examinationOtoscopic examination
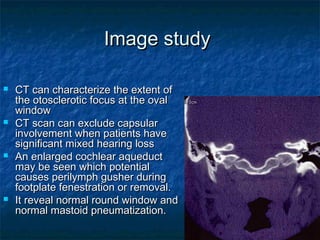
- 8. Image studyImage study CT can characterize the extent ofCT can characterize the extent of the otosclerotic focus at the ovalthe otosclerotic focus at the oval windowwindow CT scan can exclude capsularCT scan can exclude capsular involvement when patients haveinvolvement when patients have significant mixed hearing losssignificant mixed hearing loss An enlarged cochlear aqueductAn enlarged cochlear aqueduct may be seen which potentialmay be seen which potential causes perilymph gusher duringcauses perilymph gusher during footplate fenestration or removal.footplate fenestration or removal. It reveal normal round window andIt reveal normal round window and normal mastoid pneumatization.normal mastoid pneumatization.
- 9. Differential diagnosisDifferential diagnosis Ossicular discontinuityOssicular discontinuity conductive loss of 60 db usually withoutconductive loss of 60 db usually without sensorineural componentsensorineural component flaccid tympanic membrane on pneumaticflaccid tympanic membrane on pneumatic otoscopyotoscopy type Ad tympanogramtype Ad tympanogram
- 10. Differential diagnosisDifferential diagnosis Congenital stapes fixationCongenital stapes fixation Family history less likely (10%)Family history less likely (10%) usually detected in the first decade of lifeusually detected in the first decade of life 25% incidence of other congenital anomalies25% incidence of other congenital anomalies (3% for juvenile otosclerosis)(3% for juvenile otosclerosis) non-progressive CHLnon-progressive CHL
- 11. Differential diagnosisDifferential diagnosis Malleus head fixationMalleus head fixation when congenital, associated with otherwhen congenital, associated with other stigmata (aural atresia)stigmata (aural atresia) presence of tympanosclerosispresence of tympanosclerosis pneumatic otoscopypneumatic otoscopy almost always associated with type Asalmost always associated with type As tympanogram (only in advanced otosclerosis)tympanogram (only in advanced otosclerosis)
- 12. Differential diagnosisDifferential diagnosis PagetPaget’’s diseases disease - diffuse involvement of the bony skeleton- diffuse involvement of the bony skeleton - elevated alkaline phosphatase- elevated alkaline phosphatase - CT - diffuse, bilateral, petrous bone involvement- CT - diffuse, bilateral, petrous bone involvement with extensivewith extensive -de-mineralization-de-mineralization - More commonly crowds the ossicles in the- More commonly crowds the ossicles in the epitympanum, partially fixingepitympanum, partially fixing the ossicular chainthe ossicular chain
- 13. Differential diagnosisDifferential diagnosis Osteogenesis imperfectaOsteogenesis imperfecta presence of blue sclerapresence of blue sclera h/o of multiple bone fracturesh/o of multiple bone fractures CTCT –– more common involves the otic capsulemore common involves the otic capsule and to a greater extentand to a greater extent
- 14. Surgical interventionsSurgical interventions The best surgical candidateThe best surgical candidate good health with a socially unacceptablegood health with a socially unacceptable ABG,ABG, a negative Rinne test,a negative Rinne test, excellent discrimination,excellent discrimination, the desire for surgery after an appropriatethe desire for surgery after an appropriate period of time for deliberation.period of time for deliberation. Younger patients are more likely to developYounger patients are more likely to develop re-ossification of the stapes footplate overre-ossification of the stapes footplate over their lifetime.their lifetime.
- 15. Surgical interventionsSurgical interventions Most authors discourage performingMost authors discourage performing stapes surgery in patients with Meniere'sstapes surgery in patients with Meniere's disease, especially when it is active.disease, especially when it is active.
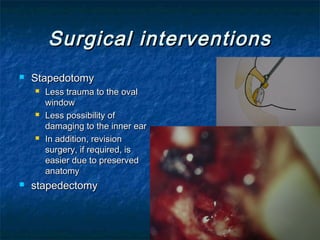
- 16. Surgical interventionsSurgical interventions StapedotomyStapedotomy Less trauma to the ovalLess trauma to the oval windowwindow Less possibility ofLess possibility of damaging to the inner eardamaging to the inner ear In addition, revisionIn addition, revision surgery, if required, issurgery, if required, is easier due to preservedeasier due to preserved anatomyanatomy stapedectomystapedectomy
- 18. Non-surgical interventionsNon-surgical interventions Amplification:Amplification: hearing aidehearing aide Patients who do not want to undergo surgeryPatients who do not want to undergo surgery for otosclerosisfor otosclerosis patients who are not fit for surgery.patients who are not fit for surgery.
- 19. Non-surgical interventionsNon-surgical interventions Medical treatment:Medical treatment: Usual dose is about 20-120mg of fluoride a dayUsual dose is about 20-120mg of fluoride a day Efficacy of the treatment can be evaluated 2 yearsEfficacy of the treatment can be evaluated 2 years later.later. SchwartzeSchwartze’’s sign, and the degree of tinnitus and imbalances sign, and the degree of tinnitus and imbalance are reassessed, and a CT scan is repeated.are reassessed, and a CT scan is repeated. Once the disease was stable, the patient is placed onOnce the disease was stable, the patient is placed on a life-ling maintenance dose of about 25mg of fluoridea life-ling maintenance dose of about 25mg of fluoride a day.a day. 50% of patients have stabilization of their disease,50% of patients have stabilization of their disease, 30% improve, and the rest continue to progress.30% improve, and the rest continue to progress.
- 20. Non-surgical interventionsNon-surgical interventions Indications for medical treatmentIndications for medical treatment Not surgical candidates,Not surgical candidates, Decide against surgery,Decide against surgery, Patient with SNHL or vestibular symptomsPatient with SNHL or vestibular symptoms positive Schwartzepositive Schwartze’’s sign may be given fluorides sign may be given fluoride treatments for 6-12 months prior to surgery to inducetreatments for 6-12 months prior to surgery to induce the focus to mature and potentially prevent thethe focus to mature and potentially prevent the progression of disease after surgery.progression of disease after surgery. determined to be active during surgery, postoperativedetermined to be active during surgery, postoperative treatment can be initiated.treatment can be initiated.