OBES SURG (2011) 21:1739–1749
DOI 10.1007/s11695-010-0319-4
CLINICAL RESEARCH
Impact of Aerobic Exercise Training on Heart Rate
Variability and Functional Capacity in Obese Women
After Gastric Bypass Surgery
Viviane Castello & Rodrigo Polaquini Simões &
Daniela Bassi & Aparecida Maria Catai & Ross Arena &
Audrey Borghi-Silva
Published online: 20 November 2010
# Springer Science+Business Media, LLC 2010
Abstract
Background Obesity is a major public health concern on a
global scale. Bariatric surgery is among the treatment
options, resulting in significant and sustainable weight loss
as well as amelioration of comorbidities. The purpose of
this study was to evaluate whether a 12-week aerobic
exercise program positively impacts heart rate variability
(HRV) and functional capacity after gastric bypass surgery
(GBS) in a female cohort.
Methods Of the 52 patients initially recruited, 21 were
randomized to a training group (TG) or control group and
successfully completed the study. Patients were tested on
two occasions: 1 week before GBS and 4 months after
GBS. Anthropometric variables, body composition, record
of heart rate and R-R intervals, and 6-min walk test
V. Castello : R. P. Simões : D. Bassi : A. M. Catai :
A. Borghi-Silva (*)
Cardiopulmonary Physiotherapy Laboratory, Nucleus of Research
in Physical Exercise, Federal University of São Carlos,
Rod. Washington Luis, km 235,
13565-905, São Carlos, São Paulo, Brazil
e-mail: audrey@ufscar.br
R. Arena
Department of Internal Medicine,
Virginia Commonwealth University Richmond,
Richmond, VA, USA
R. Arena
Department of Physiology,
Virginia Commonwealth University Richmond,
Richmond, VA, USA
R. Arena
Department of Physical Therapy,
Virginia Commonwealth University Richmond,
Richmond, VA, USA
(6MWT) were assessed at both time points. The TG
underwent an aerobic exercise training program on a
treadmill (1-h session, totaling 36 sessions over 12 weeks).
Results The main findings from this study were: (1) only
the TG demonstrated a significant increase (p<0.05) in all
indexes of heart rate variability (HRV) after 12 weeks of
aerobic exercise training and (2) only the TG demonstrated
a significant increase (p<0.05) in 6MWT distance and
decrease in diastolic blood pressure after aerobic exercise
training.
Conclusions We conclude that 12 weeks of aerobic
exercise training improves cardiac autonomic modulation
and functional capacity 4 months after GBS.
Keywords Bariatric surgery . Autonomic nervous system .
Morbid obesity . Severe obesity . Body mass index . Body
composition . Physical fitness . Weight loss
Introduction
Obesity is considered one of the most serious public health
concerns throughout the world [1]. Estimates from the
World Health Organization [2] indicate that more than one
billion adults are overweight and that 300 million in this
cohort are clinically obese. Data from the Brazilian Institute
of Geography and Statistics [3] indicate that 41.1% of men
and 40% of women are overweight in this country.
Moreover, obesity impacts 13% of the total Brazilian
population with a higher rate among women (13.6%)
compared with men (12.4%) [4]. The obesity epidemic is
having a negative impact by increasing the risk of
developing insulin resistance, type II diabetes, hypertension, dyslipidemia, sleep apnea syndrome, cardiovascular
�1740
disease [5, 6], sympathetic nervous system alterations
[7, 8], musculoskeletal complications, and certain forms
of cancer [9]. In addition, obesity is often linked to a
sedentary lifestyle pattern and is associated with reduced
cardiorespiratory fitness [10]. Moreover, a reduced exercise
capacity has been related to short-term complications after
bariatric surgery [11].
Bariatric surgery is a surgical treatment option that
results in significant and sustainable weight loss, leads to an
improvement in comorbidity status, and may prevent many
complications related to obesity [12]. In particular, gastric
bypass surgery (GBS) has demonstrated favorable results
both in terms of the extent and long-term maintenance of
weight loss [13]. However, in a previous study [14]
adherence to an exercise program was the sole significant
behavioral predictor of weight loss following GBS. In
addition, Maniscalco et al. [15] showed that 1 year after
GBS, a significant increase in aerobic exercise capacity was
associated with sustained weight loss. The relationship
between improvement in aerobic fitness and weight loss
was confirmed by Tompkins et al. [16], following morbidly
obese patients 3 and 6 months after GBS.
Poor aerobic fitness in morbidly obese patients is
explained by both reduced cardiovascular function [10] as
well as a low oxidative skeletal muscle capacity [17, 18]. In
addition, reduced heart rate variability (HRV) is related to
an increased body mass index (BMI) [19] and generally
associated with increased morbidity and mortality in
longitudinal studies [20]. On the other hand, 12 weeks of
aerobic exercise training has significantly improved both
the sympathetic and parasympathetic nervous activities in
obese individuals [21] independent of weight loss. However, we are unaware of any previous study that has
investigated the effects of a physical training program after
GBS on HRV in morbidly obese patients.
The purpose of this study is to therefore evaluate
whether a 12-week aerobic exercise training program can
modify HRV and functional capacity in severely obese
women 4 months after GBS. We hypothesized that the
application of aerobic exercise training will positively alter
HRV in severely obese women after GBS. A secondary
hypothesis is that the aerobic exercise training will result in
an improvement in functional capacity.
Materials and Methods
Design and Study Population
This is a prospective randomized controlled trial. Patients
were recruited over a 2-year period (2007 to 2009) through
the gastroenterologist physician overseeing the surgical
procedure. All study assessments and the exercise training
OBES SURG (2011) 21:1739–1749
program was performed in the Cardiopulmonary Physiotherapy Laboratory at Federal University of São Carlos.
The present investigation included women with morbid
obesity (BMI ≥40 kg/m2) [2] for more than 5 years, aged
between 20 and 45 years who were undergoing a Roux-enY GBS. Exclusion criteria consisted of: (1) patients with
orthopedic or neurological conditions that would preclude
participation in an exercise program, (2) myocardial
infarction (within 6 months of study enrollment), (3)
implanted pacemaker, (4) unstable angina, (5) chronic
disturbances in heart rhythm, (6) significant acute arrhythmias, (7) valvular heart disease, (8) a past history consistent
with heart disease, (9) uncontrolled hypertension, (10)
uncontrolled diabetes mellitus, (11) concomitant surgery,
(12) chronic obstructive pulmonary disease, (13) betablocker use, (14) postmenopausal status, and (15) participation in a regular exercise program at the time of study
enrollment. The investigation was approved by the Ethics
Committee for Human Research of Institutions and all
subjects signed a written consent form prior to the initiation
of the study.
Clinical Evaluation
All patients underwent a clinical examination prior to
surgery, which was performed by a gastroenterologist and
a cardiologist. This examination consisted of a comprehensive medical history, resting 12-lead electrocardiogram
(ECG), endoscopy and blood analysis used to determine
hemoglobin, triglycerides, total cholesterol, and fractions:
low-density lipoprotein (LDL) and high-density lipoprotein
(HDL), fasting glucose, and uric acid. In addition,
spirometric measurements, regular physical activity pattern,
anthropometric data, record of heart rate (HR) and R-R
intervals (R-Ri), and 6-min walk test (6MWT) were
collected before gastric bypass surgery (BGBS) as detailed
in the “Experimental Procedures” section.
Surgical Procedure
As previously indicated, all subjects in the present study
underwent a Roux-en-Y GBS, which can be described as a
combination of a restrictive and malabsorptive procedure.
Through a midline incision supraumbilical, a small stomach
pouch was first separated from the distal stomach; then, a
Y-shaped section of the small intestine was connected to the
gastric pouch to bypass the duodenum and a part of the
jejunum. Finally, this bypassed portion of the intestine was
attached more distally to the small bowel [22]. The patients
were admitted to hospital on the morning of surgery, after a
fasting period of 12 h, and the mean hospital stay was
3 days. Lastly, no subject in the present study had
postoperative complications.
�OBES SURG (2011) 21:1739–1749
Experimental Procedures
One month after GBS, the patients were randomized by
using sequentially numbered, sealed, opaque envelopes into
two groups: training group (TG) and control group (CG).
All evaluations were made 1 week BGBS and 4 months
after GBS (4GBS). Maximal exercise testing was applied
1 month after GBS to assist in prescribing an individualized
exercise training program.
All subjects were evaluated in the morning to avoid
differing physiologic responses due to circadian changes
and were instructed to avoid caffeinated and alcoholic
beverages or any other stimulants the night before and the
day of data collection. In addition, subjects were instructed
to not perform activities requiring moderate-to-heavy
physical exertion the day before the application of the
protocols. All experiments were carried out in a climatically
controlled room at 22–24°C and relative air humidity at
50–60%.
1741
b. Skinfold Thickness
The skinfolds of the biceps, triceps, subscapular,
suprailiac, abdomen, and thigh were measured thrice
using metal calipers (Cescorf, Porto Alegre, Rio
Grande do Sul, Brazil), and the average was used
[27]. The analysis of percent of fat mass (FM%) and
lean mass (LM) in kilograms was performed using four
skinfolds (biceps, triceps, subscapular, and suprailiac),
as suggested by Durnin and Womersley [28].
c. Body Circumferences
We measured the circumferences of arm, axillary,
xiphoid, hip, waist, and thigh using a flexible tape
measure of 0.1 cm. Waist circumference was measured
at the level of the umbilicus and the hips at the level of
the iliac crest taken with the patient in a standing
position. All measurements were performed thrice by
research in Nutritional Sciences who had been previously trained and certified to perform these procedures,
and the average was used [27].
Spirometric Measurements
Record of HR and R-Ri
The spirometric measurements were assessed to exclude
individuals with airflow obstruction. Forced vital capacity
(FVC) and forced expiratory volume in 1 s (FEV1)
assessments were performed using a spirometer (MedGraphics CPFS/D™ USB, St. Paul, MN, USA) with a
calibrated pneumotachograph according to ATS standardization [23], and exclusion criteria was set at a FEV1/FVC
<0.70 (GOLD) [24]. The values obtained were compared to
the predicted normal values of Knudson et al. [25].
First, the subjects were maintained at rest in the supine
position for approximately 10 min to ensure that a true
resting HR value was obtained. Subsequently, the HR and
R-Ri were recorded at rest in the supine position for 10 min
with a cardiofrequencimeter (Polar S810i, Kempele, Oulu,
Finland) fixed on the chest and with simultaneous transmission to the watch that stored the data; then, the data
were transferred to a computer through an interface (Polar
Advantage, Kempele, Oulu, Finland) for further analysis.
Regular Physical Activity Pattern
6MWT
Physical activity patterns were assessed by information
regarding occupation, sports activities and leisure habits
through the modified Baecke questionnaire for epidemiological studies [26]. This questionnaire consists of a scale
of one to five (5 representing the most active) with eight
questions pertaining to occupation, four addressing athletic
activities, and four addressing habitual leisure habits.
Results are reported as sum of scores (with minimum score
of 4.5 and maximum 14.5).
Anthropometric Variables and Body Composition
a. Body Anthropometry
Height and body weight were measured with women
barefoot and light clothing to the nearest 1 mm and
0.1 kg, respectively, with an stadiometer (Welmy
R-110, Santa Barbara do Oeste, São Paulo, Brazil).
BMI was calculated by dividing the body weight in
kilograms by the square of height in meters (kg/m2).
Two tests were performed on alternating days, and the
result of second 6MWT was considered for analysis [29].
The test was performed according to the recommendations
of ATS [29], and the women were instructed to walk as fast
as possible without running on a flat surface, 30 m long in
6 min. All subjects were given standardized encouragement
during the test. Maximal dyspnea (assessed with the 0–10
Borg scale) [30] was obtained after the test, while HR and
blood pressure (BP) were obtained immediately before and
after 6MWT.
Maximal Exercise Testing
Maximal exercise testing was performed by a physician
1 month after GBS, to evaluate aerobic capacity and
determine exercise training intensity. An incremental
symptom-limited exercise test was performed on a treadmill
(Imbramed master ATL, Porto Alegre, Rio Grande do Sul,
�1742
Brazil) using the modified Bruce protocol [31]. Subjects
were continuously monitored by ECG (Ecafix TC 500, São
Paulo, São Paulo, Brazil). At the terminal portion of each
stage of the exercise test, BP was measured by an indirect
method, using a sphygmomanometer (BD, São Paulo, São
Paulo, Brazil), HR was monitored by ECG and the Borg
scale assessed subjective symptoms [30]. The termination
criteria of the aerobic assessment followed AHA guidelines
for exercise testing [32].
Physical Training Protocol
Forty-eight hours following the maximal exercise test, the
TG initiated the aerobic exercise training program on a
treadmill. The sessions were held for 1 h on alternate days:
three times per week, for 12 weeks, totaling 36 sessions.
Each session consisted of: (1) initial 5 min of stretching the
upper and lower limbs (hamstrings, quadriceps, calves,
shoulders) and diaphragmatic breathing and awareness of
proper posture in front of a mirror in the position standing
and sitting, (2) 5 min of warm up on a treadmill at 3 km/h,
(3) 40 min of exercise on treadmill with speed and
inclination varying according to the behavior of HR; These
40 min were separated into four steps of 10 min each: step
1—intensity of exercise in which the HR remained at 50%
of HR peak reached in maximal exercise testing, step 2—
60% of HR peak, step 3—70% of HR peak, and step 4—
maintaining 70% of HR peak. (4) 1 min recovery at 3 km/
h and (5) 10 min of the same initial stretching and
diaphragmatic breathing. HR and BP were obtained at the
beginning of the session, at the end of each step, recovery,
and at the end of the session. The sessions were performed
individually and supervised by a physiotherapist.
Following the 12-week aerobic exercise training protocol, the patients were re-evaluated (anthropometric data,
record of HR and R-Ri, and 6MWT).
Heart Rate Variability Analysis
All artifacts were reviewed by visual inspection on the
computer display. Only segments with >90% pure sinus
beats were included in final analyses. The data were entered
into Kubios HRV Analysis software (MATLAB, version 2
beta, Kuopio, Finland).
HRV was analyzed with linear statistical measures in
time-domain and with non-linear. Mean of HR, standard
deviation of all N-N normal intervals (SDNN), square root
of the difference in the sum of squares between R-Ri on the
record, divided by the determined time minus one
(RMSSD), number of R-Ri differing by more than 50 ms
(NN50), and percentage of R-Ri differing by more than
50 ms (pNN50) were computed as time domain measures.
In addition, non-linear statistical measures were calculated
OBES SURG (2011) 21:1739–1749
by Poincaré plot perpendicular and along the line-ofidentity: standard deviation of instantaneous R-R interval
variability (SD1) and standard deviation of long-term
continuous R-Ri variability (SD2).
Statistical Analysis
The sample size was calculated using the GraphPad
StatMate software, version 1.01. To reach statistical
significance (p<0.05 at a power of 80% with a confidence
interval of 95%), a sample of seven women was required in
each group to demonstrate a mean difference between TG
and CG. The mean difference to determine power according
to HRV was 6 as derived from previous investigations [33].
Anticipating a dropout rate of 30%, we randomized a total
of 32 patients.
The Kolmogorov–Smirnov test was used to investigate
the data distribution, and it confirmed that the distribution
was normal. The data were then expressed as means and
standard error (SE; for a 95% confidence interval). Fisher’s
exact test for categorical data was compared with variables
between two groups. The paired Student t test was used to
compare the variables before and after 4 months following
GBS and unpaired Student t test compared differences
between the TG and CG. The gain obtained by the groups
was derived from absolute delta comparisons (post-treatment minus pre-treatment), and p values <0.05 were
considered significant. The analysis was carried out using
the Statistica for Windows software release 5.1 (StatSoft,
Inc, Tulsa, OK, USA) and Graphpad StateMade software
release 1.01 (Inc, San Diego, USA).
Results
We recruited 52 women who were undergoing GBS;
however, 15 were excluded due to uncontrolled hypertension (n=1), concomitant surgery (n=5), chronic obstructive
pulmonary function (n=3), beta-blocker use (n=2), and
musculoskeletal deficit (n=4). In addition, five patients did
not consent to participate in the study. Thus, 32 women
were considered eligible and were randomized to either the
TG or CG (n=16, each group). However, only 11 of TG
and ten of CG subjects successfully completed the study, as
shown in Fig. 1. Three patients in the TG dropped out of
the study due to trouble balancing work and the hours of
physical training, and two did not like to exercise due
muscle or joint pain. Furthermore, five patients of CG
refused to participate in the reassessment (three lived in
another city, which prevented re-evaluation, and two did
not show interest in continuing the study due to lack of
compliance) and one patient died secondary to cancer
diagnosed post GBS.
�OBES SURG (2011) 21:1739–1749
1743
Fig. 1 Flowchart showing
patient participation in the study
n number of individuals, COPD
chronic obstructive pulmonary
disease, TG trained group, CG
control group
The initial evaluation demonstrated that the women
presented with some degree of cardiac risk factors, both
in the TG as in CG; however, there was no statistical
difference between groups (Table 1). Furthermore, the use
of prescription medications was not different between
groups (Table 1).
Spirometric Measurements As listed in Table 1, there were
no significant differences between groups according to all
indexes. However, the measured values were below
predicted values in both groups.
Regular Physical Activity Pattern On the basis of the
Baecke questionnaire results, all women were considered
to be sedentary with a total score at or below 8: 19 subjects
had scores between 6 and 8, ten in the TG and nine in the
CG; and two had scores below 6, one in each group [26]. In
relation to patients who refused to continue in the study, (1)
five of the training group were classified as sedentary and
all had scores between 6 and 8 and (2) five in the control
group were also classified as sedentary; however, three had
scores between 6 and 8 and two had scores less than 6.
Anthropometric Variables and Body Composition There
were no significant differences between groups in BGBS
with respect to anthropometry, skinfold thickness, and
circumference. All patients lost weight 4 months post
GBS, independent of participation in an exercise training
program. However, when comparing BGBS with 4GBS
within groups, there were no changes in abdominal and
thigh skinfold thickness in the CG only. Additionally,
subjects in the TG experienced a significant reduction in
axillary, xiphoid, hip, waist, and thigh circumferences
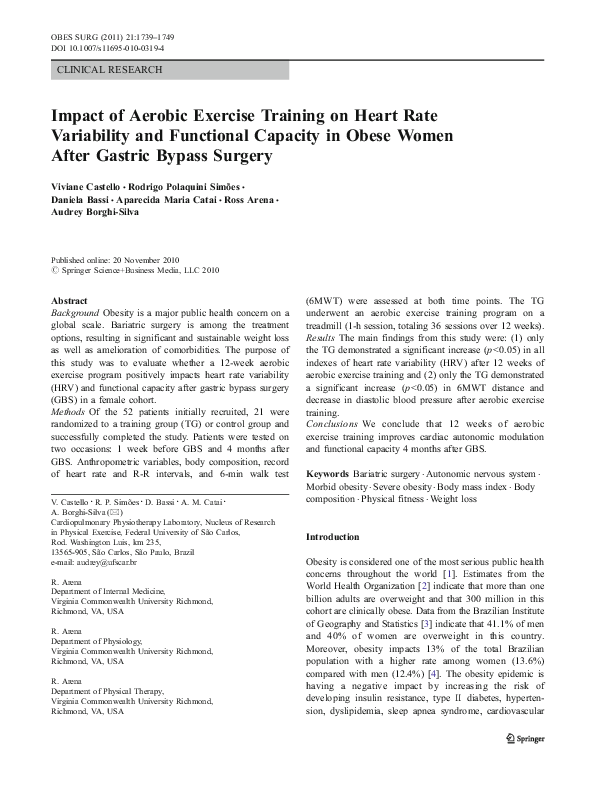
(Table 2). Delta of thigh circumference was comparable
between groups to show the effects of the aerobic physical
training (Fig. 2), and a significant reduction was observed
only the TG.
Heart Rate Variability HRV indexes are presented in
Table 3. There were no significant differences between
groups BGBS in relation to time domain and non-linear
indexes. However, following GBS, there was a significant
decrease in mean HR and increase of indexes SDNN,
RMSSD, NN50, pNN50, SD1, and SD2 in the TG only.
When comparing the TG and CG at 4GBS, only HR was
comparable. Delta of effects of aerobic exercise training on
SDNN and RMSSD index at rest were comparable between
groups (Fig. 2), while only the TG demonstrated a
significant improvement in indexes following the exercise
intervention.
�1744
OBES SURG (2011) 21:1739–1749
Table 1 Risk factors, medications, and lung function of
patients before surgery
Risk factors
Anemia
Diabetes
Dyslipidemia
Hypertension
Hypothyroidism
Smoking
Medications
Antidiabetic
Angiotensin II receptor antagonist
Angiotensin-converting enzyme inhibitors
Calcium channel blocker
Antidepressants
Contraceptive
Diuretics
Data in lung function are
presented as mean±SE. No
differences were observed
between groups
TG trained group, CG control
group, n number of individuals,
FVC forced vital capacity, FEV1
forced expiratory volume in 1 s,
pred predict
Table 2 Anthropometric
data, skinfold thickness, and
circumferences of patients
(TG and CG) before and
4 months after surgery
Data presented as mean±SE
TG trained group, CG control
group, n number of individuals,
BGBS before gastric bypass
surgery, 4GBS 4 months after
gastric bypass surgery, BMI
body mass index
a
Significant differences in relation
BGBS (TG and CG; paired
Student t test, p<0.05)
b
Significant differences between
TG vs CG (unpaired Student t test,
p<0.05)
Thyroid-stimulating hormone (TSH)
Lung function
FVC (l)
FVC (% pred)
FEV1 (l)
FEV1(% pred)
FEV1/FVC
FEV1/FVC (% pred)
TG (n=11)
CG (n=10)
2
0
1
3
2
2
1
1
1
2
1
1
1.0
0.47
1.0
1.0
1.0
1.0
0
1
1
1
4
5
3
1
1
1
0
3
3
2
0.47
1.0
1.0
1.0
1.0
0.65
1.0
2
1
1.0
3.3±0.2
94.1±3.2
2.7±0.2
91.9±4.7
79.3±3.9
93.6±4.6
3.2±0.2
92±3.6
2.8±0.2
94.5±3.6
84.9±1.8
101.9±1.9
0.95
0.66
0.58
0.66
0.20
0.11
TG (n=11)
p value
CG (n=10)
Anthropometric data
BGBS
4GBS
BGBS
4GBS
Age (years)
Height (m)
Weight (kg)
BMI (kg/m2)
Fat mass (%)
Lean mass (kg)
Skinfold thickness (cm)
38.0±4.0
1.59±0.02
117.0±4.0
45.64±1.51
45.8±1.4
63.0±3.4
–
–
94.0±4.0a
36.82±1.28a
37.8±1.2a
58.0±2.9a
36.0±4.0
1.61±0.01
117.0±6.0
44.46±0.96
42.0±1.5
67.0±1.7
–
–
94.0±5.0a
35.71±0.92a
36.0±1.1a
60.0±1.6a
Biceps
Triceps
Subscapular
Suprailiac
Abdominal
Thigh
Circumferences (cm)
Arm
Axillary
Xiphoid
Hip
Waist
Thigh
3.9±0.6
5.2±0.4
5.2±0.6
4.4±0.4
6.2±0.4
7.0±0.4
42.3±1.1
113.6±1.6
108.8±2.6
129.8±2.7
124.3±2.8
79.0±2.7
2.1±0.2a
3.4±0.2a
3.0±0.3a
2.8±0.2a
3.9±0.3a
5.0±0.4a
36.1±1a
99.8±1.8a
93.7±1.7a
115.1±2.7a
105.2±2.2a
65.9±2a
3.0±0.4
4.2±0.5
4.0±0.5
3.7±0.5
6.2±0.5
5.9±0.5
40.8±0.8
113.6±2.9
108.5±3.2
131.5±3.2
123.1±3.6
75.7±1.9
1.9±0.2a
2.9±0.3a
2.5±0.3a
2.4±0.2a
4.7±0.6
4.7±0.7
37.9±0.8a
107.9±2.7ab
102.1±2.7ab
125.2±3.3ab
116.6±3.9ab
71.5±1.9ab
�OBES SURG (2011) 21:1739–1749
1745
Fig. 2 Delta of effects of the aerobic physical training in both groups.
a SDNN: standard deviation of all N-N normal intervals. b RMSSD:
square root of the difference in the sum of squares between R-R
intervals on the record, divided by the determined time minus one. c
Walking distance of 6-min walk test × delta of lean mass. d
Circumference of thigh. Data presented as mean±SE. Single asterisk
indicates the significant differences between trained group (TG; in
gray) vs. control group (CG, in black), p<0.05
6MWT As listed in Table 3, there were no significant
differences between groups at BGBS for all 6MWT
variables. The aerobic exercise training protocol significantly increased walking distance, which was not observed
in the CG. Systolic BP decreased significantly in both
groups; however, only the TG significantly reduced
diastolic BP after the aerobic exercise training program.
Both groups significantly reduced perception of dyspnea
Table 3 Variables of heart rate variability and 6MWT of patient’s (TG and CG) before and 4 months after surgery
TG (n=11)
Time-domain
Mean HR (bpm)
SDNN (ms)
RMSSD (ms)
NN50 (ms)
pNN50 (%)
Non-linear
SD1 (ms)
SD2 (ms)
6MWT
Walking distance (m)
HR (bpm)
Systolic BP (mmHg)
Diastolic BP (mmHg)
Borg score (0–10)
BGBS
74.1±2.4
29.2±5.0
30.2±5.2
31.3±13.5
10.5±4.5
CG (n=10)
4GBS
63.7±2.8a
58.9±10.7a
67±13.9a
105.4±24.6a
35.8±8.3a
21.5±3.7
52.1±8.3
477.9±22.9
128±1.7
170.5±5.2
90.5±4.0
5.8±0.9
BGBS
4GBS
76.4±2.5
23.0±5.0
24.1±6.7
23.7±15.6
8.0±5.3
69.3±3.1
27.9±4.5b
29.4±6.4b
31.4±10.7b
10.7±16.4b
47.9±9.9a
108.8±17.2a
17.2±4.8
38.8±7.6
20.9±4.6b
51.6±7.5b
527.6±17.7a
126.2±3.9
146.6±4.0a
85.0±3.0a
3.3±0.6a
492.6±21.1
128.3±5.5
171.0±7.1
92.0±2.4
5.0±0.8
509.0±12.5
127.5±5.5
150.0±7.1a
88.8±2.4
3.8±0.5a
Data presented as mean±SE
TG trained group, CG control group, n number of individuals, BGBS before gastric bypass surgery, 4GBS 4 month after gastric bypass surgery, HR
heart rate, SDNN standard deviation of all N-N normal intervals, RMSSD square root of the difference in the sum of squares between R-R intervals
on the record, divided by the determined time minus one, NN50 the number of R-R intervals differing by more than 50 ms, pNN50 (%) percentual
of R-R intervals differing by more than 50 ms, SD1 standard deviation of instantaneous R-R interval variability, SD2 standard deviation of longterm continuous R-R interval variability, 6MWT 6-min walk test, BP blood pressure
a
Significant differences in relation BGBS (TG and CG; paired Student t test, p<0.05)
b
Significant differences between TG vs CG (unpaired Student t test, p<0.05)
�1746
and leg exertion symptoms 4GBS, without any significant
difference between groups. Figure 2 illustrates the delta of
walking distance × delta of LM between TG and CG, and
only the TG demonstrated a significant increase. In relation
to patients who discontinued the study, we found that for
the distance on the 6MWT of the five subjects in the TG,
only one had a value lower than the observed mean.
Conversely, three of five subjects in the CG were below the
mean 6MWT distance.
Discussion
Summary of Findings
The main findings from this study were: (1) only the TG
showed a significant increase in all indexes of HRV after
12 weeks of aerobic exercise training, (2) only TG
demonstrated a significant increase in 6MWT distance and
decrease in diastolic BP after aerobic exercise training, and
(3) GBS reduced weight and improved the symptoms of
dyspnea, muscle fatigue, and reduced systolic BP and HR
independent of aerobic exercise training.
Importance of this Study and Methodological
Considerations
To our knowledge, this is the first study to evaluate the
effects of aerobic exercise training after GBS on HRV in
women with morbid obesity. Previous studies reported the
effects of GBS and the benefits of an exercise program on
physical fitness [5, 34], without assessment of cardiac
autonomic control of HR. The effects of aerobic exercise
training on the autonomic nervous system have been
assessed in obese middle-age subjects who did not undergo
GBS and significant improvement of sympathetic and
parasympathetic nervous system were observed, suggesting
a possible reversal effect of human autonomic nervous
system dysfunction brought about by excess body weight
and inactivity [21].
In relation to dropout rate, we believe that some of the
participants refused to participate of study secondary to the
observation that obese individuals have low adherence
(60–70% dropout) to physical training programs as described by Dishman et al. [35].
Risk Factors, Medications, and Spirometric Measurements
As listed in Table 1, there were no differences regarding
risk factors, current medication, and spirometric variables
between the TC and CG, suggesting that the groups were
homogeneous after randomization. In relation to spiro-
OBES SURG (2011) 21:1739–1749
metric variables, we used these measures to ensure
exclusion of individuals with airflow obstruction
(Fig. 1), as it is known that these individuals with this
pulmonary condition have changes in autonomic cardiac
function [36].
Regular Physical Activity Pattern
The evaluation of the pattern of physical activity performed
by Baecke questionnaire showed that all women had same
level of physical activity at baseline and were classified as
sedentary. This was also the case for women who refused to
participate in the study, diminishing the possibility that
“self-selection” could have affected the results. The level of
physical activity is a factor of great importance for the
comparative analysis of HRV, as physically active individuals have a better response of cardiac autonomic behavior
as Sztajzel et al. [37] compared HRV of two trained athlete
groups with one group of sedentary individuals and
concluded that both trained groups had higher values of
parasympathetic activity than the control group.
Anthropometric Variables and Body Composition
The decrease of weight, BMI, and FM% at 4GBS in
relation to BGBS in both groups was expected, since the
surgical procedure promotes weight loss due to caloric
restriction and intestinal malabsorption [38]. Regarding
LM, the reductions observed in both groups can be
explained by high amount of weight loss, the malabsorptive
characteristic of the procedure, and the inadequate protein
intake inducing muscle atrophy [5, 39]. However, despite
the aerobic exercise program implemented in the TG, the
loss of muscle mass cannot be avoided, possibly due to the
type of exercise applied (aerobic), which promotes greater
improvement in muscle oxidative capacity than in muscle
mass [5].
Regarding skinfold thickness, only abdominal and thigh
skinfolds in CG did not improve from BGBS to 4GBS.
Therefore, more marked reductions of these skinfolds in the
group undergoing aerobic exercise training showed a
greater effect of exercise on subcutaneous adipose tissue,
particularly tissue in the lower limb muscles involved in the
type of exercise (treadmill) implemented in the present
study. This same explanation in relation to exercise with
lower limbs can be considered in relation to arm circumference, which was the only variable that showed no
difference between groups at 4GBS.
Heart Rate Variability
Regarding the CG, we did not find significant differences in
both HR and HRV comparing BGBS to 4GBS, suggesting
�OBES SURG (2011) 21:1739–1749
that the surgical procedure itself resulted in no change in
cardiac autonomic control. These results are not in
agreement with the study of Alam et al. [40] that assessed
the changes in HRV indexes 1, 6, and 12 months after
bariatric surgery and found improvement of cardiac
autonomic control 1 month following surgery. However,
these patients underwent a different type of surgery in
relation to our study (six patients underwent to laparoscopic
gastric banding and five to bilio-pancreatic diversion),
which may help to explain the difference in findings.
Some studies suggest that improvement in HRV can be
observed after reduction of at least 20% of body weight
[40] or reductions greater than 28% in BMI [41]. In the
current study, the reduction of body weight at the follow-up
assessment was 19.6% for both groups and the decrease of
BMI was 19.3% and 19.7% in TG and CG, respectively
(data not showed); this finding may help to explain why
HRV did not improve in the CG (i.e., level of weight loss
was not high enough).
However, longitudinal studies [33, 40–43] that assessed
HRV between 6 and 12 months after different techniques of
weight loss surgery found significant improvements in
relation to these indexes. Therefore, the weight loss itself
obtained by surgery seems to be effective in relation to
cardiac autonomic control over the longer term, a time
frame not incorporated into the current investigation.
Both decrease in HR and increase in HRV observed in
the TG (Table 3) suggest an improvement in cardiac
autonomic control measured in these individuals, possibly
provided by aerobic exercise training. However, the
relationship between physical training and HRV in obesity
has been controversial in some studies. Figueroa et al. [44]
evaluated 28 obese women divided into two groups: with
and without type 2 diabetes participating in 16 weeks of
aerobic exercise training with subjects walking at 65% of
peak oxygen consumption, 3 days/week at home and one
supervised session on a treadmill in the laboratory. In this
analysis, the authors did not observe changes in HRV after
16 weeks of training.
In the study by Amano et al. [21] with obese individuals
(without bariatric surgery procedure), the authors applied an
aerobic exercise training program on a cycle ergometer
(20 min at anaerobic threshold), three times/week for 12
consecutive weeks and demonstrated that HRV increased
after exercise training, without significant weight loss. de
Jong et al. [45] evaluated the impact of 6 months of caloric
restriction on autonomic function in 48 overweight individuals, demonstrating the decrease in sympathetic nervous
system and increase in parasympathetic nervous system
function does occur with weight loss but is more pronounced when the caloric restriction is combined with
exercise. These controversial findings in data might have
been at least partially the result of different intensity,
1747
duration, and frequency of the implemented exercise
training protocols as well as different subject characteristics
(gender and age) in the various studies [46]. Our data
support the hypothesis that the improvement in HRV was at
least partially due to the aerobic exercise training program
employed. Perugini et al. [47] demonstrated that HRV was
inversely correlated with insulin resistance and directly
correlated with the glucose disposition index, suggesting a
correlation between hyperinsulinemia and poor HRV. Thus,
the improvement of HRV after bariatric surgery found in
previous studies appears to be linked to improvement of
insulin resistance more so than the reduction in body
weight.
In this sense, we posit that physical exercise is an
essential part of a rehabilitation program following GBS
because it increases HDL cholesterol, lowers LDL
cholesterol, and decreases insulin resistance, subsequently reducing the risk of cardiovascular disease [48].
Exercise therapy is a non-pharmacological treatment that
improves HRV in myocardial infarction, chronic heart
failure, and revascularization patients by increasing vagal
tone and decreasing sympathetic activity [49]. In this
context, the hypothesis is that a shift toward greater vagal
modulation may also positively affect the prognosis of
these individuals. The underlying mechanisms by which
exercise training improves vagal modulation are speculative at present; however, it has been theorized that
angiotensin II and nitric oxide may be potential mediators
[49]. In this way, considering the risk factors and potential
cardiac events that this population is exposed to, we
believe that physical training should be an integral
component of their care.
6MWT
Previous studies have suggested the 6MWT can be used to
develop an exercise program during the preoperative and
postoperative phases of bariatric surgery [50], quantifying
some aspects of functional capacity in obese patients and to
monitor changes in physical fitness after an intervention. In
our study, the walking distance increased after GBS only in
the group undergoing the physical training program. For
women who refused to participate in the study, individual
values indicate that of five volunteers of training group,
four were above mean, and three were below the mean in
the control group, minimizing the possibility that the less fit
people selectively dropped out of the study.
Souza et al. [51] evaluated functional capacity using the
6MWT in severely obese subjects 1 day before and
7–12 months after Roux-en-Y gastric bypass surgery. The
average distance walked in the postoperative phase was
longer compared to the preoperative distance. Likewise, the
study by Maniscalco et al. [15] showed that in 15 severely
�1748
obese patients who underwent laparoscopic adjustable
gastric banding, the distance walked during the 6MWT
increased when compared with an assessment 1 year after
the surgical procedure.
In our study, two tests were performed because the first
test tends to underestimate exercise capacity due to lack of
familiarity with the subject’s test [29]. Moreover, we
excluded patients with orthopedic or neurological conditions and cardiorespiratory complication, which may limit
walking performance in obese. Thus, our findings show
that a short period of 4 months after the GBS was unable to
improve the functional capacity of women assessed by the
6MWT differently of group submitted to physical training.
These findings demonstrate that the increased walking
distance does not occur only in consequence of weight
reduction, and that adherence to a training program can
elicit positive changes in functional capacity after bariatric
surgery.
The present study also showed that the systolic BP
decreased significantly after the GBS in both groups;
however, only TG significantly reduced diastolic BP,
possibly provided by aerobic exercise training. According
to Lewington et al. [52], reductions of 10 and 5 mmHg in
systolic and diastolic blood pressure, respectively, could
decrease the long-term risk of death by ischemic heart
diseases by about 40%. In our study, we observed a
significant reduction of systolic BP (mean) after the GBS
by approximately 24 mmHg for the TG and 21 mmHg in
the CG, but in relation to diastolic BP the mean reduction
was 5.5 mmHg in the TG and approximately 3 mmHg for
the CG. This decrease in diastolic blood pressure is
possibly due to a decrease in peripheral vascular resistance
caused by improvement of vasodilatation of skeletal muscle
after the aerobic exercise training program [53].
One limitation of the study was that the women included
were not evaluated by ergospirometry to assess functional
capacity or the prescription of physical training, a limitation
that must be rectified by future investigations. In addition,
further studies are needed to assess whether the improvement in autonomic function reduces cardiovascular morbidity and mortality in a population of severely obese
women after bariatric surgery. Also, more information
related to the behavior of HRV in trained and untrained
individuals in the long term (i.e., ≥12 months post GBS) is
needed. However, the current investigation is important in
demonstrating only 4 months of physical training is a
valuable non-pharmacological treatment in improving important physiologic variables such as HRV.
We conclude that a 12-week aerobic exercise training
program improves cardiac autonomic modulation and
functional capacity in obese women 4 months after GBS.
In this way, aerobic physical training can produce marked
and faster benefits after GBS.
OBES SURG (2011) 21:1739–1749
Acknowledgements The authors would like to thank the Fundação
de Amparo à Pesquisa do Estado de São Paulo (FAPESP-07/53202-9)
and the Coordenação de Aperfeiçoamento de Pessoal de Nível
Superior (CAPES) for providing both financial and material support.
In addition, the authors also thank the medical gastroenterologists:
Noé Carvalho Azambuja Jr and João do Nascimento Ortega. More
importantly, however, the authors thank the patients for their effort and
enthusiastic cooperation throughout the study.
Conflict of Interest The authors declare that they have no conflict
of interest related to the article or the research described.
References
1. Wang Y, Beydoun MA. The obesity epidemic in the United States—
gender, age, socioeconomic, racial/ethnic, and geographic characteristics: systematic review and meta-regression analysis. Epidemiol
Rev. 2007;29:6–28.
2. World Health Organization (WHO). Obesity: preventing and
managing the global epidemic: report of a WHO consultation.
Geneva: World Health Organization; 2000. Technical report series
no. 894.
3. Brazilian Institute of Geography and Statistics. Household Budget
Survey 2002–2003. Available at: http://www.abeso.org.br (last
accessed 20 April 2010).
4. Ministry of Health of Brazil. Vigitel Brazil 2008: monitoring of
risk and protective factors for chronic diseases through telephone
survey/Ministry of Health, Secretariat of Health Surveillance,
Secretariat for Strategic and Participative Management. Brasilia,
2009.
5. Stegen S, Derave W, Calders P, et al. Physical fitness in morbidly
obese patients: effect of gastric bypass surgery and exercise
training. Obes Surg. 2009 [Epub ahead of print].
6. National Task Force on the Prevention and Treatment of Obesity.
Overweight, obesity, and health risk. Arch Intern Med.
2000;160:898–904.
7. Bobbioni-Harsch E, Bongard O, Habicht F, et al. Relationship
between sympathetic reactivity and body weight loss in morbidly
obese subjects. Int J Obes. 2004;28:906–11.
8. Davy KP, Orr JS. Sympathetic nervous system behavior in human
obesity. Neurosci Biobehav Rev. 2009;33:116–24.
9. Schelbert KB. Comorbidities of obesity. Prim Care Clin Off Pract.
2009;36:271–85.
10. Vanhecke TE, Franklin BA, Miller WM, et al. Cardiorespiratory
fitness and sedentary lifestyle in the morbidly obese. Clin Cardiol.
2009;32:121–4.
11. McCullough PA, Gallagher MJ, Dejong AT, et al. Cardiorespiratory fitness and short-term complications after bariatric surgery.
Chest. 2006;130:517–25.
12. Cowan Jr GS, Hiler ML, Buffington C. Criteria for selection of
patients for bariatric surgery. Eur J Gastroenterol. 1999;11:69–75.
13. Jones Jr KB. Experience with Roux-en-Y gastric bypass, and
commentary on current trends. Obes Surg. 2000;10:183–5.
14. Welch G, Wesolowski C, Piepul B, et al. Physical activity predicts
weight loss following gastric bypass surgery: findings from a
support group survey. Obes Surg. 2008;18:517–24.
15. Maniscalco M, Zedda A, Giardiello C, et al. Effect of bariatric
surgery on the six-minute walk test in severe uncomplicated
obesity. Obes Surg. 2006;16:836–41.
16. Tompkins J, Bosch PR, Chenowith R, et al. Changes in functional
walking distance and health-related quality of life after gastric
bypass surgery. Phys Ther. 2008;88:928–35.
17. Cortright RN, Sandhoff KM, Basilio JL, et al. Skeletal muscle fat
oxidation is increased in African-American and white women
�OBES SURG (2011) 21:1739–1749
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
after 10 days of endurance exercise training. Obesity.
2006;14:1201–10.
Privette JD, Hickner RC, Macdonald KG, et al. Fatty acid
oxidation by skeletal muscle homogenates from morbidly obese
black and white American women. Metabolism. 2003;52:735–8.
Felber Dietrich D, Ackermann-Liebrich U, Schindler C, et al.
Effect of physical activity on heart rate variability in normal
weight, overweight and obese subjects: results from the SAPALDIA study. Eur J Appl Physiol. 2008;104:557–65.
Bigger Jr JT, Fleiss JL, Rolnitzky LM, et al. Frequency domain
measures of heart period variability to assess risk late after
myocardial infarction. J Am Coll Cardiol. 1993;21:729–36.
Amano M, Kanda T, Ue H, et al. Exercise training and autonomic
nervous system activity in obese individuals. Med Sci Sports
Exerc. 2001;33:1287–91.
Bobbioni-Harsch E, Sztajzel J, Barthassat V, et al. The effect of
insulin on cardiac autonomic balance predicts weight reduction
after gastric bypass. Diabetologia. 2005;48:1258–63.
American Thoracic Society. Standardisation of spirometry. Eur
Respir J. 2005;26:1104–9.
Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the
diagnosis, management, and prevention of COPD. Am J Respir
Crit Care Med. 2007;176:532–55.
Knudson RJ, Lebowitz MD, Holberg CJ, et al. Changes in the
normal maximal expiration flow-volume curve with growth and
aging. Am Rev Respir Dis. 1983;127:725–34.
Baecke JAH, Burema J, Frijters JER. A short questionnaire for the
measurement of habitual physical activity in epidemiological
studies. Am J Clin Nutr. 1982;36:936–42.
Bredella MA, Utz AL, Torriani M, et al. Anthropometry, CT, and
DXA as predictors of GH deficiency in premenopausal women:
ROC curve analysis. J Appl Physiol. 2009;106:418–22.
Durnin JVG, Womersley P. Body fat assessed from total body
density and its estimation from skinfold tickness: measurement in
481 men and women aged from 16 to 72 years. Br J Nutr.
1974;32:77–9.
ATS statement: guidelines for the six-minute walk test. Am J
Respir Crit Care Med. 2002; 166:111–7.
Borg GA. Psychophysical bases of perceived exertion. Med Sci
Sports Exerc. 1982;14:377–81.
Bruce RA, Kusumi F, Hosmer D. Maximal oxygen intake and
nomographic assessment of functional aerobic impairment in
cardiovascular disease. Am Heart J. 1973;85:546–62.
Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002
guideline update for exercise testing: summary article: a report of
the American college of cardiology/American heart association
task force on practice guidelines (Committee to update the 1997
exercise testing guidelines). Circulation. 2002;106:1883–92.
Nault I, Nadreau E, Paquet C, et al. Impact of bariatric surgeryinduced weight loss on heart rate variability. Metabolism.
2007;56:1425–30.
Josbeno DA, Jakicic JM, Hergenroeder A, et al. Physical activity
and physical function changes in obese individuals after gastric
bypass surgery. Surg Obes Relat Dis. 2008;6:361–6.
Dishman RK, Buckworth J. Increasing physical activity: a
quantitative synthesis. Med Sci Sports Exerc. 1996;28:706–19.
1749
36. Reis MS, Arena R, Deus AP, et al. Deep breathing heart rate
variability is associated with respiratory muscle weakness in
patients with chronic obstructive pulmonary disease. Clinics.
2010;65:369–75.
37. Sztaizel J, Jung M, Sievert K, et al. Cardiac autonomic profile in
different sports disciplines during all-day activity. J Sports Med
Phys Fitness. 2008;48:495–501.
38. Zalesin KC, Franklin BA, Lillystone MA, et al. Differential loss
of fat and lean mass in the morbidly obese after bariatric surgery.
Metab Syndr Relat Disord. 2010;8:15–20.
39. Poitou BC, Ciangura C, Coupaye M, et al. Nutritional deficiency
after gastric bypass: diagnosis, prevention and treatment. Diabet
Metab. 2007;33:13–24.
40. Alam I, Lewis MJ, Lewis KE, et al. Influence of bariatric surgery
on indices of cardiac autonomic control. Auton Neurosci.
2009;151:168–73.
41. Maser RE, Lenhard MJ, Irgau I, et al. Impact of surgically induced
weight loss on cardiovascular autonomic function: one-year
follow-up. Obesity. 2007;15:364–9.
42. Machado MB, Velasco IT, Scalabrini-Neto A. Gastric bypass and
cardiac autonomic activity: influence of gender and age. Obes
Surg. 2009;19:332–8.
43. Karason K, Mølgaard H, Wikstrand J, et al. Heart rate variability
in obesity and the effect of weight loss. Am J Cardiol.
1999;83:1242–7.
44. Figueroa A, Baynard T, Fernhall B, et al. Endurance training
improves post-exercise cardiac autonomic modulation in obese
women with and without type 2 diabetes. Eur J Appl Physiol.
2007;100:437–44.
45. de Jong L, Moreira EA, Martin CK, et al. Team. Impact of 6month caloric restriction on autonomic nervous system activity in
healthy, overweight, individuals. Obesity. 2010;18:414–6.
46. Hottenrott K, Hoos O, Esperer HD. Heart rate variability and
physical exercise. Current status. Herz. 2006;31:544–52.
47. Perugini RA, Li Y, Rosenthal L, et al. Reduced heart rate
variability correlates with insulin resistance but not with measures
of obesity in population undergoing laparoscopic Roux-en-Y
gastric bypass. Surg Obes Relat Dis. 2010;6:237–41.
48. Kraus WE, Slentz CA. Exercise training, lipid regulation, and
insulin action: a tangled web of cause and effect. Obesity.
2009;17:S21–6.
49. Routledge FS, Campbell TS, McFetridge-Durdle JA, et al.
Improvements in heart rate variability with exercise therapy. Can
J Cardiol. 2010;26:303–12.
50. Enright PL. The six-minute walk test. Respir Care. 2003;48:783–
5.
51. Souza SAF, Faintuch J, Fabris SM, et al. Six-minute walk test:
functional capacity of severely obese before and after bariatric
surgery. Surg Obes Relat Dis. 2009;5:540–3.
52. Lewington S, Clarke R, Qizilbash N, et al. Age-specific relevance
of usual blood pressure to vascular mortality: a meta-analysis of
individual data for one million adults in 61 prospective studies.
Lancet. 2002;360:1903–13.
53. Pescatello LS, Franklin BA, Fagard R, et al. American college of
sports medicine position stand. Exercise and hypertension. Med
Sci Sports Exerc. 2004;36:533–53.
�
 Daniela Bassi
Daniela Bassi