



















































The ankle and foot complex
- 2. Ankle/foot complex is structurally analogous to the wrist- hand complex of the upper extremity. Primary role to bear weight. The structures of the ankle/foot complex permit both stability and mobility depending on conditions acting on it.
- 4. Stability • It provide adequate BOS and function as rigid lever for pushing-off during walking, running, or jumping.
- 5. Mobility • it must also be mobile to adapt to uneven terrain, absorb shock as the foot hits the ground.
- 6. Total 26 foot bones, which functionally divided into 3; Forefoot (anterior) • Metatarsals - 5 • Phalanges - 14 Midfoot (middle) • Navicular - 1 • Cuboid - 1 • Cuneiform – 3 Hindfoot (posterior) • Talus – 1 • Calcaneus - 1
- 8. 25 component joints • Proximal and distal tibiofibular joints – 1-1 • Ankle (talo – crural) joint - 1 • Talo – calcaneal (subtalar) joint - 1 • Talo – navicular joint - 1 • Calcaneo – cuboidal joint - 1 • Tarso – metatarsal joints - 5 • Metatarso – pharangeal joints - 5 • Inter – phalangeal joints - 9
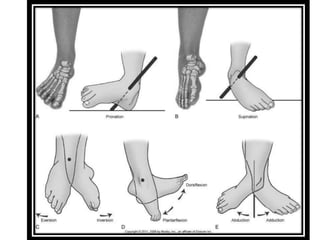
- 9. Three cardinal motions : • Dorsiflexion / Plantarflexion • Inversion / Eversion • Abduction / Adduction
- 10. Plane : Sagittal plane Axis : Coronal axis Dorsiflexion decreases the angle between the leg and the dorsum of the foot, whereas Plantarflexion increases this angle. At the toes, motion around a similar axis is termed extension (bringing the toes up), whereas the opposite motion is flexion (bringing the toes down or curling them).
- 11. Plane : Frontal plane Axis : longitudinal (anteroposterio A-p)axis Inversion occurs when the plantar surface of the segment is brought toward the midline; eversion is the opposite.
- 12. Plane : transverse plane Axis : vertical axis Abduction is when the distal aspect of a segment moves away from the midline of the body (or away from the midline of the foot in the case of the toes); adduction is the opposite.
- 15. Pronation / Supination Pronation/supination in the foot are motions that occur around an axis that lies at an angle to each of the axes for “cardinal” motions. Consequently, pronation and supination are terms used to describe “composite” motions that have components of, or are coupled to, each of the cardinal motions. Pronation = dorsiflexion, eversion, and abduction. Supination = plantarflexion, inversion, and adduction.
- 17. Valgus refers to an increase in the medial angle between two bones varus refers to the opposite. Valgus (calcaneovalgus) : an increase in the medial angle between the calcaneus and posterior leg. Varus (calcaneovarus) : an decrease in the medial angle between the calcaneus and posterior leg.
- 19. Talocrural joint. Articulation Proximal : Distal tibia and fibula Distal : Body of talus Hinge synovial joint with a joint capsule and associated ligaments. It have a single oblique axis with one degree of freedom around which the motion of dorsiflexion / plantarflexion occur.
- 22. Proximal articular surfaces • Concave surface of the distal tibia and of the tibial and fibular malleoli. • These three facets form an almost continuous concave joint surface that extends more distally on the fibular (lateral) side than on the tibial (medial) side and more distally on the posterior margin of the tibia than on the anterior margin. • Distal most aspect of fibula known as lateral malleolus. • Distal tibia and both malleoli resembles and is referred to as a mortise.
- 24. A common example of a mortise is the gripping part of a wrench. Either the wrench can be fixed (fitting a bolt of only one size) or it can be adjustable (permitting use of the wrench on a variety of bolt sizes). The adjustable mortise is more complex than a fixed mortise because it combines mobility and stability functions.
- 25. The mortise of the ankle is adjustable, relying on the proximal and distal tibiofibular joints to both permit and control the changes in the mortise. The proximal and distal tibiofibular joints are anatomically distinct from the ankle joint, but functionally likned to the ankle. Unlike their upper extremity counterparts, the proximal and distal radioulnar joints, the tibiofibular joints do not add any degrees of freedom to the more distal ankle and foot joints. However, fusion of the radioulnar joints would have little effect on wrist range of motion (ROM), whereas fusion of the tibiofibular joints may impair normal ankle function.
- 26. Plane synovial joint. Articulation : head of the fibula with the posterolateral aspect of the tibia. A slight convexity of the tibial facet and a slight concavity of the fibular facet. Each proximal tibiofibular joint is surrounded by a joint capsule that is reinforced by anterior and posterior tibiofibular ligaments. Motion : very small, superior and inferior translation and rotation of fibula.
- 29. syndesmosis, or fibrous union. Articulation : concave facet of the tibia and the convex facet of the fibula. The distal tibia and fibula do not actually come into contact with each other but are separated by fibroadipose tissue. Although there is no joint capsule, there are several associated ligaments at the distal tibiofibular joint.
- 31. Function : • Maintain a stable mortise. • Support distal tibiofibular joint. 3 ligaments • Anterior tibiofibular ligament • Posterior tibiofibular ligament • Interosseous membrane The interosseous membrane directly supports both proximal and distal tibiofibular articulations.
- 32. Body of talus It has three articular surfaces: • large lateral (fibular) facet • Smaller medial (tibial) facet • Trochlear (superior) facet The large, convex trochlear surface has a central groove that runs at a slight angle to the head and neck of the talus. The body of the talus also appears wider anteriorly than posteriorly, which gives it a wedge shape.
- 33. The articular cartilage covering the trochlea is continuous with the cartilage covering the more extensive lateral facet and the smaller medial facet.
- 35. Thin and especially weak anteriorly and posteriorly. Therefore, the stability of the ankle depends on an intact ligamentous structure.
- 36. The 3 ligament that supports proximal and distal tibiofibular joint and mortise. • Anterior and posterior tibiofibular ligament • Tibiofibular interosseous ligament 2 additional ligament that maintain contact between talus and mortise and control medial-lateral joint stability. • Medial collateral ligament • Lateral collateral ligament Both of these ligaments also provide key support for the subtalar or (talocalcaneal) joint that they also cross.
- 37. Deltoid ligament Fan shaped Superficial and deep fibers Origin : borders of the tibial malleolus Insertion : • anteriorly on navicular • Distally on talus • Posterior on calcaneus
- 38. It is extremely strong ligament so injury chances are very less. Eversion and pronation of ankle and talus can injure this ligament. However, these forces may actually fracture and displace the tibial malleolus before the deltoid ligament tears.
- 40. Made up of 3 bands commonly referred to as seperate ligaments i.e; • Anterior talofibular ligament • Posterior talofibular ligament • Calcaneofibular ligament Anterior and posterior talofibular ligament runs horizontal whereas calcaneofibular ligament runs vertical.
- 41. Lateral collateral ligament control inversion and supination of ankle and talus. its weaker and more susceptible to injury than are those of the medial collateral ligament.
- 43. Superior and inferior extensor retinacula Superior and inferior peroneal retinacula Function : provide stability to ankle and subtalar joint Along with collateral ligaments. the inferior band of the superior peroneal retinaculum, which lies close and parallel to the calcaneofibular ligament, appears to reinforce that ligament.
- 45. In neutral position of the ankle joint, the joint axis passes approximately through the fibular malleolus and the body of the talus and through or just below the tibial malleolus. The fibular malleolus and its associated fibular facet on the talus are located more distally and posteriorly than the tibial malleolus and its associated tibial facet. The more posterior position of the fibular malleolus is due to the normal torsion or twist that exists in the distal tibia in relation to the tibia’s proximal plateau.
- 47. Figure A. Posterior view showing the mortise around the body of the talus and the average 14 degree inclination of the of the ankle axis from the transverse plane. Figure B. Superior view showing the ankle axis rotated, on average, 23 degree from the frontal plane.
- 48. Tibial torsion may be defined as the torsion, or twisting, between the upper and lower ends of the tibiofibular unit. This twisting may be reffered as tibial torsion or tibiofibular torsion (because both the tibia and fibula are involved with the rotation in the transverse plane) and accounts for the toe-out position of the foot in normal standing. Lateral tibial torsion increases from birth to 10 years of age.
- 49. Ankle joint is considerd to have one degree of freedom. Dorsiflexion and plantarflexion That, occurring between talus and mortise.
- 50. Dorsiflexion 10 to 20 degree Motion of the head of the talus dorsally (upward) while the body of the talus moves posteriorly in the mortise. Plantar flexion 20 to 50 degree Opposite Motion of the head and body of talus.
- 51. Talar rotation or talar abduction/adduction 7 degree medial rotation and 10 degree lateral rotation Talus may rotate slightly within the mortise in the transverse plane around a vertical axis. Talar tilt 0r talar inversion/eversion 5 degree or less Seen in the frontal plane around an A-P axis.
- 52. When the foot is weight-bearing, dorsiflexion occurs by the tibia’s rotating over the talus As the tibia rotates over the talus, the concave tibiofibular segment slides forward on the trochlear surface of the talus Therefore, the wider anterior portion of the talus “wedges” into the mortise enhancing stability of the ankle.
- 53. The loose packed position of the ankle joint is in plantar flexion. During plantar flexion, only the relatively narrow posterior body of the talus is in contact with the mortise. The ankle is considered to be less stable when in plantar flexion. There is a higher incidence of ankle sprains when the ankle is plantar flexed than when dorsi flexed.
- 54. The asymmetry in size and orientation of the lateral and medial facets of the ankle joint contribute to changes in the ankle mortise that occur during ankle movements. The lateral (fibular) facet is substantially larger than the medial (tibial) facet. distal fibula moving on the larger lateral facet of the talus must undergo a greater displacement than the tibial malleolus as the tibia and fibular move together during dorsiflexion. The greater arc of motion for the fibula malleolus than for the tibial malleolus results in superior/inferior motion and medial/lateral rotation of the fibula that requires mobility of the fibula at both the proximal and the distal tibiofibular joints.
- 56. Ankle dorsiflexion and plantarflexion movements are limited primarily by soft tissue restrictions. Tension in the triceps surae (gastrocnemius and soleus muscles) is the primary limitation to dorsiflexion. Dorsiflexion is more limited typically with the knee in extension than with the knee in flexion.
- 57. Tension in the tibialis anterior, extensor hallucis longus, and extensor digitorum longus muscles is the primary limit to plantarflexion. The tibialis posterior, flexor hallucis longus, and flexor digitorum longus muscles help protect the medial aspect of the ankle; the peroneus longus and peroneus brevis muscles protect the lateral aspect.