
































RADIAL NERVE PALSY AND TENDON TRANSFER
- 1. RADIAL NERVE PALSY AND TENDON TRANSFERS PRESENTED BY: DR. N. BENTHUNGO TUNGOE, PG(M.S ORTHOPEDICS), CENTRAL INSTITUTE OF ORTHOPEDICS, VMMC & SJH, NEW DELHI
- 2. Basic Functions of the hand. A, Grasp. B, Side pinch (key pinch). C, Tip pinch. D, Chuckpinch. E, Hook. F, Paperweight.
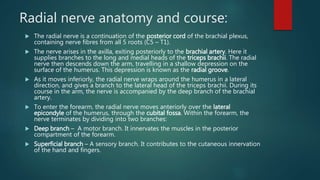
- 3. Radial nerve anatomy and course: The radial nerve is a continuation of the posterior cord of the brachial plexus, containing nerve fibres from all 5 roots (C5 – T1). The nerve arises in the axilla, exiting posteriorly to the brachial artery. Here it supplies branches to the long and medial heads of the triceps brachii. The radial nerve then descends down the arm, travelling in a shallow depression on the surface of the humerus. This depression is known as the radial groove. As it moves inferiorly, the radial nerve wraps around the humerus in a lateral direction, and gives a branch to the lateral head of the triceps brachii. During its course in the arm, the nerve is accompanied by the deep branch of the brachial artery. To enter the forearm, the radial nerve moves anteriorly over the lateral epicondyle of the humerus, through the cubital fossa. Within the forearm, the nerve terminates by dividing into two branches: Deep branch – A motor branch. It innervates the muscles in the posterior compartment of the forearm. Superficial branch – A sensory branch. It contributes to the cutaneous innervation of the hand and fingers.
- 4. MOTOR BRANCHES: The radial nerve innervates muscles located in the arm and forearm. In the arm, it directly innervates the three heads of the triceps brachii. This muscle performs extension at the elbow. In the forearm, the deep branch of the radial nerve innervates the muscles in the posterior compartment of the forearm. These muscles generally extend at the wrist and finger joints.
- 5. Muscles supplied by radial nerve
- 6. SENSORY BRANCHES: There are four branches of the radial nerve that provide cutaneous innervation to the skin of the upper limb: Lower lateral cutaneous nerve of arm – Innervates the lateral aspect of the upper arm, below the deltoid muscle. Posterior cutaneous nerve of arm – Innervates the posterior surface of the upper arm. Posterior cutaneous nerve of forearm – Innervates a strip of skin down the middle of the posterior forearm. Superficial branch of the radial nerve – Innervates the dorsal surface of the lateral three and half digits, and their associated palm area
- 8. RADIAL NERVE EXAMINATION: 1.Triceps muscle (C6-C8) assessment: Have the patient place the upper arm parallel to the ground, which eliminates the effect of gravity. Starting with the forearm half-extended, support the limb at the elbow and instruct the patient to fully extend the forearm against resistance.
- 9. 2. Brachioradialis (C5, C6) assessment: The patient flexes at the elbow with the forearm halfway between pronation and supination. Ask the patient to flex against resistance. With contraction, the brachioradialis muscle becomes prominent in the lateral antecubital fossa, where it can be observed and palpated.
- 10. 3. Extensor carpi radialis longus (C6, C7) and brevis (C7, C8) assessment: These two muscles are assessed together by having the patient extend and abduct (bend radially) the hand against resistance. With the arm pronated, contraction of these muscles can be seen lateral to the brachioradialis.
- 11. 4. Supinator (C6, C7) assessment: The supinator should be tested with the forearm extended, to minimize substitution by the biceps brachii. The patient maintains the forearm in supination as you attempt to pronate it.
- 12. 5. Extensor carpi ulnaris (C7, C8) assessment: Test by stabilizing the distal forearm and having the patient extend and adduct (bend in an ulnar direction) the hand. This muscle’s tendon at the wrist’s edge can be seen and felt.
- 13. 6. Extensor digitorum communis (C7, C8) assessment: each finger is extended at the knuckle joint with the forearm and hand well supported in a neutral position. Resistance is applied just proximal to the proximal interphalangeal joint.
- 14. 7. Extensor digiti minimi (C7, C8) assessment: This muscle acts in similar fashion as the extensor digitorum communis, yet only upon the fifth digit. The fifth digit is extended at the metacarpal–phalangeal joint while its distal interphalangeal joints are relaxed in flexion.
- 15. 8. Abductor pollicis longus (C7, C8) assessment: This muscle abducts the thumb in a radial direction (in the plane of the palm), unlike the median innervated abductor pollicis brevis, which controls palmar abduction of the thumb. test the abductor pollicis longus by stabilizing the hand and having the patient move an extended thumb away from the index finger in the plane of the palm.
- 16. 9. Extensor pollicis longus (C7, C8) assessment: Thumb extension is best assessed with the hand as a fist, resting on its ulnar surface. The thumb is extended away from the other fingers, as if the patient is hitchhiking. Resistance is applied to the distal phalange to assess the extensor pollicis longus muscle.
- 17. 10. Extensor pollicis brevis (C7, C8) assessment: Thumb extension is best assessed with the hand as a fist, resting on its ulnar surface. The thumb is extended away from the other fingers, as if the patient is hitchhiking. Resistance is applied to the proximal phalange to assess the extensor pollicis brevis muscle.
- 19. Radial nerve palsy: clinical features The patient loses the ability to extend the wrist, fingers and thumb, movements that are essential for functional grasp. In addition, the patient loses grip strength because he cannot stabilize the wrist during power grip. Fortunately, the loss of cutaneous sensibility in the radial nerve distribution is well tolerated. A high radial nerve palsy is defined as an injury proximal to the elbow. Wrist, finger (MCPJ), and thumb extension, as well as thumb abduction are lost. Low radial nerve palsy, defined as an injury to the PIN, occurs distal to the elbow. Wrist extension is preserved because the more proximally innervated ECRL remains intact. If the PIN is injured proximally, ECU function may be lost, resulting in radial deviation with wrist extension. If the injury to the PIN is more distal, ECU function is preserved and wrist extension remains balanced.
- 20. Causes:
- 23. Tendon transfer: radial nerve palsy There are three main goals when treating radial nerve palsy. restoration of finger (MCPJ) extension, restoration of thumb extension, and in cases of high radial nerve palsy, restoration of wrist extension.
- 25. Wrist extension: The most accepted method for restoring wrist extension after high radial nerve injury is the PT to ECRB transfer. If recovery of the radial nerve is not expected, the transfer should be performed in an end-to-end fashion, meaning that the ECRB tendon is transected and the cut end of the PT tendon sutured to it (Figure 1). This creates a direct line of pull, and a more efficient transfer. However, if the radial nerve has been repaired and ECRB reinnervation is expected in the future, the transfer should be performed in an end-to-side fashion, with the cut PT tendon sutured to the side of the intact ECRB tendon (Figure 2). If performed early, this transfer acts as an internal splint that stabilizes the wrist while the nerve is recovering. Because the ECRB is left intact, it can resume wrist extension once it regains function.
- 27. Thumb extension Many different tendons can be transferred to the EPL to restore thumb extension. The palmaris longus (PL) or the ring finger flexor digitorum superficialis (FDS) are used most often. When the ring FDS is used, it can be split and inserted into both the EPL and the EIP, allowing concomitant thumb and index finger extension. Although this transfer seems to violate the principle of using a single tendon to perform a single movement, in reality it does not. Concomitant thumb and index finger extension is a composite movement that is useful in precision manipulation, and can be considered a single function. When the PL is used as a motor, the EPL is usually rerouted volarly to meet the PL in a direct line of pull. This results in abduction of the thumb as well as IPJ extension.
- 29. Finger MCP extension: Finger MCPJ extension can be re-established by transferring the FCR, FCU or FDS tendon to the EDC. In the early 1900’s, Jones popularized the used of the FCU to restore MCPJ extension. However, there are a number of drawbacks to using the FCU. For one, it sacrifices the only remaining ulnar-sided wrist motor. This results in radial deviation of the wrist, particularly in cases of low radial nerve palsy in which the ECRL remains intact. In addition, ulnar deviation with wrist flexion is lost when the FCU is sacrificed. This is an important wrist motion, and is essential for activities such as hammering and throwing. For these reasons, the FCR (Brand) and FDS (Boyes) transfers are also often used. Neither the FCR nor the FDS transfer results in radial deviation of the wrist or loss of ulnar deviation with wrist flexion. In addition, the FDS transfer has the advantage of having better excursion than the other two transfers. The main disadvantage of the FDS transfer is that powering MCPJ extension with a finger flexor is not synergistic, and motor re-education after the transfer is difficult.
- 31. Other techniques: The ring finger FDS is transferred to the EPL and EIP to provide thumb and index finger extension. The middle finger FDS is used to power the EDC to all four fingers, restoring finger extension. Merle d’Aubigne procedure. It involves a PT to ECRB (and ECRL) transfer. The FCU is used to power the EPL and EDC together. In addition, the PL is transferred to the EPB and APL to provide thumb abduction
- 32. Others:
- 33. Post op rehabilitation: the patient should be placed in an above elbow splint or cast postoperatively. The elbow should be flexed at ninety degrees, the forearm pronated, and the wrist extended at thirty degrees. This takes tension off the PT to ECRB transfer. The thumb should be abducted and extended, and the MCPJ’s of the fingers extended, to take tension off the transfers to the EDC and the EIP. The IPJ’s of the fingers should be left free. During the first four weeks after surgery, it is important to maintain range of motion of the shoulder and the IPJ’s of the fingers. At four weeks mobilization begins. During weeks four to six, exercises will focus on mobilization of single joints, while keeping tension off the transfer. Avoid simultaneous flexion of the wrist and fingers, so as not to place excessive tension on the transfers At eight weeks postoperatively, strengthening exercises are begun, and the splint can be weaned off. Full activity is resumed at twelve weeks.1