



































SIMTEGR8: Simulation To Evaluate Great Care
- 1. Simulation to Evaluate Great Care (SIMTEGR8) Assessing the impact of Better Care Fund interventions on emergency admissions Cheryl Davenport Director of Health and Care Integration Leicestershire County Council Claire Cordeaux Director of Health and Social Care SIMUL8 Corporation
- 2. National Context • Policy Implementation : Better Care Fund (BCF) A pooled budget between NHS and Local Authority Partners Mandated from 2015 Designed to promote joining up care pathways between health and social care. Targeted to reducing hospital admissions, improving hospital discharge, and providing more integrated care in the community Impact assessed against national metrics High level of political expectation and scrutiny
- 3. £77,000 awarded via University’s EPG Reduce Emergency admissions by 3.5% 1-year Evaluation Project Conducted Outputs inform commissioning intentions and models of care for BCF schemes for 2016/17 Local Response to National Context
- 4. Local Context: Leicestershire • Commitment to independent evaluation of BCF, one of the first places in the country to do so • Innovative local partnership led to successful grant application at LU • Dedicated resource to undertake the evaluation • Supported by Programme Board and Advisory Panel • Methodology involves developing and testing a simulation of the pathway, assessing the impact of 4 new integrated care pathways, recommending further opportunities for improvement - both in terms of systems improvement and service user experience • SIMTEGR8 findings along with clinical audits have informed commissioning intentions for integrated care for 2016/17
- 5. Evaluation Study: Purpose • Evaluate how emergency admissions to hospitals can be reduced • Help Improve the patient journey through new integrated interventions
- 6. Description of the 4 Emergency Admissions Interventions Evaluated Older Persons Unit (OPU) • The OPU provides GPs and other health care professionals such as EMAS and ED staff with an alternative method of obtaining a comprehensive geriatric assessment as opposed to admission to the acute sector for patients who are perceived as being pre-hospital admission. Nursing homes can also make direct referrals to the OPU. • The service offers clinical assessment and support which is initially provided by an Advanced Nurse Practitioner specialising in older people and a Consultant Geriatrician. • At the unit, the patient receives a comprehensive geriatric assessment including diagnostic testing such as bloods and x-rays. Patients requiring further diagnostics such as ultrasound will be referred as appropriate. • The service is available Monday to Friday – 9am-5pm (excluding bank holidays)
- 7. Description of the 4 Emergency Admissions Interventions Evaluated Integrated Crisis Response Service 24/7– Overnight Nursing • Leicestershire Partnership Trust’s (LPT’s) enhanced Overnight Nursing Assessment Service provides four virtual beds and a roving night team, providing home visits, and overnight support in patients’ own homes. • The service complements existing Community Health Services unscheduled care and social care crisis response services to provide 24-hour unscheduled care. • It incorporates nursing assessment and therapeutic intervention, including the identification and management of low-level social care needs to ensure patients are safe at home. • The service is available seven nights a week from 10pm to 8am and is a fully integrated part of LPT’s community health services so that the needs of patients are met over 24 hours. It operates across Leicestershire County and Rutland and is available to patients registered with a Leicestershire County or Rutland GP.
- 8. Description of the 4 Emergency Admissions Interventions Evaluated Rapid Response Falls Service • A comprehensive non-conveyance pathway whereby potential admissions due to falls are assessed by paramedics on scene, using a Falls Risk Assessment Tool (FRAT). • If further follow up is needed urgently in the home, but the patient does not need conveying to hospital the paramedics have dedicated referral pathways to local Integrated Crisis Response team for community nursing and social care support.
- 9. Description of the 4 Emergency Admissions Interventions Evaluated 7 day Services in Primary Care • During 2015/16 the 2 CCGs in Leicestershire piloted 7 day services for specific cohorts of patients. • Models of care included acute visiting in the home and appointment based services at specific primary care facilities • Due to the pilot nature of this work, and evaluation processes in GP practice, some of the models were adjusted in year, as well as informing a fundamental review of how to approach this in 2016/17 onwards.
- 10. Project Governance • Local Project Board, Partnership Collaboration Agreement • Roles: LU - researcher resource, academic oversight, production of evaluation report Healthwatch – patient experience workshops, testing simulation models with users LCC – SRO level project support, facilitation of stakeholder workshops links with BCF plan and project leads SIMUL8 – simulation modelling support, resources and training All – supported general project management, admin, comms and dissemination.
- 11. Advisory Board of Regional/National Experts: • East Midlands Regional lead for the National Institute for Health and Care Excellence • Member of the Better Care Fund National Policy Team (NHS England/Local Government Association) • Academic Adviser from Swansea University • GP Clinical Adviser from West Leicestershire CCG • Head of Research - Leicestershire Partnership Trust
- 12. Other aspects of evaluation • The Leicestershire Integration Programme has a number of other elements of evaluation in progress e.g. Clinical Audits for the 4 original emergency admissions schemes – testing the appropriateness of the referral for the pathway and the definition of the avoided admission. FAME and ROSPA– testing the effectiveness of falls prevention programme/clinics Independent evaluation of Local Area Coordination
- 14. Example: Night Nursing Service • Proposed change • The (stakeholder) simulation model • Running the workshops • Patient/carer simulation model
- 15. Purpose of Workshops • Evaluate how emergency admissions to hospitals can be reduced • Help Improve the patient journey through new integrated interventions
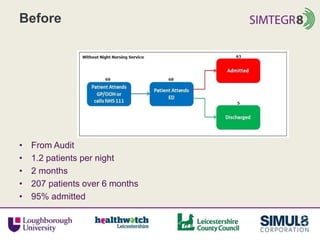
- 16. Before
- 17. Before • From Audit • 1.2 patients per night • 2 months • 207 patients over 6 months • 95% admitted
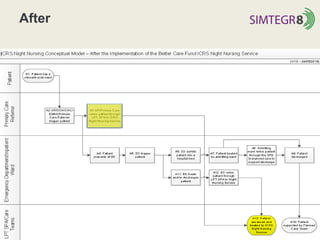
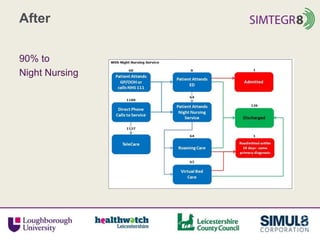
- 18. After
- 20. The (Stakeholder) Simulation Model
- 21. Running the Stakeholder Workshop • Model understanding – what is the model doing? • Face validation – is the model depicting reality? • Problem scoping – what is causing problems? • Improvement – identifying and testing improvements
- 22. The Patient/Carer Simulation Model
- 23. Aims of Methodology • Generate discussion about Model Pathway Reality Metrics • Identify issues • Resolve issues
- 24. Methodology Overview • Simple models will be used in a facilitated workshop environment. Adapted from SimLean Facilitate (Robinson et al 2014) Conceptual Modelling Rapid Model Development Facilitation (Stakeholders) Facilitation (Users)
- 25. Facilitation Workshops Workshop Intervention Date Stakeholder Workshop 1 Integrated Crisis Response, Night Nurses 11/9/15 Stakeholder Workshop 2 Older Persons Unit 11/9/15 Stakeholder Workshop 3 7-day services in Primary Care 29/10/15 Stakeholder Workshop 4 Falls 29/10/15 User Workshop 1 Older Persons Unit 10/11/15 User Workshop 2 Night Nurses 10/11/15 User Workshop 3 Falls 2/02/2016
- 26. Process Maps • Use “before” and “after” • Mostly accurate • Some changes needed – patient entry point – multi-service • Simplified versions useful
- 27. Telling the Patient Story • Simulation designed to tell “before” and “after” story of a patient • The visual display of the simulations changed to improve participant engagement
- 28. Issues Identified • Known unknowns Metrics/ data • Referrals Lack of knowledge Self referral (OPU) • Inclusion of other services Social Services, therapy, Mental Health • Other existing shortcuts Patient care plans • Geography Access to service Differences
- 29. Solutions suggested • Collect data from Single Point of Access Individually Together • Publicise Leaflets, presentations, simplify, training • Collaborate
- 30. Known Unknowns • Current Performance Metrics Currently the only consistently collected metrics are those of the SUSD Dashboard (revolving around the key metric of avoided admissions) • Potential New Metrics Consistently recorded patient outcomes (where they left the healthcare system, their journey to get there and the circumstances of them leaving) Metrics that record time spent in the system – this would allow comparison to national and local averages for similar cohorts of patients
- 31. Known Unknowns • Potential New Metrics Metrics for recording the number of movements within the system, indicating that a patient is not finding the care that they require when they require it • Patient satisfaction metrics that can be measured against the quantitative performance metrics to ensure that an improvement of a metric, such as cost or time, is not coming at the detriment to the patient experience • Any patient satisfaction metrics would need careful consideration to their collection, as this has proved impractical after the event
- 32. User Satisfaction What to measure • Simplicity of experience • Attention to patient comfort, physical and environmental • Timeliness • Times unable to access • Time with patient • Reliability of attendance • Quantity of referrals • Quantity of points of access • Confidence in clinicians • Respect for dignity of patient • Clarity of information • Patient satisfaction with outcomes • Possible choices for patient • Simple, comfortable experience • Effective use of time • Usage of service • Care and consideration • Adherence to patient wishes
- 33. How to measure it
- 34. We met our aims • Generate discussion about Model Pathway Reality Metrics • Identify issues Resolve issues
- 35. Lessons for Engaging User Perspective • What we could have be done differently for capturing service user experience include the following: 1. Early engagement and buy in with Scheme Leads from the outset of the project – would have helped in identifying relevant users. 2. Different approaches to engage frail, elderly patients with complex needs using each of the schemes – cohort of patients difficult to engage as outlined in the methodology and this proved to be a challenge in the timescales. 3. Consideration that patient perspective could include both service user and expert patient voice – independent and informed patient insight is valuable.
- 36. How have the findings been applied to the models of care and commissioning intentions • Immediate findings and recommendations by pathway shared with Integration Operational group, including providers, ahead of final evaluation report being produced. • The existing action plan for the delivery of the 4 schemes in 2015/16 was updated with immediate actions that could be applied from the evaluation work and pathway models • Report to UHL Exec Team – December 2016 to highlight the impact of the pathways so far and what the emerging evaluation findings were • Medium term changes, such as further service redesign and associated commissioning decisions (e.g. future role of the OPU, future models for 7 day services) were considered as part of BCF refresh December 2015 – March 2016.
- 37. What is our approach for phase 2? • Using national and regional BCF funding we are embarking on phase 2 of the our SIMTEGR8 evaluation programme starting 1/8/16 • Resource available is £70k • Project approach and methodology will be adjusted based on lessons learned from Phase 1 • Dedicated project management support 2 days per week from LCC • Approach to patient experience and methodology for stakeholder workshops will be refreshed. • Max of 4 pathways will be evaluated 2 will be admissions avoidance (a cardio/respiratory pathway at Glenfield hospital, and an urgent care vanguard scheme) 1 will be discharge related (intensive community support in the home) 1 will be prevention related (our new integrated housing offer – called t “Lightbulb”)
- 38. Dissemination Plan • Online resources, including simulation models, to support wider adoption and sustain the learning • Application of the methodology to other parts of the Leicestershire integration programme • Application of the methodology to other integration programmes regionally and nationally • Dissemination Routes to include: BCF network – regional, national, Better Care Exchange SIMUL8 webinar 29th July Healthwatch organisations regionally/nationally Health and Wellbeing Boards regionally/nationally Academic networks, publications, conference. Social media/other communication channels
- 39. Website, Handbooks and Support • Website: Our test site is currently at this address: http://simtegr8.wix.com/simtegr8v2 -the final site address will be circulated once launched • View handbooks and models on the website • Enquiries and Support: simtegr8@lboro.ac.uk
- 40. SIMTEGR8 Project Board Contacts @SIMTEGR8 Professor Stewart Robinson Dean, School of Business and Economics, University of Loughborough S.L.Robinson@lboro.ac.uk Professor Zoe Radnor Dean, School of Business, University of Leicester zjr1@leicester.ac.uk Vandna Gohil Director, Healthwatch Leicestershire vandna.g@healthwatchleics.co.uk Cheryl Davenport Director, Health and Care Integration, Leicestershire County Council cheryl.davenport@leics.gov.uk Claire Cordeaux Executive Director, Health and Social Care, SIMUL8 Corporation Claire.C@SIMUL8.com