Journal of Alzheimer’s Disease 42 (2014) 1239–1250
DOI 10.3233/JAD-140405
IOS Press
1239
Depression in Mild Cognitive Impairment is
associated with Progression to Alzheimer’s
Disease: A Longitudinal Study
Stefan Van der Musselea,b , Erik Fransenc , Hanne Struyfsa , Jill Luyckxa , Peter Mariënd,e , Jos Saerensd ,
Nore Somersd , Johan Goemand , Peter P. De Deyna,d,f,g and Sebastiaan Engelborghsa,d,∗
a Reference
Center for Biological Markers of Dementia (BIODEM), Laboratory of Neurochemistry and Behavior,
Institute Born-Bunge, University of Antwerp, Antwerp, Belgium
b Department of Nursing and Midwifery Sciences, Faculty of Medicine and Health Sciences, University of Antwerp,
Antwerp, Belgium
c StatUa Center for Statistics, University of Antwerp, Antwerp, Belgium
d Department of Neurology and Memory Clinic, Hospital Network Antwerp (ZNA), Middelheim and Hoge Beuken,
Antwerp, Belgium
e Department of Clinical and Experimental Neurolinguistics (CLIN), Vrije Universiteit Brussel, Brussels, Belgium
f Department of Rehabilitation Sciences and Physiotherapy, Faculty of Medicine and Health Sciences, University
of Antwerp, Antwerp, Belgium
g Department of Neurology and Alzheimer Research Center, University Medical Center Groningen,
University of Groningen, The Netherlands
Accepted 8 May 2014
Abstract.
Background: Behavioral and psychological signs and symptoms of dementia (BPSD) belong to the core symptoms of dementia
and are also common in mild cognitive impairment (MCI).
Objective: This study would like to contribute to the understanding of the prognostic role of BPSD in MCI for the progression
to dementia due to Alzheimer’s disease (AD).
Methods: Data were generated through an ongoing prospective longitudinal study on BPSD. Assessment was performed by
means of the Middelheim Frontality Score, Behave-AD, Cohen-Mansfield Agitation Inventory, Cornell Scale for Depression in
Dementia (CSDD), and Geriatric Depression Scale 30-questions (GDS-30). Cox proportional hazard models were used to test
the hypothesis that certain BPSD in MCI are predictors of developing AD.
Results: The study population consisted of 183 MCI patients at baseline. At follow-up, 74 patients were stable and 109 patients
progressed to AD. The presence of significant depressive symptoms in MCI as measured by the CSDD (HR: 2.06; 95% CI:
1.23–3.44; p = 0.011) and the GDS-30 (HR: 1.77; 95% CI: 1.10–2.85; p = 0.025) were associated with progression to AD. The
severity of depressive symptoms as measured by the GDS-30 was a predictor for progression too (HR: 1.06; 95% CI: 1.01–1.11;
p = 0.020). Furthermore, the severity of agitated behavior, especially verbal agitation and the presence of purposeless activity,
was also associated with progression, whereas diurnal rhythm disturbances were associated with no progression to AD.
Conclusion: Depressive symptoms in MCI appear to be predictors for progression to AD.
Keywords: Alzheimer’s disease, association, BPSD, Cox proportional hazard, dementia, depression, depressive symptoms, mild
cognitive impairment, predictor, prognostic value
∗ Correspondence
to: Dr. Sebastiaan Engelborghs, MD, PhD,
University of Antwerp/Institute Born-Bunge; Reference Center for
Biological Markers of Dementia (BIODEM), Universiteitsplein 1,
BE-2610 Antwerp, Belgium. Tel.: +32 3 265 25 96; Fax: +32 3 265
26 18; E-mail: Sebastiaan.Engelborghs@uantwerpen.be.
ISSN 1387-2877/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved
This article is published online with Open Access and distributed under the terms of the Creative Commons Attribution Non-Commercial License.
�1240
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
INTRODUCTION
Mild cognitive impairment (MCI) is a clinical concept that identifies subjects who are in an intermediate
cognitive state between normal aging and dementia.
MCI is a syndrome characterized by an impairment
of memory or other cognitive decline, which does not
affect a person’s basic activities of daily living, whereas
the complex instrumental functions may be minimally
impaired. MCI can be divided into two subtypes: an
amnestic subtype with memory deficits and a nonamnestic subtype with a cognitive decline other than
memory. The subtypes can be further specified, based
on cognitive impairment in a ‘single domain’ or in
‘multiple domains’ [1, 2].
The clinical presentation, etiology, and outcome of
MCI are heterogeneous. The etiology can be neurodegenerative, vascular, metabolic, traumatic, psychiatric,
or other [1, 2]. Furthermore, patients with amnestic MCI are likely to progress to dementia due to
Alzheimer’s disease (AD) [3], whereas the outcome of
non-amnestic MCI appears to be more heterogeneous,
including vascular dementia, frontotemporal dementia,
and dementia with Lewy bodies [1]. However, not all
MCI patients progress to dementia and some recover
to normal cognition [2]. This can at least partially be
explained by the fact that elderly with depression and
cognitive symptoms were diagnosed as MCI in some
studies [4]. It is assumed that less than half of the MCI
patients develop a type of dementia and the annual
rate of MCI progression to dementia is approximately
5–10% [5]. However, the progression rate is influenced
by the MCI definition used, the MCI subtype and the
research setting [5].
Behavioral and psychological signs and symptoms
of dementia (BPSD) belong to the core symptoms of
dementia [6], but BPSD are also common in MCI with
reported prevalence ranging from 35% to 85% [7–10].
Moreover, certain BPSD are also more prevalent and
severe in MCI than in cognitively healthy older adults,
but less prevalent and severe in MCI than in AD [7].
Given the high prevalence of BPSD in MCI and AD
and given the intermediate BPSD state of MCI between
healthy older adults and AD [7], it is possible that some
of these symptoms are predictors of progression from
MCI to AD.
Therefore, large prospective longitudinal studies are
needed for improved understanding of the prognostic
value of neuropsychiatric features in MCI for the progression to dementia [9, 10]. With this study, we would
like to contribute to the understanding of the epidemiology of MCI, the diagnostic value of BPSD in MCI
and the evaluation of the prognostic role of BPSD in
MCI for the progression to AD. We hypothesize that
BPSD in MCI are predictors for the progression to AD.
MATERIALS AND METHODS
Study population and diagnostic criteria
This monocenter study included patients at the
moment of their diagnostic work-up in a tertiary care
level memory clinic. The diagnostic work-up consisted
of a general physical and neurological examination,
routine blood examination, structural neuroimaging
consisting of brain magnetic resonance imaging or, if
not feasible, brain computerized tomography, standard
electroencephalogram, the Mini-Mental State Examination (MMSE) [11], and an extensive time-linked
(±3 months) neuropsychological examination with
adjustment for gender, age, and education, comprising among others the Wechsler Memory Scale III [12],
Repeatable Battery for the Assessment of Neuropsychological Status [13], and/or Hierarchic Dementia
Scale [14].
To diagnose MCI at baseline, Petersen’s diagnostic
criteria [1] were applied, i.e., (1) cognitive complaint,
preferably corroborated by an informant; (2) objective cognitive impairment, quantified as a performance
of more than 1.5 SD below the appropriate mean on
the neuropsychological subtests; (3) largely normal
general cognitive functioning; (4) essentially intact
activities of daily living (basic and instrumental activities of daily living were determined by a clinical
interview with the patient and an informant); and
(5) not demented. As all cognitive domains of subjects were tested in an extensive time-linked (±3
months) neuropsychological examination, all MCI
patients were categorized as: an ‘amnestic’ subtype
with memory deficits or a ‘non-amnestic’ subtype with
cognitive decline other than memory; and cognitive
impairment could be present in a ‘single domain’ or in
‘multiple domains’. Patients with neurological, psychiatric, or somatic disorders that were a sufficient cause
for the cognitive complaints, such as alcohol abuse or
severe depression, were excluded. Severe depression at
baseline was defined as a Cornell Scale for Depression
in Dementia (CSDD) total score of ≥22 or a Geriatric
Depression Scale 30 questions (GDS-30) total score
of ≥21. Study participants were 55 years of age minimum and had a clinical follow-up of at least one year
or until dementia diagnosis.
In total our database contained data on 589 patients
recruited for cognitive impairment (not demented)
�S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
BPSD research purposes since 2003. After strict application of the MCI Petersen criteria, 303 patients were
eligible. From this cohort, 235 MCI patients met the
study criteria. Only 5 subjects dropped out due to
the criterion ‘severe depression at baseline’. Two of
them remained non-amnestic single domain MCI over
time, one subject normalized, one progressed to frontotemporal lobar degeneration and only one patient
progressed to AD. To diagnose probable AD at followup, the NINCDS/ADRDA criteria [15] were used,
though all patients also fulfilled the DSM-IV-TR criteria [16]. Clinical and neuropsychological follow-up of
included patients and autopsy in deceased patients during follow-up who consented [17], further contributed
to the diagnostic accuracy of the subjects in this study.
Staging of cognitive deterioration was assessed by
means of the Global Deterioration Scale [18]. Age at
disease onset was estimated by the clinician following an interview with the patient’s main caregiver. In
case a non-professional caregiver was not available,
the patient’s main professional caregiver was contacted
and interviewed.
The local ethics committee approved this study.
All patients and/or patients’ caregivers gave written
informed consent. All patients were of Caucasian origin.
BPSD assessment
All subjects underwent in-depth BPSD assessment
at inclusion (baseline) consisting of an interview of
both patient and caregiver, covering a period of two
weeks prior to inclusion. The battery of BPSD assessment scales comprised: Middelheim Frontality Score
(MFS), Behavioral Pathology in Alzheimer’s Disease
Rating Scale (Behave-AD), Cohen-Mansfield Agitation Inventory (CMAI), CSDD, and GDS-30.
The MFS is a validated assessment scale that measures frontal lobe features and reliably discriminates
FTD from AD patients with a sensitivity and specificity of almost 90% and with good inter- and intra-rater
reliability [19, 20]. According to the Instructions for
Administration and Scoring, the MFS was rated by the
clinician or researcher and was obtained by summating
scores in a standardized fashion on ten items. Each item
was scored either zero (absent) or one (present) yielding a total maximal score of 10. The items scored are:
(1) initially comparatively spared memory and spatial
abilities; (2) Loss of insight and judgment; (3) disinhibition; (4) dietary hyperactivity; (5) changes in sexual
behavior; (6) stereotyped behavior; (7) impaired control of emotions, euphoria or emotional bluntness; (8)
1241
aspontaneity; (9) speech disturbances such as stereotyped phrases, logorrhoea, mutism, echolalia; and (10)
restlessness. The presence of frontal lobe symptoms
in our study subjects was determined to be significant
by a discriminatory cut-off of a total MFS score of ≥5
[20].
The Behave-AD is a 25-item scale that measures
BPSD in seven clusters (Table 2), scored on a fourpoint scale of increasing severity [21]. Besides a
total score, a global score on a four-point scale of
increasing severity is provided, reflecting how troubling to the caregiver or dangerous to the patient the
BPSD are, from not troubling or not dangerous (score
0) to severely troubling or dangerous (score 3). We
dichotomized the severity scores to calculate prevalence percentages for Behave-AD clusters, total score
and global score. Within the anxieties/phobias cluster,
four types of anxiety symptoms are assessed which
include; anxiety regarding upcoming events (‘Godot
syndrome’), fear of being left alone, other anxieties and
other phobias which are each rated according to severity as outlined above. The activity disturbances cluster
includes three items; wandering away from home, purposeless activity and inappropriate activity. We found
it important to dissect these two Behave-AD clusters,
as we believed that their individual items could be of
prognostic value. It is farfetched to analyze the delusion or hallucination items, one cluster is a one-item
cluster and other clusters are, besides in the BehaveAD, thoroughly discussed in the other more specific
assessment scales.
The CMAI assesses 29 agitated behaviors on a
seven-point scale of increasing frequency (1 = never
to 7 = several times an hour) [22]. CMAI cluster scores
include aggressive behavior (10 items), physically nonaggressive behavior (11 items) and verbally agitated
behavior (8 items); a total score is provided as well.
Agitation was considered to be clinically relevant when
one or more items occurred at least once a week
(any individual item score ≥3). Aggressive, physically non-aggressive and verbally agitated behavior
was considered to be clinically relevant when one or
more items within the respective cluster occurred at
least once a week [23–29].
Depressive symptoms were assessed by means of
the CSDD and the GDS-30. The CSDD is a 19item depression scale [30]. Item scores range from
0 (absent) to 2 (severe), with a maximum total score
of 38 points. The items are clustered in five groups:
(A) mood-related signs: anxiety, sadness and lack
of reactivity to pleasant events; (B) behavioral disturbances: agitation, retardation, multiple physical
�1242
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
Table 1
Baseline population characteristics
Total n = 183
Stable MCI n = 74
Progression AD n = 109
Statistics
Male / Female
Age at inclusion (y)
Age at onset (y)
Disease duration (y)
Education (y; n = 147)
MMSE score (0–30)
Global Deterioration Scale (1–7)
77/106
74.9 ± 7.5 (55–91)
72.1 ± 7.8 (53–90)
2.7 ± 1.8 (0–14)
10.9 ± 2.6 (6–17)
26.0 ± 2.8 (18–30)
3.0 ± 0.6 (2–5)
35/39
72.0 ± 8.0 (55–88)
69.1 ± 8.3 (53–85)
2.7 ± 1.9 (0–10)
10.6 ± 2.6 (6–16; n = 68)
27.0 ± 2.5 (20–30)
3.0 ± 0.5 (2–4)
42/67
76.9 ± 6.5 (58–91)
74.1 ± 6.8 (56–90)
2.7 ± 1.8 (0–14)
11.2 ± 2.6 (6–17; n = 79)
25.3 ± 2.7 (18–30)
3.0 ± 0.6 (2–5)
p = 0.239
p < 0.001
p < 0.001
p = 0.776
p = 0.173
p < 0.001
p = 0.763
Amnestic single domain (%) (n)
Amnestic multiple (%) (n)
Non-amnestic single (%) (n)
Non-amnestic multiple (%) (n)
15.8 (29)
64.5 (118)
8.7 (16)
10.9 (20)
13.5 (10)
60.8 (45)
14.9 (11)
10.8 (8)
17.4 (19)
67.0 (73)
4.6 (5)
11.0 (12)
p = 0.476
p = 0.393
p = 0.016
p = 0.966
45.5 (30)
637.5 ± 261.2
411.9 ± 242.1
65.5 ± 30.2
17.4 (4)
823.9 ± 287.3
308.8 ± 144.2
51.8 ± 19.5
60.5 (2)
537.8 ± 182.0
465.8 ± 265.8
72.7 ± 32.5
p = 0.001
p < 0.001
p = 0.021
p = 0.014
54.9
24.0
4.5
27.3
1.1
1.7
2.2
50.7
28.8
4.1
34.2
0.0
2.7
4.1
57.8
20.6
4.8
22.3
1.9
1.0
0.9
p = 0.348
p = 0.212
p = 0.821
p = 0.080
p = 0.235
p = 0.369
p = 0.164
Pathological CSF biomarkers (%; n = 66)
Concentration A1-42 (n = 66)
Concentration T-tau (n = 67)
Concentration P-tau181P (n = 67)
Free of psychotropic medication (%)
Antidepressants (%)
Antipsychotics (%)
Hypnotics, sedatives, anxiolytics (%)
Cholinesterase inhibitors (%)
Antiparkinsonian agents (%)
Antiepileptics (%)
Data are given as ratio, percentage or mean ± SD with ranges represented between brackets. For comparison of male-female ratios and
percentages, Chi-square statistics were used. For other comparisons, Mann-Witney U test was used. The level of significance was set at
p < 0.05.
complaints and loss of interest; (C) physical signs:
appetite loss, weight loss and lack of energy; (D)
cyclic functions: diurnal variation of mood, difficulty falling asleep, multiple awakenings during sleep
and early morning awakening; (E) ideational disturbances: suicide, poor self-esteem, pessimism and
mood-congruent delusions. The presence of significant
depressive symptoms was defined by the CSDD as a
total score of >7 [31]. Studies have shown the CSDD
to be valid for screening depression in non-demented
patients too [32].
The GDS-30 is a 30-item self-rating scale developed to screen for depression in elderly people and can
also be rated, as in this study, by an interview with the
patient, even not requiring a trained interviewer [33].
The presence of significant depressive symptoms was
defined by the GDS-30 as a total score >11 [33]. The
GDS-30 is also a reliable screening tool for depressive
symptoms in MCI [34].
For optimal interpretation of our data, we mentioned
the score ranges of all assessment scales between
brackets (x-y) in Tables 2 & 3.
Cerebrospinal fluid (CSF) sampling and
biomarker analyses
Lumbar puncture, CSF sampling, and handling
have been performed according to a standard proto-
col [35]. CSF samples were stored at −80◦ C until
analysis.
CSF biomarker analyses of A1-42 , T-tau, and
P-tau181P were performed using commercially available single parameter ELISA kits (INNOTEST® ,
Fujirebio Europe, Ghent, Belgium) at the BIODEM
lab of Institute Born-Bunge/University of Antwerp as
previously described [35].
A CSF biomarker profile was considered pathological and suggestive for AD if a subject displayed
a low CSF A1-42 value in combination with an
increased T-tau and/or increased P-tau181P value
(unpublished data). In our hands, and using the commercially available INNOTEST kits (Fujirebio Europe,
Ghent), normal values are: A1-42 >638.50 pg/mL,
T-tau <296.50 pg/mL and P-tau181P <56.50 pg/mL.
These cutpoints have been determined in autopsyconfirmed AD patients as compared to cognitively
healthy elderly (unpublished data).
Statistical analyses
The BPSD assessment scales used during this study
provide semi continuous variables. The KolmogorovSmirnov test indicated that none of the used
study variables could be treated as normally distributed. Therefore, non-parametric statistics were
used: Kruskal-Wallis test and Mann-Whitney U tests
�1243
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
Table 2
Baseline prevalence and severity of BPSD
Prevalence %
Behavior/disturbances
MFS ≥5 score/total (0–10)
Frontal lobe symptoms
Behave-AD (0–21)
Delusions
Behave-AD (0–15)
Hallucinations
Behave-AD (0–36)
Psychosis
Behave-AD (0–9)
Activity
Behave-AD (0–9)
Aggressiveness
Behave-AD (0–3)
Diurnal rhythm
Behave-AD (0–6)
Affective
Behave-AD (0–12)
Anxiety/Phobias
Behave-AD (0–75)
Total score
Behave-AD (0–3)
Global score
CMAI (10–70)
Aggressive
CMAI (11–77)
Physically non-aggressive
CMAI (8–56)
Verbally agitated
CMAI (29–203)
Total score
CSDD (0–38)
>7 / total score
GDS-30 (0–30)
≥12 / total score
Severity mean
Stable (n = 74)
Progressive (n = 109)
Statistics
Stable (n = 74)
Progressive (n = 109)
Statistics
2.7
4.6
p = 0.525
14.7
p = 0.048
2.7
6.4
p = 0.254
6.8
17.4
p = 0.036
16.2
12.8
p = 0.521
51.4
54.1
p = 0.712
41.9
26.6
p = 0.031
43.2
42.2
p = 0.889
43.2
41.3
p = 0.792
85.1
86.2
p = 0.834
29.2
35.2
p = 0.399
0.0
0.0
NA
21.9
18.5
p = 0.574
46.6
53.7
p = 0.347
54.8
63.0
p = 0.272
12.2
16.5
p = 0.415
22.9
21.9
p = 0.882
2.1 ± 1.5
(0–7)
0.3 ± 1.0
(0–6)
0.2 ± 0.7
(0–6)
0.5 ± 1.5
(0–11)
0.3 ± 0.8
(0–4)
1.5 ± 1.8
(0–7)
0.4 ± 0.7
(0–3)
0.8 ± 1.1
(0–5)
0.8 ± 1.3
(0–8)
4.2 ± 3.9
(0–22)
0.4 ± 0.6
(0–3)
10.0 ± 0.2
(10–12)
12.0 ± 2.6
(10–28)
11.7 ± 4.8
(8–34)
33.7 ± 6.5
(29–72)
4.3 ± 3.3
(0–18)
8.3 ± 4.6
(0–20)
p = 0.145
5.4
1.7 ± 1.5
(0–6)
0.1 ± 0.5
(0–4)
0.1 ± 0.5
(0–4)
0.2 ± 0.9
(0–6)
0.2 ± 0.5
(0–3)
1.2 ± 1.4
(0–5)
0.5 ± 0.7
(0–3)
0.8 ± 1.2
(0–5)
0.7 ± 0.9
(0–3)
3.5 ± 3.1
(0–16)
0.4 ± 0.8
(0–3)
10.0 ± 0.2
(10–11)
12.2 ± 2.8
(11–24)
10.7 ± 3.8
(8–29)
32.9 ± 5.1
(29–58)
4.2 ± 3.0
(0–12)
8.0 ± 4.7
(1–19)
p = 0.045
p = 0.265
p = 0.036
p = 0.653
p = 0.446
p = 0.052
p = 0.966
p = 0.939
p = 0.313
p = 0.598
p = 0.988
p = 0.696
p = 0.127
p = 0.303
p = 0.959
p = 0.514
Data are given as percentages and mean scores ± SD with ranges represented between brackets. For comparison of prevalence percentages,
Chi-square statistics were used. For comparison of severity scores, Mann-Whitney U test was used. The level of significance was set at p < 0.05.
were applied to compare (semi) continuous variables,
Chi-square statistics for categorical data.
Cox proportional hazard models were fitted to test
if a given variable could predict the time to change in
diagnosis from a baseline of MCI to an endpoint of
AD. To estimate the Hazard Ratios (HR) for incident
AD, 95% confidence intervals (CI) were used. All Cox
proportional hazard models included age at baseline as
a covariate. The significance of the variable of interest
was tested using a likelihood ratio test, comparing the
model with both age at baseline and the variable of
interest, to a model containing only age at baseline.
Given the study objectives, focus was put on the
stable MCI patients (no progress to dementia during
our follow-up) in comparison with the AD progressive
MCI patients. Nonetheless, in the end we also applied
the Cox proportional hazard statistics to the data of all
235 MCI patients with a group of stable MCI patients
compared to progressive MCI patients, considering all
types of dementia as the other group, including the
category ‘unspecified’ type of dementia.
Probability levels of <0.05 were considered significant. Statistical analyses were carried out using SPSS
Statistics 17.0.
RESULTS
The follow-up outcomes from the 235 baseline MCI
patients that met the study criteria were: (1) 74 ‘stable’ MCI patients and (2) 161 ‘progressive’ MCI
patients progressed to dementia. From these 161: (a)
109 progressed to AD, (b) 13 progressed to a non-AD
dementia; and (c) 39 progressed to an unspecified type
of dementia. So 69% (n = 161) of the 235 MCI patients
progressed to any kind of dementia and at least 46%
�1244
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
(n = 109) of the 235 MCI patients progressed to AD.
The baseline characteristics of the study population are
summarized in Table 1. The average time in progressive patients to develop AD was 2 years (2.0 ± 1.6 SD).
The mean time of clinical follow-up of stable patients
was 4 years (3.8 ± 2.3 SD) with a minimum of one year
and a maximum of 9 years. On average, the progressive
patients were older at study inclusion and age at onset
and had a lower MMSE at baseline.
Table 2 compares the prevalence and severity of
BPSD between the stable and the progressive MCI
patients. Delusions and psychosis are more prevalent and severe at baseline in progressive patients as
compared to the stable MCI patients. Diurnal rhythm
disturbances are more prevalent in stable MCI patients
than in progressive, but mainly due to ‘repetitive wakening during the night’. When it comes to more severe
forms of diurnal rhythm disturbances, there is no difference in prevalence between stable and progressive
MCI patients.
To study any difference in baseline BPSD between
MCI subtypes or between men and women, we compared MFS, Behave-AD, CMAI, GDS-30, and CSDD
total scores and Behave-AD global score. There was
no difference in BPSD between the 4 MCI subtypes.
Between men and women only the mean GDS-30 total
score differed as women displayed more depressive
symptoms than men (♂: 7.4 (±4.1) versus ♀: 8.9 (±4.9),
p = 0.035).
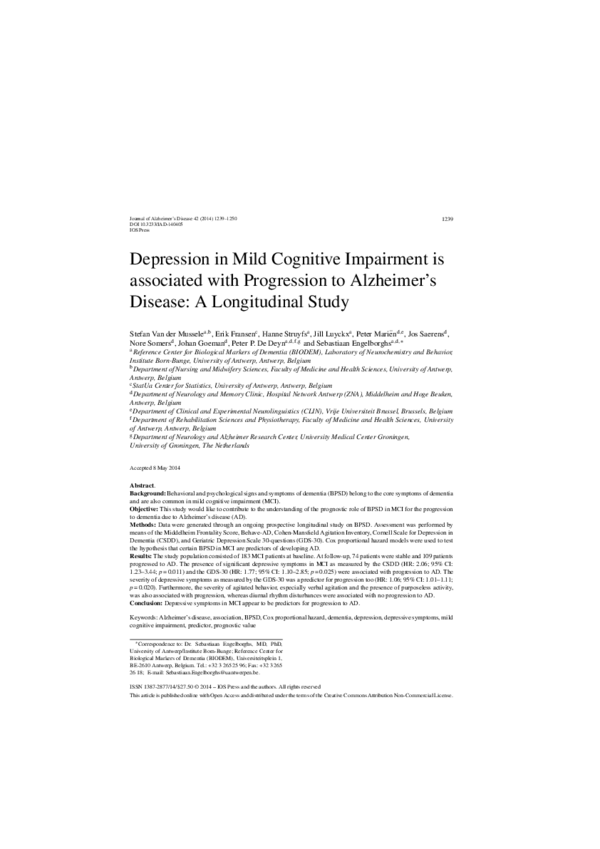
Cox proportional hazards regression model (Table 3)
adjusted for age (Fig. 1) demonstrated that the presence of depressive symptoms was associated with
progression from MCI to AD. Significant depressive symptoms as measured by the CSDD doubled
the hazard of progression to AD (Fig. 1). Significant
depressive symptoms as measured by the GDS-30 are
associated with a 77% increased hazard of progression
to AD. The presence of diurnal rhythm disturbances,
associated with a 35% decreased hazard, appeared to
be ‘protective’ for the progression to AD. Each 1-unit
increase on the cluster verbally agitated behavior of
the CMAI, was associated with a 6% increased hazard
of progression; and each 1-unit increase on the total
score of the CMAI, was associated with a 4% increased
hazard. Also each 1-unit increase on the GDS-30 was
associated with a 6% increased hazard of progression.
Additionally, we found that only the presence (HR:
2.00; 95% CI: 1.12–3.59; p = 0.032) and severity (HR:
1.58; 95% CI: 1.06 – 2.36; p = 0.045) of ‘purposeless activity’ is a predictor for progression to AD.
The Behave-AD items ‘Godot syndrome’, ‘fear of
being left alone’, ‘other anxieties’, ‘other phobias’,
Fig. 1. Survival curve: Progression to AD related to depressive
symptoms in MCI. The prediction of incident AD was estimated
with Cox proportional hazards regression models, adjusted for age.
Line 0: MCI patients without significant depressive symptoms based
on CSDD ≤7 (n = 156). Line 1: MCI patients with significant depressive symptoms based on CSDD >7 (n = 27). p = 0.011.
‘wandering away’ and ‘inappropriate activity’ were no
significant predictors for progression to AD.
Considering all MCI patients (n = 235) in a secondary analysis, we could only demonstrate that
agitated behavior in MCI was associated with progression to dementia, especially verbal agitation. The
presence of agitated behavior as measured by the
total score of the CMAI was associated with a 46%
increased hazard of progression to dementia (HR: 1.46;
95% CI: 1.06 – 2.00; p = 0.020). Also each 1-unit
increase on the total score of the CMAI was associated with a 6% increased hazard of progression (HR:
1.06; 95% CI: 1.02 – 1.10; p = 0.003). The presence of
verbally agitated behavior as measured by the CMAI
was associated with a 67% increased hazard of progression to dementia (HR: 1.67; 95% CI: 1.20 – 2.31;
p = 0.002). Also each 1-unit increase on the cluster verbally agitated behavior of the CMAI was associated
with a 4% increased hazard of progression (HR: 1.04;
95% CI: 1.01 – 1.07; p = 0.012). In this analysis, we
could not confirm that depressive symptoms were a
predictor in MCI for progression to dementia (CSDD
>7: p = 0.179; CSDD total score: p = 0.540; GDS-30
≥12: p = 0.158; GDS-30 total score: p = 0.136). Moreover, other BPSD, like the presence of diurnal rhythm
disturbances and the presence and severity of purposeless activity were no more significant predictors in
MCI for the progression to dementia in this analysis.
Sixty-six patients underwent lumbar puncture for CSF
�1245
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
Table 3
MCI BPSD hazard ratios for progression to AD
Behavior/disturbances
MFS ≥5 score / total (0–10)
Frontal lobe symptoms
Behave-AD (0–21)
Delusions
Behave-AD (0–15)
Hallucinations
Behave-AD (0–36)
Psychosis
Behave-AD (0–9)
Activity
Behave-AD (0–9)
Aggressiveness
Behave-AD (0–3)
Diurnal rhythm
Behave-AD (0–6)
Affective
Behave-AD (0–12)
Anxiety/Phobias
Behave-AD (0–75)
Total score
Behave-AD (0–3)
Global score
CMAI (10–70)
Aggressive
CMAI (11–77)
Physically non-aggressive
CMAI (8–56)
Verbally agitated
CMAI (29–203)
Total score
CSDD (0–38)
>7 / total score
GDS-30 (0–30)
≥12 / total score
Present (dichotomous)
(semi) Continuous
HR
95% CI
Statistics
HR
95% CI
Statistics
1.32
0.53–3.27
p = 0.571
1.03
0.90–1.18
p = 0.689
1.60
0.93–2.73
p = 0.105
1.12
0.92–1.35
p = 0.289
0.84
0.39–1.82
p = 0.646
0.93
0.70–1.25
p = 0.630
1.36
0.82–2.24
p = 0.252
1.03
0.91–1.17
p = 0.669
1.28
0.73–2.26
p = 0.407
1.26
0.97–1.65
p = 0.107
1.21
0.83–1.77
p = 0.327
1.05
0.94–1.16
p = 0.395
0.65
0.42–1.00
p = 0.045
0.84
0.60–1.16
p = 0.269
1.21
0.82–1.77
p = 0.347
1.10
0.93–1.31
p = 0.286
1.08
0.73–1.59
p = 0.706
1.07
0.91–1.25
p = 0.412
1.13
0.65–1.95
p = 0.662
1.03
0.98–1.08
p = 0.230
1.45
0.97–2.17
p = 0.072
1.07
0.83–1.38
p = 0.591
NA
NA
NA
0.93
0.39–2.22
p = 0.864
0.94
0.58–1.54
p = 0.812
1.01
0.93–1.10
p = 0.811
1.39
0.95–2.03
p = 0.092
1.06
1.02–1.10
p = 0.012
1.48
1.00–2.19
p = 0.050
1.04
1.01–1.07
p = 0.034
2.06
1.23–3.44
p = 0.011
1.06
0.99–1.13
p = 0.082
1.77
1.10–2.85
p = 0.025
1.06
1.01–1.11
p = 0.020
The prediction of incident AD was estimated with Cox proportional hazards regression models, adjusted for age. Hazard ratios (HR) with 95%
confidence intervals (CI) are reported for the associations of each BPSDvariable with incident AD. The level of significance was set at p < 0.05.
biomarker analyses. From these 66 patients, 52 had
their lumbar puncture within a 3 month time-linked
interval with the study inclusion date. Pathological
biomarker profiles pointing to AD were found in 22
patients (42%). The progressive group had a higher
percentage of patients with an AD pathological CSF
biomarker profile. These biomarker profiles appeared
to be a strong predictor for the progression to AD (HR:
5.57; 95% CI: 2.46 – 12.61; p < 0.001).
DISCUSSION
We conclude that the presence of significant depressive symptoms in MCI as measured by the CSDD
(HR: 2.06; 95% CI: 1.23–3.44; p = 0.011) and the
GDS-30 (HR: 1.77; 95% CI: 1.10–2.85; p = 0.025)
are associated with an increased hazard of progression to AD. Also the severity of depressive symptoms
as measured by the GDS-30 (HR: 1.06; 95% CI:
1.01–1.11; p = 0.020) is a predictor for progression to
AD. Furthermore, the severity of agitated behavior,
especially verbal agitation and the presence of purposeless activity are identified as predictors for progression
AD.
From the secondary analysis, we learn that agitation
in MCI is also a predictor for progression to dementia
in general and that depressive symptoms in MCI are
specific predictors for progression to AD, as they were
not significant for progression to unspecified dementia.
The dementia (69%) and AD (≥46%) progression
rates in our study are quite high as compared to other
studies [5]. This might be due to strict application of
the MCI definition, with objective cognitive impairment quantified as a performance of more than 1.5 SD
below the appropriate mean on the neuropsychological
subtests [5]; the research setting, being a specialized
�1246
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
hospital-based setting, a memory clinic [5]; and strict
in- and exclusion criteria focusing on a neurodegenerative MCI etiology [1, 2].
Depression is known to be associated with the
incidence of MCI and dementia [36]. In some studies, also in MCI, depressive symptoms are associated
with progression to AD or dementia [37, 38]. Our
findings are in line with previous research, acknowledging that depression or depressive symptoms are
of prognostic value for progression from MCI to AD
[38–43], although this could not be demonstrated in
some other studies [44–50]. One study even found a
negative correlation between progression and the presence of affective symptoms [51]. Nevertheless, this
conflicting evidence might be due to differences in
study methodology, such as MCI definition, assessment instruments, sample size, statistics, follow-up
term, research setting, etc. Furthermore, neither Gallagher et al. [45] nor our study could demonstrate a link
between affective symptoms in MCI and progression
to AD by means of the Behave-AD. The Behave-AD
cluster affective disturbance was probably not specific
enough towards depressive symptoms as compared
to the CSDD and GDS-30 depression scales. Also
in accordance with our results, Gallagher et al. [45]
showed by means of the Behave-AD that purposeless
activity was a significant clinical predictor for AD in
MCI.
That diurnal rhythm disturbances are associated
with no progression to AD is surprising, as circadian
rhythm disturbances are frequent in AD [52–54] and
in some studies even a predictor for the progression to
dementia [55]. An explanation for our finding can be
a lack of sensitivity of the Behave-AD cluster diurnal
rhythm disturbances (that only consists of one item)
in progressive MCI patients, as it is also known to
be difficult to obtain accurate self-reports on sleep in
demented patients [56].
Hazard ratios often indicate the risk for an event,
but one could question to which extent depression is
a true ‘risk factor’ versus an early symptom occurring in the prodromal AD stage. Panza et al. [57]
concluded in 2010 that at least in certain subsets of
older adults, late-life depression, MCI and dementia
could represent a possible clinical continuum [57].
They hypothesized that the neuropathological and neurochemical changes that characterize AD can play a
role in the etiopathogenesis of depressive symptoms
[57]. So, assuming that MCI may be the earliest identifiable clinical stage of dementia, depressive symptoms
may be an early manifestation rather than a risk factor for dementia and AD [57]. Recent studies provided
also neuroanatomical [58, 59] and neurochemical [60]
evidence to support this hypothesis.
Furthermore, we also found that severity of agitation in MCI, especially verbally agitated behavior,
was predictive for progression to AD. Neuroanatomical studies about agitation in MCI and AD point
toward involvement of frontal and temporal brain areas
[61]. Recently Trzepacz et al. [61] and Tsai et al.
[60] added evidence to this theory and confirmed the
relation between agitation and AD pathology in these
specific brain areas through neurodegeneration and
neurochemical changes. Also worse cognitive performance on the MMSE correlated with AD-related brain
changes in these two studies.
Moreover, the following hypothesis might also
explain the interrelation between depression and agitation as predictors for progression to AD. As described
above, AD can play a role in the etiopathogenesis of depressive symptom. In addition, decreased
serotonergic activity has been related to depression
[62] and dopaminergic neurons are modulated by
serotonergic innervation [63]. Indeed, the serotonergic system appears to have an inhibitory effect
on the dopaminergic function [63, 64]. Furthermore,
ascending dopaminergic pathways are part of the
frontal-subcortical circuitry [65] and the dopaminergic
system is one of the important modulators of frontal
lobe function [66]. Consequently, frontal-subcortical
circuit dysfunction leads to impaired executive functions, apathy and impulsivity [65] and might thus as
well explain the prevalence and severity of agitation in
MCI and AD patients.
Given our results, the interrelation of depression and agitation and recent neurochemical and
neuroanatomical evidence, we may conclude that significant depressive symptoms and increased agitation
are indeed early symptoms of AD rather than risk factors, which however has to be confirmed by future
research.
This study has several strengths. First, this study
is an up-to-9-year and still ongoing prospective
longitudinal study. The continuous, even after AD progression, clinical and neuropsychological follow-up
of included subjects contributed to increased diagnostic certainty of the population included. Second, the
study included a well-characterized MCI population,
diagnosed by strict application of stringent clinical
diagnostic criteria and well monitored over time in
our longitudinal protocol. Third, all patients were diagnosed by clinicians in the same center which preserves
homogeneity in the MCI diagnostics and AD progression diagnoses. Fourth, we found homogeneous
�S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
BPSD characteristics and AD progression rates in the
four MCI subtypes of this study population. Consequently, no bias was introduced due to MCI BPSD or
subtype heterogeneity. However, the absence of differences in BPSD comparing MCI subtypes might
be due to limited statistical validity, because of relatively small subgroups of non-amnestic MCI patients
included. Last but not least, though it was not the purpose of this study, we showed that a pathological AD
biomarker profile was a strong predictor for progression to AD. Even though, these data were only available
for a limited subgroup, the results were robust and in
line with previous research [67, 68].
In 2013, mild and major neurocognitive disorders
(NCD) were introduced as new categories in the 5th
edition of the Diagnostic and Statistical Manual of
Mental Disorders (DSM-5) with their own diagnostic
criteria [69]. Their adoption in the DSM-5 is in fact an
important recognition of MCI as a clinical diagnostic
entity. The reason of acknowledgment in the DSM-5
is the same as the motivation of the National Institute
of Aging-Alzheimer Association (NIA-AA) working
groups [3] and the International Working Group (IWG)
[70]: to facilitate the diagnosis of the very early stages
of AD, hoping for more successful therapeutic developments, through better research criteria. Mild and
major NCD can also be ‘due to AD’, like ‘MCI due
to AD’ (NIA-AA) or ‘prodromal AD’ (IWG). NCD
covers the concept of MCI with a distinction between:
mild, when the cognitive decline is modest without
interference with complex instrumental activities of
daily living; and major, when the cognitive decline is
significant with a minimal interference with instrumental activities of daily living. In contrast with the new
concepts of the NIA-AA and the IWG, biomarkers are
not included in the NCD (due to AD) criteria.
Some study limitations are known to the authors.
First, Table 3 shows the main results and several
p-values that are nominally significant (p < 0.05),
including the significant hazard ratios related to the
presence of significant depressive symptoms (CSDD:
p = 0.011; GDS-30: p = 0.025) and the presence of
diurnal rhythm disturbances (p = 0.045); and the significant hazard ratios related to the severity of agitation
(p = 0.034), verbally agitated behavior (p = 0.012)
and the severity of depressive symptoms (GDS-30:
p = 0.020). However, since we have tested multiple hypotheses, the risk of a false positive finding
is inflated. Therefore, these significant associations
should be regarded as interesting leads for further
research rather than firm evidence of a strong association. Second, from 39 of the 235 MCI patients that met
1247
our study criteria, we were not able to retrieve to which
type of dementia they progressed. Third, our study
population was recruited in a memory clinic, which
might have introduced a selection bias as BPSD might
have contributed to referral. Fourth, another bias is that
some study subjects might have developed depressive
symptoms as a psychological reaction to the cognitive
decline [57]. Fifth, although some studies found apathy
as a predictor factor for the progression to AD by application of Cox survival analysis [47, 48], we did not
study the prognostic value of this specific symptom as
no specific apathy assessment instrument was included
in our study. Apathy has only been assessed partially
through items 7 ‘( . . . ) or emotional bluntness’ and 8
‘aspontaneity’ of the MFS. Lastly, our study population was not free of psychotropic drug intake, as more
than half of the study population was treated with at
least one psychotropic drug at baseline. Consequently,
these psychopharmacological agents may have influenced our results by masking potential associations
through diminished BPSD.
Some studies use MMSE scores as part of their key
eligibility criteria for MCI like the Alzheimer’s Disease Neuroimaging Initiative which mentions MMSE
scores 24–30 (inclusive) for MCI subjects as an inclusion criterion. This might raise questions about our
MCI study population with a broad MMSE range
(18–30). However, we would like to stress that the
MMSE was only used for screening purposes. Besides,
all patients underwent an extensive time-linked (±3
months) neuropsychological examination with adjustment for gender, age and education, comprising
amongst others the Wechsler Memory Scale, Hierarchic Dementia Scale and/or Repeatable Battery for the
Assessment of Neuropsychological Status. This neuropsychological examination was used to test for the
clinical diagnostic criteria for MCI and/or progression
to AD.
Depressive symptoms in MCI appear to be associated with progression to AD. Further research is
important to unravel whether depression is a true ‘risk
factor’ in MCI for the progression to AD or whether it
is an early symptom of AD.
ACKNOWLEDGMENTS
This research was supported by the University
Research Fund of the University of Antwerp; the
Foundation for Alzheimer Research (SAO-FRA);
the Institute Born-Bunge; an unrestricted research
grand form Lundbeck NV (Belgium); the agreement
�1248
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
between the Institute Born-Bunge and the University
of Antwerp; the central Biobank facility of the Institute Born-Bunge/University Antwerp; Neurosearch
Antwerp; the Thomas Riellaerts Research Fund; the
Research Foundation - Flanders (FWO-Vlaanderen);
the Agency for Innovation by Science and Technology
(IWT); the Interuniversity Attraction Poles (IAP) program P7/16 of the Belgian Science Policy Office; the
Methusalem excellence grant of the Flemish Government, Belgium; and the Medical Research Foundation
Antwerp. This work is part of the BIOMARKAPD
project within the EU Joint Programme for Neurodegenerative Disease Research (JPND). This work
has received support from the EU/EFPIA Innovative
Medicines Initiative Joint Undertaking (EMIF grant
n◦ 115372). The authors acknowledge Prof. Dr. M.
Elseviers (University of Antwerp), the administrative
assistance of W. Wittebolle, S. Hicketick, A. Eyckens and the clinical staff involved (Hospital Network
Antwerp).
Authors’ disclosures available online (http://www.jalz.com/disclosures/view.php?id=2326).
[8]
[9]
[10]
[11]
[12]
[13]
[14]
[15]
REFERENCES
[16]
[1]
[2]
[3]
[4]
[5]
[6]
[7]
Petersen RC (2004) Mild cognitive impairment as a diagnostic
entity. J Intern Med 256, 183-194.
Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L,
Wahlund LO, Nordberg A, Backman L, Albert M, Almkvist
O, Arai H, Basun H, Blennow K, de Leon M, DeCarli C, Erkinjuntti T, Giacobini E, Graff C, Hardy J, Jack C, Jorm A,
Ritchie K, van Duijn C, Visser P, Petersen RC (2004) Mild
cognitive impairment–beyond controversies, towards a consensus: Report of the International Working Group on Mild
Cognitive Impairment. J Intern Med 256, 240-246.
Albert MS, Dekosky ST, Dickson D, Dubois B, Feldman HH,
Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC,
Snyder PJ, Carrillo MC, Thies B, Phelps CH (2011) The
diagnosis of mild cognitive impairment due to Alzheimer’s
disease: Recommendations from the National Institute on
Aging-Alzheimer’s Association workgroups on diagnostic
guidelines for Alzheimer’s disease. Alzheimers Dement 7,
270-279.
Dierckx E, Engelborghs S, De Raedt R, De Deyn PP, PonjaertKristoffersen I (2007) Mild cognitive impairment: What’s in
a name? Gerontology 53, 28-35.
Mitchell AJ, Shiri-Feshki M (2009) Rate of progression of
mild cognitive impairment to dementia–meta-analysis of 41
robust inception cohort studies. Acta Psychiatr Scand 119,
252-265.
Finkel SI, Costa e Silva, Cohen G, Miller S, Sartorius N
(1996) Behavioral and psychological signs and symptoms of
dementia: A consensus statement on current knowledge and
implications for research and treatment. Int Psychogeriatr 8,
497-500.
Van der Mussele S, Le Bastard N, Vermeiren Y, Saerens J,
Somers N, Marien P, Goeman J, De Deyn PP, Engelborghs S
(2013) Behavioral symptoms in mild cognitive impairment as
[17]
[18]
[19]
[20]
[21]
[22]
[23]
compared with Alzheimer’s disease and healthy older adults.
Int J Geriatr Psychiatry 28, 265-275.
Van der Mussele S, Marien P, Saerens J, Somers N, Goeman
J, De Deyn PP, Engelborghs S (2014) Behavioral syndromes
in mild cognitive impairment and Alzheimer’s disease. J
Alzheimers Dis 38, 319-329.
Monastero R, Mangialasche F, Camarda C, Ercolani S,
Camarda R (2009) A systematic review of neuropsychiatric
symptoms in mild cognitive impairment. J Alzheimers Dis 18,
11-30.
Apostolova LG, Cummings JL (2008) Neuropsychiatric manifestations in mild cognitive impairment: A systematic review
of the literature. Dement Geriatr Cogn Disord 25, 115-126.
Folstein MF, Folstein SE, McHugh PR (1975) Mini-mental
state. A practical method for grading the cognitive state of
patients for the clinician. J Psychiatr Res 12, 189-198.
The Psychological Corporation (1998) WAIS-III-WMS-III
Technical Manual, Harcourt Brace & Co, London.
Randolph C, Tierney MC, Mohr E, Chase TN (1998) The
Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary clinical validity. J Clin Exp
Neuropsychol 20, 310-319.
Cole MG, Dastoor DP (1987) A new hierarchic approach to
the measurement of dementia. Accurate results within 15 to
30 minutes. Psychosomatics 28, 298-301, 304.
McKhann G, Drachman D, Folstein M, Katzman R, Price
D, Stadlan EM (1984) Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under
the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 34,
939-944.
American Psychiatric Association (2000) DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, Fourth
Edition (Revised Text). American Psychiatric Association,
Washington, DC.
Le Bastard N, Coart E, Vanderstichele H, Vanmechelen E,
Martin JJ, Engelborghs S (2013) Comparison of two analytical platforms for the clinical qualification of Alzheimer’s
disease biomarkers in pathologically-confirmed dementia. J
Alzheimers Dis 33, 117-131.
Reisberg B, Ferris SH, de Leon MJ, Crook T (1982) The
Global Deterioration Scale (GDS) for assessment of primary
degenerative dementia. Am J Psychiatry 139, 1136-1139.
Aries MJ, Le Bastard N, Debruyne H, Van Buggenhout
M, Nagels G, De Deyn PP, Engelborghs S (2010) Relation
between frontal lobe symptoms and dementia severity within
and across diagnostic dementia categories. Int J Geriatr Psychiatry 25, 1186-1195.
De Deyn PP, Engelborghs S, Saerens J, Goeman J, Marien
P, Maertens K, Nagels G, Martin JJ, Pickut BA (2005) The
Middelheim Frontality Score: A behavioural assessment scale
that discriminates frontotemporal dementia from Alzheimer’s
disease. Int J Geriatr Psychiatry 20, 70-79.
Reisberg B, Borenstein J, Salob SP, Ferris SH, Franssen E,
Georgotas A (1987) Behavioral symptoms in Alzheimer’s disease: Phenomenology and treatment. J Clin Psychiatry 48,
9-15.
Cohen-Mansfield J (1996) Conceptualization of agitation:
Results based on the Cohen-Mansfield Agitation Inventory
and the Agitation Behavior Mapping Instrument. Int Psychogeriatr 8, 309-315.
Choy CN, Lam LC, Chan WC, Li SW, Chiu HF (2001) Agitation in Chinese elderly: Validation of the Chinese version of
the Cohen-Mansfield Agitation Inventory. Int Psychogeriatr
13, 325-335.
�S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
[24]
[25]
[26]
[27]
[28]
[29]
[30]
[31]
[32]
[33]
[34]
[35]
[36]
[37]
[38]
[39]
[40]
[41]
Cohen-Mansfield J, Marx MS, Rosenthal AS (1989) A
description of agitation in a nursing home. J Gerontol 44,
M77-M84.
Gruber-Baldini AL, Boustani M, Sloane PD, Zimmerman
S (2004) Behavioral symptoms in residential care/assisted
living facilities: Prevalence, risk factors, and medication management. J Am Geriatr Soc 52, 1610-1617.
Suh GH (2004) Agitated behaviours among the institutionalized elderly with dementia: Validation of the Korean version
of the Cohen-Mansfield Agitation Inventory. Int J Geriatr
Psychiatry 19, 378-385.
Testad I, Aasland AM, Aarsland D (2007) Prevalence and correlates of disruptive behavior in patients in Norwegian nursing
homes. Int J Geriatr Psychiatry 22, 916-921.
Zuidema SU, Derksen E, Verhey FR, Koopmans RT (2007)
Prevalence of neuropsychiatric symptoms in a large sample
of Dutch nursing home patients with dementia. Int J Geriatr
Psychiatry 22, 632-638.
Zuidema SU, de Jonghe JF, Verhey FR, Koopmans RT (2010)
Environmental correlates of neuropsychiatric symptoms in
nursing home patients with dementia. Int J Geriatr Psychiatry
25, 14-22.
Alexopoulos GS, Abrams RC, Young RC, Shamoian CA
(1988) Cornell Scale for Depression in Dementia. Biol Psychiatry 23, 271-284.
Burns A, Lawlor B, Craig S (2004) Assessment Scales in Old
Age Psychiatry, Martin Dunitz, London.
Alexopoulos GS, Abrams RC, Young RC, Shamoian CA
(1988) Use of the Cornell scale in nondemented patients. J
Am Geriatr Soc 36, 230-236.
Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M,
Leirer VO (1982) Development and validation of a geriatric
depression screening scale: A preliminary report. J Psychiatr
Res 17, 37-49.
Debruyne H, Van Buggenhout M, Le Bastard N, Aries M,
Audenaert K, De Deyn PP, Engelborghs S (2009) Is the geriatric depression scale a reliable screening tool for depressive
symptoms in elderly patients with cognitive impairment? Int
J Geriatr Psychiatry 24, 556-562.
Engelborghs S, De VK, Van de Casteele T, Vanderstichele
H, Van EB, Cras P, Martin JJ, Vanmechelen E, De Deyn PP
(2008) Diagnostic performance of a CSF-biomarker panel
in autopsy-confirmed dementia. Neurobiol Aging 29, 11431159.
Gao Y, Huang C, Zhao K, Ma L, Qiu X, Zhang L, Xiu Y,
Chen L, Lu W, Huang C, Tang Y, Xiao Q (2013) Depression
as a risk factor for dementia and mild cognitive impairment: A
meta-analysis of longitudinal studies. Int J Geriatr Psychiatry
28, 441-449.
Simard M, Hudon C, van RR (2009) Psychological distress
and risk for dementia. Curr Psychiatry Rep 11, 41-47.
Enache D, Winblad B, Aarsland D (2011) Depression in
dementia: Epidemiology, mechanisms, and treatment. Curr
Opin Psychiatry 24, 461-472.
Teng E, Lu PH, Cummings JL (2007) Neuropsychiatric symptoms are associated with progression from mild cognitive
impairment to Alzheimer’s disease. Dement Geriatr Cogn
Disord 24, 253-259.
Steenland K, Karnes C, Seals R, Carnevale C, Hermida
A, Levey A (2012) Late-life depression as a risk factor
for mild cognitive impairment or Alzheimer’s disease in
30 US Alzheimer’s disease centers. J Alzheimers Dis 31,
265-275.
Rosenberg PB, Mielke MM, Appleby BS, Oh ES, Geda
YE, Lyketsos CG (2013) The association of neuropsychi-
[42]
[43]
[44]
[45]
[46]
[47]
[48]
[49]
[50]
[51]
[52]
[53]
[54]
[55]
[56]
[57]
1249
atric symptoms in MCI with incident dementia and Alzheimer
disease. Am J Geriatr Psychiatry 21, 685-695.
Modrego PJ, Ferrandez J (2004) Depression in patients with
mild cognitive impairment increases the risk of developing
dementia of Alzheimer type: A prospective cohort study. Arch
Neurol 61, 1290-1293.
Lee GJ, Lu PH, Hua X, Lee S, Wu S, Nguyen K, Teng E,
Leow AD, Jack CR, Jr., Toga AW, Weiner MW, Bartzokis G,
Thompson PM (2012) Depressive symptoms in mild cognitive
impairment predict greater atrophy in Alzheimer’s diseaserelated regions. Biol Psychiatry 71, 814-821.
Devier DJ, Pelton GH, Tabert MH, Liu X, Cuasay K, Eisenstadt R, Marder K, Stern Y, Devanand DP (2009) The impact
of anxiety on conversion from mild cognitive impairment to
Alzheimer’s disease. Int J Geriatr Psychiatry 24, 1335-1342.
Gallagher D, Coen R, Kilroy D, Belinski K, Bruce I, Coakley
D, Walsh B, Cunningham C, Lawlor BA (2011) Anxiety and
behavioural disturbance as markers of prodromal Alzheimer’s
disease in patients with mild cognitive impairment. Int J Geriatr Psychiatry 26, 166-172.
Palmer K, Berger AK, Monastero R, Winblad B, Backman
L, Fratiglioni L (2007) Predictors of progression from mild
cognitive impairment to Alzheimer disease. Neurology 68,
1596-1602.
Palmer K, Di IF, Varsi AE, Gianni W, Sancesario G, Caltagirone C, Spalletta G (2010) Neuropsychiatric predictors
of progression from amnestic-mild cognitive impairment to
Alzheimer’s disease: The role of depression and apathy. J
Alzheimers Dis 20, 175-183.
Richard E, Schmand B, Eikelenboom P, Yang SC, Ligthart
SA, Moll van Charante EP, van Gool WA (2012) Symptoms
of apathy are associated with progression from mild cognitive
impairment to Alzheimer’s disease in non-depressed subjects.
Dement Geriatr Cogn Disord 33, 204-209.
Robert PH, Berr C, Volteau M, Bertogliati C, Benoit M,
Sarazin M, Legrain S, Dubois B (2006) Apathy in patients
with mild cognitive impairment and the risk of developing
dementia of Alzheimer’s disease: A one-year follow-up study.
Clin Neurol Neurosurg 108, 733-736.
Robert PH, Berr C, Volteau M, Bertogliati-Fileau C, Benoit M,
Guerin O, Sarazin M, Legrain S, Dubois B (2008) Importance
of lack of interest in patients with mild cognitive impairment.
Am J Geriatr Psychiatry 16, 770-776.
Ramakers IH, Visser PJ, Aalten P, Kester A, Jolles J, Verhey
FR (2010) Affective symptoms as predictors of Alzheimer’s
disease in subjects with mild cognitive impairment: A 10-year
follow-up study. Psychol Med 40, 1193-1201.
Ju YE, McLeland JS, Toedebusch CD, Xiong C, Fagan AM,
Duntley SP, Morris JC, Holtzman DM (2013) Sleep quality
and preclinical Alzheimer disease. JAMA Neurol 70, 587-593.
Rothman SM, Mattson MP (2012) Sleep disturbances in
Alzheimer’s and Parkinson’s diseases. Neuromolecular Med
14, 194-204.
Weldemichael DA, Grossberg GT (2010) Circadian rhythm
disturbances in patients with Alzheimer’s disease: A review.
Int J Alzheimers Dis 2010, pii: 716453.
Somme J, Fernandez-Martinez M, Molano A, Zarranz JJ
(2013) Neuropsychiatric symptoms in amnestic mild cognitive impairment: Increased risk and faster progression to
dementia. Curr Alzheimer Res 10, 86-94.
Bombois S, Derambure P, Pasquier F, Monaca C (2010) Sleep
disorders in aging and dementia. J Nutr Health Aging 14,
212-217.
Panza F, Frisardi V, Capurso C, D’Introno A, Colacicco AM,
Imbimbo BP, Santamato A, Vendemiale G, Seripa D, Pilotto
�1250
[58]
[59]
[60]
[61]
[62]
[63]
[64]
S. Van der Mussele et al. / Depression in MCI Associated with Progression to AD
A, Capurso A, Solfrizzi V (2010) Late-life depression, mild
cognitive impairment, and dementia: Possible continuum? Am
J Geriatr Psychiatry 18, 98-116.
Son JH, Han DH, Min KJ, Kee BS (2013) Correlation between
gray matter volume in the temporal lobe and depressive symptoms in patients with Alzheimer’s disease. Neurosci Lett 548,
15-20.
Lee GJ, Lu PH, Hua X, Lee S, Wu S, Nguyen K, Teng E,
Leow AD, Jack CR Jr, Toga AW, Weiner MW, Bartzokis G,
Thompson PM (2012) Depressive symptoms in mild cognitive
impairment predict greater atrophy in Alzheimer’s diseaserelated regions. Biol Psychiatry 71, 814-821.
Tsai CF, Hung CW, Lirng JF, Wang SJ, Fuh JL (2013) Differences in brain metabolism associated with agitation and
depression in Alzheimer’s disease. East Asian Arch Psychiatry 23, 86-90.
Trzepacz PT, Yu P, Bhamidipati PK, Willis B, Forrester T,
Tabas L, Schwarz AJ, Saykin AJ (2013) Frontolimbic atrophy
is associated with agitation and aggression in mild cognitive
impairment and Alzheimer’s disease. Alzheimers Dement 9,
S95-S104.
Coppen A (1967) The biochemistry of affective disorders. Br
J Psychiatry 113, 1237-1264.
Di Giovanni G, Esposito E, Di Matteo V (2010) Role of serotonin in central dopamine dysfunction. CNS Neurosci Ther
16, 179-194.
Engelborghs S, Vloeberghs E, Le BN, Van BM, Marien
P, Somers N, Nagels G, Pickut BA, De Deyn PP (2008)
[65]
[66]
[67]
[68]
[69]
[70]
The dopaminergic neurotransmitter system is associated with
aggression and agitation in frontotemporal dementia. Neurochem Int 52, 1052-1060.
Bonelli RM, Cummings JL (2007) Frontal-subcortical circuitry and behavior. Dialogues Clin Neurosci 9, 141-151.
Goldman-Rakic PS, Lidow MS, Gallager DW (1990) Overlap of dopaminergic, adrenergic, and serotoninergic receptors
and complementarity of their subtypes in primate prefrontal
cortex. J Neurosci 10, 2125-2138.
Hansson O, Zetterberg H, Buchhave P, Londos E, Blennow K,
Minthon L (2006) Association between CSF biomarkers and
incipient Alzheimer’s disease in patients with mild cognitive
impairment: A follow-up study. Lancet Neurol 5, 228-234.
Shaw LM, Vanderstichele H, Knapik-Czajka M, Figurski M,
Coart E, Blennow K, Soares H, Simon AJ, Lewczuk P, Dean
RA, Siemers E, Potter W, Lee VM, Trojanowski JQ (2011)
Qualification of the analytical and clinical performance of
CSF biomarker analyses in ADNI. Acta Neuropathol 121,
597-609.
American Psychiatric Association (2013) DSM-5: Diagnostic
and Statistical Manual of Mental Disorders, Fifth Edition.
American Psychiatric Association, Washington, DC.
Dubois B (2014) Improving diagnostic criteria for
Alzheimer’s disease - An update from the International
Working Group. Lancet Neurol, in press.
�
 Sebastiaan Engelborghs
Sebastiaan Engelborghs