International Journal of Drug Policy 22 (2011) 292–300
Contents lists available at ScienceDirect
International Journal of Drug Policy
journal homepage: www.elsevier.com/locate/drugpo
Research paper
Uptake, benefits of and barriers to safer crack use kit (SCUK) distribution
programmes in Victoria, Canada—A qualitative exploration
Andrew Ivsins a,b , Eric Roth b,c , Nadine Nakamura d , Mel Krajden e , Benedikt Fischer d,f,∗
a
Department of Sociology, University of Victoria, PO Box 3050, STN CSC, Victoria, BC, Canada V8W 3P5
Centre for Addictions Research of BC, Room 273-2300, McKenzie Avenue, Victoria, BC, Canada V8P 5C2
Department of Anthropology, University of Victoria, P.O. Box 3050, STN CSC, Victoria, BC, Canada V8W 3P5
d
Centre for Applied Research in Mental Health and Addiction, Faculty of Health Sciences, Simon Fraser University, 2400-515 West Hastings Street, Vancouver, BC, Canada V6B 5K3
e
BC Centre for Disease Control, 655 West 12th Avenue, Vancouver, BC, Canada V5Z 4R4
f
Centre for Addiction and Mental Health, 33 Russell Street, Toronto, Ontario, Canada M6J 1H4
b
c
a r t i c l e
i n f o
Article history:
Received 5 October 2010
Received in revised form 4 May 2011
Accepted 7 May 2011
Keywords:
Crack use
Community health
Hepatitis C virus
Harm reduction
Safer crack use kit
Canada
a b s t r a c t
Background: Crack use is prevalent amongst street drug users in Canadian cities, and associated with
severe drug use, health and social problems. Whilst few targeted interventions are available for crack
use, the common use and sharing of hazardous makeshift paraphernalia are a key concern, as these risks
may be associated with oral injury and blood-borne virus (BBV) – e.g., hepatitis C virus (HCV) – transmission amongst users. Recently, distribution programmes of so-called ‘safer crack use kits’ (SCUKs) have
been initiated in select Canadian cities, primarily to reduce the use of unsafe materials and paraphernalia sharing amongst crack users. This study explored uptake and benefits of, barriers to, and possible
improvements to two recently implemented SCUK distribution programme in Victoria, Canada.
Methods: N = 31 regular crack smokers were recruited through community-based efforts between June
and August 2010, and assessed via an interviewer-administered protocol involving quantitative and
qualitative data items. Descriptive analyses were completed with the quantitative data, and thematic
content analyses were conducted with the qualitative data in order to identify and extract prominent
themes and issues.
Results: The sample indicated high levels of socio-economic marginalization, poly-substance use, health
problems, lengthy crack use histories and common crack paraphernalia sharing. Most participants exclusively utilized the SCUK programme including glass-stems in addition to other paraphernalia materials.
Participants described: lesser need to share – or to commit property crimes to obtain resources for – crack
to paraphernalia, increased health awareness, and increased personal and community safety as benefits
experienced from SCUK use. Limitations in SCUK resources and distribution, shortcomings in materials,
and police interference were cited as barriers to current SCUK program delivery.
Conclusions: SCUK distribution in Victoria appears to result in a variety of individual and community
health benefits. These benefits could be solidified by addressing current programme limitations, including
better resourcing, expanding geographic distributions and eliminating police interference.
© 2011 Elsevier B.V. All rights reserved.
Background
Crack use is highly prevalent amongst street drug users in
Canada, and has substantially increased in recent years (DeBeck
et al., 2009; Fischer, Firestone Cruz, & Rehm, 2006; Fischer,
Manzoni, & Rehm, 2006; Fischer, Rehm, et al., 2006; Haydon &
Fischer, 2005; Health Canada, 2006; Werb et al., 2010). In a multi-
∗ Corresponding author at: Centre for Applied Research in Mental Health and
Addiction (CARMHA), Faculty of Health Sciences, Simon Fraser University, 2400515 West Hastings Street, Vancouver, BC, Canada V6B 5K3. Tel.: +1 778 782 5148;
fax: +1 778 782 7768.
E-mail addresses: bfischer@sfu.ca, Benedikt Fischer@camh.net (B. Fischer).
0955-3959/$ – see front matter © 2011 Elsevier B.V. All rights reserved.
doi:10.1016/j.drugpo.2011.05.005
site study of illicit opioid and other drug users across Canada,
approximately half of the sample had used crack in the previous 30
days (Fischer, Firestone Cruz, et al., 2006; Fischer, Manzoni, et al.,
2006; Fischer, Rehm, et al., 2006). Similarly, the most recent (2006)
I-Track study assessing samples of injection drug users (IDUs) in
multiple cities across Canada found 65.2% of participants had used
crack in the previous 6 months, up from 52.2% in 2004 (Health
Canada, 2004, 2006), whilst in a study of IDUs in Ottawa, 91% of participants reported smoking crack in the previous 6 months (Leonard
et al., 2008). Similarly, in a study of street-involved drug users in
Victoria, 87.8% of participants reported using crack in the previous
30 days (Ivsins et al., 2010). Crack is reported as the most commonly used drug in Vancouver (Boyd, Johnson, & Moffat, 2008;
CHASE Project Team, 2005), and the 2006 I-Track study found
�A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
Victoria crack use rates to be similar or higher compared to other
cities across Canada (Health Canada, 2006).
Crack use is associated with unique and serious health and
social problems. Users tend to be extremely marginalized within
drug-using networks and broader society, and are characterized by
severe poverty, homelessness, lack of access to legal income and
other resources, and barriers to health care services (Cross, Johnson,
Rees Davis, & James Liberty, 2001; DeBeck et al., 2007; Fischer &
Coghlan, 2007; Harwick & Kershaw, 2003). Several Canadian studies found crack users to be homeless or unstably housed (Fischer,
Firestone Cruz, et al., 2006; Fischer, Manzoni, et al., 2006; Fischer,
Rehm, et al., 2006; Fischer et al., 2010; Leonard et al., 2008). Crack
use is also associated with high levels of criminal involvement,
arrests and imprisonment (Bennett & Holloway, 2008; Fischer et al.,
2010; Manzoni, Brochu, Fischer, & Rehm, 2006).
Compared to other drug users, crack users are at elevated risk for
a variety of health problems, including human immunodeficiency
virus (HIV), hepatitis C virus (HCV) infection, and other bloodborne viruses (BBVs) and sexually transmitted infections (STIs)
(DeBeck et al., 2009; DeHovitz et al., 1994; Fischer, Firestone Cruz,
et al., 2006; Fischer, Manzoni, et al., 2006; Fischer, Rehm, et al.,
2006; Maranda, Han, & Rainone, 2004; Wallace, Porter, Weiner, &
Steinberg, 1997). Crack users frequently engage in high-risk sexual behaviour, such as having multiple sex partners, exchanging
sex for drugs, infrequent use of condoms, and involvement in sex
work; all of which are risk factors for transmission of BBVs or
STIs (Atkinson, Williams, Timpson, & Schonnesson, 2010; Booth,
Watters, & Chitwood, 1993; Harzke, Williams, & Bowen, 2009;
Schonnesson et al., 2008). Crack use is also associated with mental and emotional health issues such as depression (Schonnesson,
Williams, Atkinson, & Timpson, 2009).
Recent research with crack user populations identified two population specific health risk behaviours. First, users frequently use
crack pipes made from hazardous makeshift materials, including
glass fragments or metal pipes/tubing, aluminium cans, plastic
medicinal inhalers, car antenna or glass ginseng bottles, all of which
can cause cuts, sores, burns and blisters and chronic injuries in and
around the user’s oral cavity (Faruque et al., 1996; Porter & Bonilla,
1993; Porter, Bonilla, & Drucker, 1997; Shannon et al., 2008). Secondly, users commonly share crack use paraphernalia (Collins et al.,
2005; Fischer et al., 2010; Haydon & Fischer, 2005; Shannon et al.,
2006, 2008). A recent study of crack use in mid-sized BC communities found that 80% of participants reported sharing crack pipes
in the previous 30 days (Fischer et al., 2010). Data from a crack
user cohort in Ottawa found that 72% of participants reported sharing crack pipes in the previous six months, whilst 90% reported
sharing a pipe in the one month prior to the assessment (Leonard
et al., 2008). Amongst a sample of Vancouver crack smokers, 80%
reported sharing pipes or mouthpieces (Malchy, Bungay, & Johnson,
2008).
Sharing crack use paraphernalia has been hypothesized to
potentially facilitate BBV transmission amongst users. Several studies have found crack users – including samples with no injecting
history – to feature substantially elevated BBV rates, specifically for
HCV (McMahon & Tortu, 2003; Marcias et al., 2008; Roy et al., 2001;
Tortu, Neaigus, McMahon, & Hagen, 2001) leading to the hypothesis that the sharing of crack use paraphernalia in combination
with oral injuries, may be a possible pathway of HCV transmission
amongst crack users (Scheinmann et al., 2007; Tortu, McMahon,
Pouget, & Hamid, 2004). Indeed, a recent study examining the presence of the HCV on crack pipes suggested that HCV transmission by
way of crack paraphernalia sharing may be possible (Fischer, Powis,
Firestone Cruz, Rudzinski, & Rehm, 2008). Given that HCV is several times more infective than HIV via blood contact, and the high
rates of HCV amongst crack using populations, this is of particular
concern (Sulkowski & Thomas, 2003).
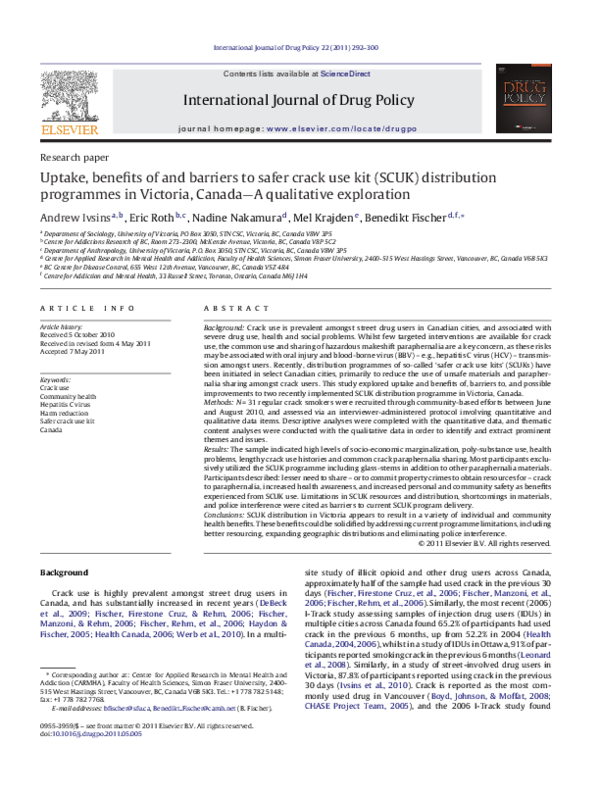
293
Fig. 1. Content material of a ‘safer crack use kit’.
Despite the prevalence of crack use and related health and social
problems, few drug intervention programmes exist in Canada tailored for crack users (Boyd et al., 2008; Fischer & Coghlan, 2007;
Bungay, Johnson, Varcoe, & Boyd, 2010). In Europe, several countries offer ‘safer inhalation facilities’ rooms for crack users, although
proposals for such facilities have been rejected in Canada to date
(EMCDDA, 2007; Fischer & Allard, 2007; Shannon et al., 2006).
In contrast, the distribution of ‘safer crack use kits’ (SCUK) to
crack users is a more easily feasible initiative due to light resource
requirements and flexible delivery options, and has been implemented in a select few cities across Canada in recent years (Haydon
& Fischer, 2005). Similar to sterile needle exchange/distribution
for injection drug users, SCUK distribution is a secondary prevention measure aimed at providing safer crack use paraphernalia [i.e.,
borosilicate (e.g., Pyrex) glass stems, rubber mouthpieces, brass
screens] to allow users to assemble their own pipes as a means of
reducing unsafe paraphernalia use and sharing. Whilst SCUK programmes in Ottawa, Ontario and Nanaimo, British Columbia (BC),
were temporarily suspended due to political opposition, SCUKs
have been distributed in Victoria, BC since 2007 (James, 2007;
O’Byrne & Holmes, 2008). Figs. 1 and 2 present illustrations of a
SCUK and its constituent parts.
Crack use paraphernalia distribution in Victoria, BC
SCUK programme delivery in Victoria happens in a distinct
wider programme and policy context. Formally – based on the
Fig. 2. Glass-stem crack pipe with filter.
�294
A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
Downtown Health Initiative Plan Action Plan – Victoria subscribes
to a ‘Four Pillars’ approach to street drug use – consisting of an
“overarching goal of . . . harm reduction” as well as prevention,
treatment and enforcement – jointly developed, implemented by
the City of Victoria, the local Vancouver Island Health Authority
(VIHA) and the Victoria Police Department (City of Victoria, 2004).
Most services to street drug users are delivered by local health and
social service agencies which receive targeted funding from VIHA.
Both local services as well institutional politics related to street
drug use have been experiencing severe disruptions and strain over
the past two years, since Victoria’s only fixed needle exchange service – run by AVI – was shut down in late 2008 due to local business
and neighbourhood pressures (MacNeil & Pauly, 2010). Since then,
the VIHA and the City have failed to identify a new location for
the fixed NEP, and local police – under a new police chief and
in the context of a new mayor – have conducted more aggressive law enforcement and policing against street drug users. The
delivery and distribution of public health services and materials to
street drug users in Victoria has further been constrained by the
fact that services are restricted by “no-service-areas”, i.e. to not
include areas in front of residences, open business, schools or daycares. This restriction is commonly referred to as the existence of
“no-go-zones” by some local service providers.
Currently, two distinct SCUK initiatives operate in Victoria. The
first SCUK (referred to as ‘SCUK-sans-stem’ from here-on in) is a
programme that includes rubber mouthpieces and pushsticks, but
no glass stem centrepieces. The idea behind this approach is that
crack users will use the rubber mouthpieces provided on existing
glass stems or makeshift material pipes from other sources in their
or others’ possession, and hence reduce direct contact or exposure to the pipe material. The materials for the SCUK-sans-stem
programme are provided by the BC Centre for Disease Control’s
(BCCDC) Provincial Harm Reduction Program and disseminated by a
variety of social/health service agencies in Victoria receiving operational funds from VIHA, including the Society for Living Intravenous
Drug Users (SOLID), PEERS Victoria Resource Society (an organization providing support for former and current sex workers), Cool
Aid Society street nurses, and Vancouver Island Health Authority
(VIHA) street nurses. Based on community sources, the SCUK-sansstem programme was expected to distribute about 600–1000 SCUK
units per week upon implementation in 2009.
The second SCUK initiative – implemented by AIDS Vancouver
Island (AVI) through their Street Outreach Services (SOS) – has
operated in Victoria since 2007. In addition to mouthpieces and
push sticks contained in the VIHA funded programme, the AVISCUK programme includes glass stems, brass screens, and health
information. However, due to funding limitations, AVI’s ability to
distribute pipes in their SCUKs is severely limited to only 300–400
units per week, distributed via its bicycle and mobile van-based
SOS programme.
The primary objectives of this study were – in an exploratory
approach – to examine, assess and compare the uptake, potential
benefits and barriers, and changes in crack users’ risk behaviour
associated with the two SCUK distribution programmes.
Methods
Between June and August 2010, interviews were conducted with
a sample of 31 regular crack users in Victoria, BC. Study participants
were recruited with assistance by street outreach workers from
three sites in Victoria: in and around a daytime drop-in centre (Our
Place), in an evening drop-in centre/homeless shelter (Streetlink),
and from a mobile outreach van. This approach allowed access to
a cross-representation of crack users, with differing use environments and access to services.
Targeted sampling methods were used to recruit potential participants especially representing potentially diverse crack user
sub-populations existent in Victoria (Watters & Biernacki, 1989).
In order to be eligible, prospective participants had to be: (1)
at least 19 years old, (2) regular crack users (defined as having
used crack on at least half of the past 30 days), (3) using crack
for at least the previous 6 months, (4) willing and able to participate in the study protocol and, (5) not severely intoxicated at
the time of the interview. After eligibility screening and obtaining consent, eligible participants were interviewed in a private
location at either of the three study sites. Interviews followed
a structured questionnaire designed to collect quantitative data
on participant socio-demographics, recent drug use, health risk
behaviours, social and health service utilization, and crack paraphernalia use, and indicated a digitally audio-recorded open-ended
semi-structured interview to collect qualitative data on the benefits
of and barriers to accessing SCUKs, reasons for sharing crack pipes,
and ways to improve the current SCUK distribution programmes
(Creswell, 2003). Interviews lasted between 30 and 45 min, and participants received a $20 honorarium for their time. The study was
approved by the investigators’ respective institutional Research
Ethics Boards.
Quantitative data were entered into an Excel based databank,
and simple descriptive statistics were computed. Interviews were
transcribed, reviewed, and coded based on several layers of content
analysis (Robson, 2002). In keeping with the exploratory approach
of the present study, qualitative analyses were conducted in two
stages of coding. The first stage involved line-by-line coding to
highlight meaningful incidents, actions, events and interactions
at the level of participant description. Similar codes were then
grouped together as common or recurring concepts or units of
data. A second stage of coding involved grouping concepts thematically, inductively centring on and resulting in the main topical
areas of (1) uptake of SCUKs, (2) benefits of SCUK distribution, (3)
barriers to accessing SCUKs and, (4) ways of improving current
SCUK distribution. Codes were examined both within and across
all themes, and compared for similarities and differences. From
this, a range of major themes were identified and organized by
topical area. Illustrative quotes were extracted based on prominent
emergent themes.
Results
Sample characteristics
Table 1 presents select key socio-economic, drug use, health
and crack use characteristics of the sample. The study sample
(16 males and 15 females) aged 22–60 years were homeless or
characterized by unstable housing (70.9%) and relied on income
assistance (80.6%) or drug dealing (58.1%) for income generation.
The majority were arrested in the past year (58.1%) and currently
under judicial restraint (87.1%). About half self-reported ‘fair’ or
‘poor’ physical health (51.6%) and HCV positive status (54.8%). The
majority used heroin (64.5%), had injected drugs (67.7%) in the past
month, had used crack for at least 10 years, and had shared crack
use paraphernalia in the past 30 days (77.4%). Overall, the sample presented indicators of high socio-economic marginalization,
intensive criminal justice involvement, poor physical health with
a high prevalence of BBV, use of a variety of both injection and
non-injection drugs, and high levels of crack paraphernalia sharing.
Uptake of SCUKs
All study participants reported obtaining SCUKs from the AVI
programme, except one who did not receive harm reduction materials from any Victoria organization. Whilst other (VIHA-funded)
�A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
295
Table 1
Key characteristics of study sample N = 31, N (%).
Socio-demographics
Sex (male)
Age
Unstable housing in the past 30 days
Arrested in past year
Health
Good or excellent physical health status (N = 29)
HIV positive (self-report)
HCV positive (self-report)
Oral sores presenting the past 30 days
Crack and other drug use
Injected drugs in the past 30 days
Length of crack use (in years)
Shared crack paraphernalia in the past 30 days
Number of crack paraphernalia sharing episodes in the past 30 days (N = 24)
SCUK distribution programmes operate in Victoria (as described
above), most participants (25 of 31) only obtained SCUKs from the
AVI programme and were not even aware of the existence of the
other programmes. The majority of participants who were aware of
them described dissatisfaction with them, as they did not include
the pipe stems or centrepieces. One participant described her experience receiving a non-AVI SCUK:
“I’ve gotten one of those before. And then I got it and there was
no pipe. There was everything but. To be honest I was really
pissed off.” (SCUK29, F, 39)
Only one participant preferred SCUKs from another organization
(SOLID) because they provided pre-burnt Brillo as the filter material
for the pipe.
16 (51.6)
Mean: 39.8, median: 39, SD: 9.36, range: 22–60
22 (70.9)
18 (58.1)
18 (62.1)
5 (16.1)
17 (54.8)
8 (25.8)
21 (67.7)
Mean: 12.1, median: 10.0, SD: 8.1, range: 0.7–28.0
24 (77.4)
Mean: 4.46, median: 4.5, SD:1.69, range: 2–7
have herpes, or HIV, or a cut lip or something like that.” (SCUK30,
M, 43)
A further health benefit of SCUK distribution perceived by
respondents was that the programmes limited the need to use
makeshift or broken items as crack paraphernalia, thus reducing
the chances of cutting their lips on sharp metal edges (i.e., on
aluminium soda/beer cans) or chipped edges of glass pipes. One
participant described how he smoked crack before SCUK distribution:
“Before this I tended to end up using tiny little shards of glass
or pop cans.” (SCUK19, M, 29)
Other participants expressed the benefits from having less hazardous paraphernalia materials available.
Benefits of SCUKs
Three distinct areas of benefits of SCUK distribution emerged
from the interviews, namely health, economic and social benefits.
Health benefits
The vast majority of participants saw and experienced health
benefits related to SCUK distribution, particularly the reduced need
for crack paraphernalia sharing. Participants were aware of the
potential health risks related to sharing pipes with others and to
the health benefits of SCUK distribution in terms of limiting the
potential spread of disease. One participant described the positive
impact she believed SCUK distribution had on her health, stating:
“I don’t get sick. When I was using other people’s pipes and stuff
I noticed I got a lot more colds, flues, and stuff like that. Staph
infections. It’s a good thing, definitely.” (SCUK04, F, 40)
Similar responses revealed that the educational efforts of frontline health service providers whilst disseminating SCUKs had
informed clients of the possible health risks of pipe sharing. Many
participants were cognizant of the potential for spreading disease
by sharing crack pipes and saw SCUKs as an opportunity to lower
these risks.
“It’s keeping me clean from getting HepC, and any other mouth
diseases you can get from sharing. . .It’s like peace-of-mind for
me. You know, I don’t have to be concerned about me getting anything from anybody else. ‘Cause they [crack pipes] are
available, rather than sharing or trying to use other people’s.”
(SCUK13, F, 44)
“Getting a new pipe. . .saves me from lowering my standards
and borrowing one off a stranger or a street person that could
“You’re not ending up using a pipe or some other foreign object
that you found on the side of the road.” (SCUK21, F, 48)
“You always have a proper pipe to use, and not sharing cracked
pipes and broken pipes. Not using little broken ends of pipes
you found on the ground.” (SCUK02, F, 28)
Economic benefits
Several participants spoke about the economic benefits of SCUK
distribution, specifically the ability to save money by not having to
buy crack pipes from stores or other users. Hardware parts diverted
to and used in the assembly of makeshift crack pipes are sold in a
number of street-level stores (e.g., dollar or corner stores) in downtown Victoria, ranging in price from $3 for thin glass pipes, up to
$10 for metal, thicker glass, or Pyrex pipes. Both used and clean
makeshift pipes are also sold on the street by other users, priced
anywhere from $5 up to $20.
“Saving money, by not having to spend ten dollars to buy a pipe
everyday. . .Which cuts down on my having to [do sex] work,
which is a good thing.” (SCUK02, F, 28)
“Not paying for it. It’s free. It’s always free. . .it saves me money
everyday!” (SCUK03, M, 44)
Another participant, who was involved in sex work, described
how the SCUK distribution from the outreach van benefits her economically, stating,
“I don’t have to go away from where I’m working to get a pipe.
I don’t have to spend money on a pipe. . .The biggest benefit
is that [the outreach distributions] right down where I need to
make my money.” (SCUK15, F, 30)
�296
A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
Social benefits
Participants identified a variety of social benefits of SCUK distribution both to the crack user community and the general public. For
example, a number of participants spoke about being involved in,
or witnessing, less petty crime – such as breaking into cars for loose
change (to buy pipes) or stealing car antennas to make pipes – as a
consequence of SCUKs distribution. As one participant explained,
“Cause they’re available you’re not out there trying to steal
something to make a pipe out of.” (SCUK16, M, 43)
Similarly, some participants saw the – somewhat secluded –
location of the evening SCUK distribution from the outreach van
as benefiting the general public by keeping interactions between
service providers and crack user clients out of public view. Keeping
their activities discrete – especially from children – was particularly
important for some users.
Finally, a number of participants described reductions in negative social interactions with other crack users around crack pipes,
e.g. verbal arguments and physical violence, as a positive social
impact of SCUK distribution. One participant stated,
“It helps me not have to argue with somebody about giving me
their fucking pipe.” (SCUK06, F, 35)
Other participants illustrated the lack of pipes leading to physical violence:
“They stop not just the spread of disease, but the spread of violence. People beating up other people for their wares. . .There
are fights for gear [crack pipes] cause there is just not enough
of it.” (SCUK26, M, 32)
“A crack pipe is a weird thing in the crack world. Crack pipes are
such a personal thing, with crack people, they will fight over it.
And if there’s lack of one, it causes fights.” (SCUK27, M, 50)
Barriers to SCUK distribution
Two main themes emerged regarding problems participants had
with the current SCUK distribution programme: difficulty accessing
SCUKs and police interference.
Difficulty accessing SCUKs
The vast majority of participants reported difficulty accessing
SCUKs as a result of SOS’ limited operations in terms of times
and space. Participants commonly described problems finding the
afternoon/evening mobile outreach workers, or spoke of the limited hours of the outreach van, and thus were unable to acquire
SCUKs when needed. As one participant succinctly stated of trying
to obtain SCUKs, “It’s just a hit and miss thing” (SCUK17, F, 60).
Similar experiences were recounted by many other participants.
“Just missing them. Sometimes I don’t get out there on time.
Like they usually come around 3:00. But you gotta catch them
within that fifteen-minute window or else you miss them. . .The
[outreach] people walking around is very hit-and-miss. Like you
never know where they’re gonna be.” (SCUK08, M, 38)
“They are not always available because they no longer have an
actual place. The van can only be out here, you know, certain
times. . .People don’t always catch them when they’re riding
around on their bikes.” (SCUK04, F, 40)
Lack of SCUK supplies was another problematic issue frequently
described by participants. Encountering the street outreach team or
van, only to be told all available pipes had already been distributed
was a common experience.
“By the time you get to the van usually they’ll run out. That’s one
problem, they seem to run out of pipes pretty quick.” (SCUK08,
M, 38)
“A lot of the times you come here you don’t get one because they
only give out, what, ten [SCUKs] a day. I don’t know how many
they give out, not many. So if you’re not here right, first-come
first-served, you don’t get one.” (SCUK28, M, 42)
Not surprisingly, a great number of participants spoke of the
impact of the ‘no-go zone’ in downtown Victoria (as described
above) preventing them from readily accessing SCUKs. Restrictions
on handing out public health materials in an area where many highrisk users are located were perceived as a critically problematic
barrier to SCUK access:
“One of the problems I run into here, in Victoria, is the red
zone. The no-go zone. The [street outreach team] are somewhat restricted as to where they can go. And unfortunately the
restricted area is basically the area where everybody hangs out.”
(SCUK11, M, 53)
“Certain places they can’t give them out. You have to follow
them or walk with them. That is another pain in the ass, because
there’s certain places where we can’t go either, because of red
zones. . .It’s kind of a downfall for us when we have to follow
them certain places. Or some of us are actually sick, or we’ve got
‘street-feet’, you know some of us can’t walk that far.” (SCUK18,
F, 46)
Police interference
Just under half of participants spoke about having their crack
pipes confiscated or broken by police. Some participants also
described a sense of trepidation about carrying pipes with them,
since not being in possession of drug use paraphernalia was part of
a bail or probation order for some. Several participants described
police interference, and its perceived detrimental impact on the
aims behind the SCUK programme:
“It really bugs me when the cops sit there and they smash your
pipes. They crush them on the sidewalk. It’s stupid. Why would
you go and crush their pipes when. . .it’s supposed to be for us
to be safer. And yet they’re crushing them, and then we have
to go and share somebody else’s once we don’t have [a pipe]
anymore. . .it happens all the time.” (SCUK18, F, 46)
“Every time the cops, they just come along and squish [the crack
pipe] and smash it. So it’s defeating the purpose, because somewhere this must be costing somebody something to come up
with the pipes to give us. And then they just come along and
smash them and we’re back to square one.” (SCUK21, F, 48)
“Any paraphernalia that’s on us whatsoever gets taken away
by the cops. That should right there be mandated. Right away.
Because that paraphernalia is nothing but a safety measure.
They’re taking away a safety measure. And when they take it
away they introduce a hazard.” (SCUK26, M, 32)
Possible improvements to SCUK distribution
Participants described two main themes on ways in which the
current SCUK distribution programme could be improved: chang-
�A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
ing specific content items in the SCUKs, and enhancing outreach
and access features of the AVI programme.
Improving SCUK programming
The SCUKs distributed by AVI as used by all but one respondent contain a glass stem, wooden push-stick, brass screens, and
a mouthpiece. The vast majority of participants complained about
the brass screens included in the AVI SCUKs, preferring to use Brillo.
When asked how SCUKs could be improved, one participant replied
simply, “I don’t like the screens and I want Brillo. Straight up.”
(SCUK15, F, 30). This sentiment was shared by most participants. As
many explained, the brass screens provided are hard or impossible
to use and thus commonly discarded.
“Put Brillo instead of screens, ‘cause nobody uses the screens.
So really you’re just wasting money on getting them. Everyone’s
just throwing them out. And hand out Brillo. Which is something
that people are always in need of.” (SCUK20, F, 28)
“Realistically, we use Brillo. I do understand. . .that it isn’t
healthy. But neither is crack. And nobody uses [brass] screens.
Hardly anybody. So why you don’t just put Brillo in there
I don’t know. . .Like why not just give people the choice.
Put in both. Brillo is so cheap. Pre-burn it, like SOLID do.”
(SCUK17, F, 60)
Though not as broadly disliked as the brass screens, many participants suggested SCUKs should include better-quality pipe stems
or centrepieces, made from stronger glass, Pyrex, or even metal.
Whilst current SCUK distribution was seen as limiting the need
to use broken glass pipes, a number of participants nonetheless
reported regularly breaking or chipping the pipes they received in
the SCUKs.
“Having pyrex pipes instead of glass ones, cause then they
wouldn’t break so easily. They’re more durable and last longer.
‘Cause they don’t break easily, then people aren’t using broken
pipes as much.” (SCUK20, F, 28)
“I wish that AVI went with the Pyrex. For sure, cause if you drop
it once it’s cracked. Everyone at Streetlink has one like this [a
broken glass pipe]. I broke mine, I forgot about it, I put my hand
in my back pocket and just about took the tip of my finger off.
They break very easy.” (SCUK30, M, 43)
Improving SCUK distribution
A variety of improvements to SCUK distribution were suggested
by participants, including distribution by peers (to increase distribution contact points and coverage), increasing the hours of
distribution, and ways to connect with users and distribute SCUK
materials that are less publicly visible (e.g., not in the middle of
busy streets). Participants most commonly suggested that larger
quantities of SCUKs need to be available so that demand can be
met. As one participant concisely stated: “They need more pipes.
That’s about all.” (SCUK12, F, 38).
“They only have so many [pipes] they can hand out. And then
once they’re at their limit they can’t hand any more out. And
there’s lots of people being left out. . .Just more pipes. They
probably need more funding for that.” (SCUK04, F, 40)
Similarly, participants suggested AVI-SOS increase both their
hours of operation and spatial reach/spread across different areas
of downtown Victoria.
297
“If [SOS] did two runs a day. Cause over up at [drop-in centre],
on Pandora [Street] there, they are basically at 3:30 everyday.
And if you miss it, you don’t get it until the next day. So if they
had it at 3:30 and 7:30 it would be more convenient for other
people.” (SCUK05, M, 37)
“The one downside of the outreach team. . .is that it is comprised
of just a few people. And this is just not enough. It’s gotta have
tentacles. . .you need 5 or so more outreach vans out there, on all
hours of the night, fanning through the city. We’re just too many
people out there, and we need you guys a lot more.” (SCUK26,
M, 32)
Of particular importance to a number of participants was the
absence of a fixed distribution SCUK, e.g. as part of a fixed needle
exchange services (NES) site, as the only such site in Victoria was
closed in May 2008. SCUK distribution from a fixed NES or other
sites, in the eyes of several participants, would solve a number of
the problems regarding access to SCUKs and other safer drug use
materials distribution.
“If we had a physical place, an actual physical site that we could
go to, that would alleviate pretty well all the barriers that could
arise. Because even someone like me, who has got social issues,
can make it out there sooner or later, whenever you’re feeling
better. But now I’ve got that barrier, along with the barrier of
trying to be able to get [to SOS] first.” (SCUK19, M, 29)
Discussion
This study examined the uptake, and potential benefits, barriers,
and improvements of two recently initiated SCUK programmes in
Victoria, BC, on the basis of interviews with a small sample of regular street-entrenched crack users. SCUKs are a relatively recent –
and still controversial – intervention for the high-risk, marginalized
and growing population of crack users in Canada (Haydon & Fischer,
2005; O’Byrne & Holmes, 2008). The key aims of SCUK delivery are
to reduce crack users’ sharing of makeshift crack paraphernalia and
thus to reduce the risks of oral injury and thus potential HCV transmission, and generally to facilitate outreach efforts to the target
population (Boyd et al., 2008; Fischer & Coghlan, 2007). Currently,
only a few SCUK programmes are available in Canadian cities, and
outcome research to date has been rather limited (Fischer et al.,
2010; Leonard et al., 2008).
A first basic finding of our study is that our sample reflects
the high degree of social marginalization (e.g., high prevalence of
unstable housing, high crime involvement), poly-substance use,
and multiple health problems found for crack users in other studies (Cross et al., 2001; DeBeck et al., 2007, 2009; DeHovitz et al.,
1994; Fischer, Firestone Cruz, et al., 2006; Fischer, Manzoni, et al.,
2006; Fischer, Rehm, et al., 2006; Fischer & Coghlan, 2007; Harwick
& Kershaw, 2003; Maranda et al., 2004; Wallace et al., 1997). In
regard to the two SCUK programmes under examination, an initial observation is that the SCUK-sans-stem programme remained
virtually unrecognized and hence rather underutilized by our sample. It appears that the absence of crack pipe stems was a primary
factor, and the limited knowledge about this programme was a
secondary factor for the programme’s limited utilization. Utilization of the programme could be different outside our particular
sample, although our study relied on targeted sampling methods
towards assembling a cross-sectionally diverse sample of crack
users. Further investigation needs to examine to which extent
the SCUK-sans-stem programme is utilized at all, who utilizes it,
and how its users are different from the individuals captured by
our study sample. These insights on utilization should be helpful
especially to the health service provider organizations behind this
�298
A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
programme, i.e. the BC Provincial Harm Reduction Program and
VIHA, towards considering design and delivery improvements to
their current SCUK programming efforts for high-risk crack users.
Most respondents in our sample regularly utilized and preferred
the AVI-SCUK programme initiative including glass stem centrepieces, and illustrated multiple benefits of SCUKs. Overall, our data
provide substantive evidence that users perceived a diverse range
of significant benefits from SCUKs in health, social and economic
realms. First and foremost, whilst the biological plausibility and
epidemiological extent of the contributions of crack pipe sharing to
actual BBV transmission is tentatively documented (DeBeck et al.,
2009; Scheinmann et al., 2007; Fischer et al., 2008) our study participants clearly believed that the use of SCUK reduced users’ risk for
oral cuts and burns as well as exposure to other disease pathogens,
and improved their awareness about and responsiveness to disease
risks conveyed by educational interventions forming part of the
SCUK distribution (e.g., information from outreach workers). These
ancillary benefits for crack users are not trivial, and appear to make
SCUKs a worthwhile public health outreach and educational intervention even in the possible absence of their demonstrable ability
to effectively prevent actual BBV transmission.
Yet beyond the increased ability for users to have their own
crack pipes available, and the reduced need to share pipes, SCUKs
also generated other important benefits perceived by the target population, some of which may be somewhat unexpected.
Specifically, respondents provided testimony suggesting how the
distribution of SCUKs increased the availability of crack use paraphernalia, and hence potentially reduced dynamics leading to
interpersonal aggression or violence over rare but needed crack
paraphernalia, or the need to commit property crimes to obtain
funds or materials in order to procure crack paraphernalia (Inciardi
& Surratt, 2001; Surratt, Inciardi, Kurtz, & Kiley, 2004) These effects
– as limited as they may be in the grand scheme of things – are
noteworthy and perhaps a critical stand-alone benefits of SCUK
distribution.
As is well documented in the literature, crack use environments
as well as markets have been characterized by high degrees of
volatility as well as interpersonal violence, causing considerable
harms to individual users as well as the communities in which they
are located (Bowling, 1999; Baumer, 1994; Valdez, Kaplan, & Curtis,
2007). Several studies have described both the prevalent exposure
of crack users to violence – much of which is amplified by gendered
dynamics of violence, e.g. by way of women’s forced involvement
in high-risk sex-trade activities in the context of crack use – as well
as the extensive toll of violence and crimes on urban communities
where crack use is prevalent (Edlin et al., 1994; Jones et al., 1998;
Surratt et al., 2004). If indeed SCUK distribution help to even just
slightly reduce the prevalence of interpersonal violence, aggression and other crimes associated with the dynamics of crack use
– and this should be a focus of future systematic studies – SCUKs
would function as both a valuable individual and community health
intervention. On this basis, SCUK would deserve to be supported by
authorities concerned with crime prevention or public order as a
bona fide personal and community safety intervention. Moreover,
the experienced benefits of SCUK are diverse, ample and substantial – and come at comparably minimal actual costs and little, if
any apparent downsides or problems. To be concrete: the material
value of a SCUK unit is <$1, the overall costs of implementing SCUK
programming amounts to no more than a few $1000 in material
costs, and distribution occurs in the context of existing outreach
infrastructure – all of which is miniscule in comparison to the costs
of processing even just a few criminal arrests or charges.
In examining barriers to SCUK dissemination, several key
findings emerged. First, several participants described extensive frustration about ongoing active efforts by police to seize
and destroy crack use paraphernalia, thereby actively interfering
with or eliminating the potential benefits of the SCUK measures
described. Whilst it is not clear what police realistically intend or
expect to accomplish by such interventions, these illustrate the fallacies of ongoing drug prohibition on the ground which have been
demonstrated to be detrimental to users’ health and safety as well
as to fuel local violence in and other harms to communities (Kerr,
Small, & Wood, 2005; Maher & Dixon, 1999; Small, Rhodes, Wood,
& Kerr, 2007). Studies have documented how active police interference with public health measures like NES have contributed to risky
drug use behaviours (e.g., needle sharing, use in unsafe places),
violence and aggression related to paraphernalia access as well as
displacement of disorder and crime – these costly lessons should
not require repeating for SCUK interventions (Davis, Burris, KrautBecher, Lynch, & Metzger, 2005; Rhodes, 2002; Rhodes et al., 2003;
Small et al., 2007).
Furthermore, the juxtaposed efforts of different public agencies
unfortunately also document to what extent the ideas of supposedly concerted or constructive local drug strategies (‘Four Pillars’)
or “coordinated harm reduction programming” under municipal
umbrellas remain a practical illusion in operational practice (City
of Victoria, 2004; Fischer, 2003; Werb et al., 2008). The nature
and goals of interventions towards drug use by the realms of
enforcement and public health are based on categorically different
assumptions in key respects (Aitken, Higgs, Kelsall, & Kerger, 2002;
Fischer, 2003; Maher & Dixon, 1999). However, key municipal policy authorities in the specific context of our study should be able to
demonstrate sufficiently sensible insights and leadership to ensure
that public health measures like SCUK are not actively hindered
or undermined by law enforcement. For example, the key health
authorities behind SCUK – supported by the Provincial Health Officer and the Victoria Municipal Government – could declare SCUK
dissemination an essential public health service, and request – for
example, via the local police services board overseeing police operations – that law enforcement personnel do not interfere with SCUK
distribution or the possession of SCUK paraphernalia by crack users.
The issue of ‘no-service-areas’ in downtown Victoria – in which
SCUK or other safer drug use materials can allegedly not be distributed – poses similar challenges. Victoria is a major tourist
destination keen to uphold its pristine image to outside visitors
as well as an urban environment characterized by a core of predominantly middle-class residents and business owners not keen
on street drug users or health services catering to them disturbing
their lifestyles and livelihoods. As our data suggest, the existence
of the ‘no-service-areas’ appear to hinder distribution of SCUK for
some users keen but unable to utilize the SCUK services and instead
are likely continue to engage in higher-risk use behaviours without
them.
The situation illustrates an all too familiar dilemma in public
health programming for street drug users: it is well documented
that in order to be most effective, ground-level interventions need
to be offered as closely to users’ places of use and practical needs.
Yet at the same time, it is understandable that such interventions
cannot occur universally and everywhere, and there is an inherent systemic dynamic to push street drug users to the margins of
and minimize the presence of their deviant behaviour or disturbing impact on ‘decent’ social life or spaces (Dovey, Fitzgerald, &
Choi, 2001; Fischer & Poland, 1998; Tempalski et al., 2007). These
tensions can lead to unsatisfactory realities or outcomes of interventions aiming at marginalized populations, as illustrated in this
present SCUK case study. If the provision of effective public health
interventions for crack users in Victoria is a sincere objective, these
may need to accept the lessons of and requirements for institutionalising ‘safer use environments’ rather than just disseminating
safe use materials in the long run. This may require, for example, establishing safer crack use facilities, aiming to protect both
the health of crack users as well as to minimize harms on sur-
�A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
rounding communities (Rhodes, 2002; Rhodes et al., 2006). The
implementation of safer environments for crack users may hence
serve both sides or interests constructively, and such propositions
are not new in Victoria: a feasibility study to examine the establishment of ‘supervised drug use facilities’ in Victoria included explicit
recommendations for safer crack smoking facility components, yet
was never acted on by authorities (Fischer & Allard, 2007). These
proposals may need to be urgently revisited and reconsidered.
As documented by our data, there is clearly room for intrinsic
improvements of SCUK programming. Most simply, current SCUK
efforts are substantively hindered by limited supply resources,
leaving many users without access to SCUKs when sought or
needed. These shortages could easily be addressed by small additions of funding to the current main SCUK provider (e.g., AVI) or
by BCCDC/VIHA providing key SCUK components – specifically:
glass stem centrepieces – with the current SCUK-sans-stem programme. It would be easily and with minimal cost possible to
provide all crack users in Victoria – for the reasons and benefits
described above – with SCUKs who seek these materials. This standard is in place for NES across Canada and elsewhere, and should
be no different for SCUKs (Des-Jarlais, 2000; Strike et al., 2006;
Wodak & Cooney, 2006). Both the City of Victoria and the local
health authority, VIHA – ideally with the support of the BC Provincial Harm Reduction Program – could easily facilitate such service
improvements. Study respondents also clearly stated that they preferred ‘Brillo’ over brass material for screens included in SCUKs.
Whilst there have been health concerns regarding the former,
current SCUK distribution by AVI have made according material
adjustments. Finally, our data also provide further evidence for the
acute need for the (re-)establishment of a fixed NES-site in Victoria, through which SCUKs could also be more reliably distributed.
The closure of the Victoria fixed NES has brought detrimental consequences for public health service delivery to the sizeable IDU
population in Victoria, and currently also hinders more effective
SCUK distribution (Ivsins et al., 2010; MacNeil & Pauly, 2010).
Our study has some important limitations. It relied on a select,
non-random sample which may represent selective views and
experiences, and data can thus not be generalized to the general crack user population in Victoria or elsewhere. Our data also
rest in narrative and subjective experiences and perceptions from
study participants which were analysed and interpreted by the
researchers, with potential limitations for intrinsic and extrinsic
validity.
Importantly, this exploratory qualitative study has documented
important dynamics of uptake and impact of, and potential
improvements for SCUK dissemination for crack users in Victoria.
SCUK distribution appears to result in a variety of tangible benefits
for users, which are particularly valuable in the absence of other
solidly effective and presently available targeted health interventions for crack users. The data provided should help local service
providers guide programme planning and delivery. For future and
long-term programming and policy decisions regarding SCUK – also
on a more pan-Canadian level – more systematic and comprehensive studies are needed, including controlled observational studies
of the impacts of SCUKs for users and communities.
Acknowledgements
The investigators acknowledge grant support from the Canadian Institutes of Health Research (CIHR), specifically CIHR Catalyst
Grant No. 211803, that supported this study. Dr. Fischer furthermore acknowledges support from a CIHR/PHAC Chair in Applied
Public Health, and a Michael Smith Foundation for Health Research
(MSFHR) Senior Scholar Award. The authors also acknowledge the
active and most helpful collaboration of AVI and VIHA in facilitating
299
this study. All data presented here however were generated independently, and all opinions and interpretations stated are those of
the authors.
Conflict of interest
All authors declare that they have no conflicts of interest.
References
Aitken, C., Higgs, P., Kelsall, J., & Kerger, M. (2002). The impact of a police crackdown
on a street drug scene: Evidence from the street. International Journal of Drug
Policy, 13, 193–202.
Atkinson, J. S., Williams, M. L., Timpson, S. C., & Schonnesson, L. N. (2010). Multiple
sexual partnerships in a sample of African-American crack smokers. AIDS and
Behavior, 14, 48–58.
Baumer, E. (1994). Poverty, crack, and crime: A cross-city analysis. Journal of Research
in Crime and Delinquency, 31, 311–327.
Bennett, T., & Holloway, K. F. D. (2008). The statistical association between drug misuse and crime: A meta-analysis. Aggression and Violent Behaviour, 13, 107–118.
Booth, R., Watters, J., & Chitwood, D. (1993). HIV risk-related sex behaviors among
injection drug users, crack smokers, and injection drug users who smoke crack.
American Journal of Public Health, 83, 1144–1148.
Bowling, B. (1999). The rise and fall of New York murder: Zero tolerance or crack’s
decline? British Journal of Criminology, 39, 531–554.
Boyd, S., Johnson, J. L., & Moffat, B. (2008). Opportunities to learn and barriers
to change: Crack cocaine use in the Downtown Eastside of Vancouver. Harm
Reduction Journal, 5.
Bungay, V., Johnson, J. L., Varcoe, C., & Boyd, S. (2010). Women’s health and use of
crack cocaine in context: Structural and ‘everyday’ violence. International Journal
Drug Policy, 21, 321–329.
CHASE Project Team. (2005). Community Health And Safety Evaluation (CHASE)
Project: Final report. Vancouver: Vancouver Coastal Health Authority.
City of Victoria. (2004). Downtown health initiative: Action plan update. Victoria, BC:
Parks, Recreation & Community Development.
Collins, C. L. C., Kerr, T., Kuyper, L. M., Li, K., Tyndall, M. W., Marsh, D. C., et al. (2005).
Potential uptake and correlates of willingness to use a supervised smoking facility for noninjection illicit drug use. Journal of Urban Health, 82, 276–284.
Creswell, J. (2003). Research design: Qualitative, quantitative, and mixed methods
approaches (2nd ed.). Thousand Oaks, CA: Sage Publications.
Cross, J., Johnson, B., Rees Davis, W., & James Liberty, H. (2001). Supporting the habit:
Income generation activities of frequent crack users compared with frequent
users of other hard drugs. Drug and Alcohol Dependence, 64, 191–201.
Davis, C. S., Burris, S., Kraut-Becher, J., Lynch, K., & Metzger, D. (2005). Effects of an
intensive street-level police intervention on syringe exchange program use in
Philadelphia, PA. American Journal of Public Health, 95, 233–236.
DeBeck, K., Shannon, K., Wood, E., Li, K., Montaner, J., & Kerr, T. (2007). Income
generating activities of people who inject drugs. Drug and Alcohol Dependence,
91, 50–56.
DeBeck, K., Kerr, T., Li, K., Fischer, B., Buxton, J., & Montaner, J. (2009). Smoking of
crack cocaine as a risk factor for HIV infection among people who use injection
drugs. Canadian Medical Association Journal, 181, 585–589.
DeHovitz, J. A., Kelly, P., Feldman, J., Sierra, M. F., Clarke, L., Bromberg, J., et al. (1994).
Sexually transmitted diseases, sexual behavior, and cocaine use in inner-city
women. American Journal of Epidemiology, 40, 1125–1134.
Des-Jarlais, D. C. (2000). Structural interventions to reduce HIV transmission among
injecting drug users. AIDS, 14, S41–S46.
Dovey, K., Fitzgerald, J., & Choi, Y. (2001). Safety becomes danger: Dilemmas of druguse in public space. Health & Place, 7, 319–331.
Edlin, B. R., Irwin, K. L., Faruque, S., McCoy, C. B., Word, C., Serrano, Y., et al. (1994).
Intersecting epidemics: Crack cocaine use and HIV infection among young innercity young adults. The New England Journal of Medicine, 331, 1422–1427.
EMCDDA. (2007). Annual report 2007: The state of the drugs problem in Europe Lisbon.
Faruque, S., Edlin, B. R., McCoy, C. B., Word, C. O., Larsen, S. A., Schmid, D. S., et al.
(1996). Crack cocaine smoking and oral sores in three inner-city neighborhoods.
Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 13,
87–92.
Fischer, B. (2003). ‘Doing good with a vengeance’: A critical assessment of the
practices, effects and implications of ‘drug treatment courts’ in North America.
Criminal Justice, 3, 227–248.
Fischer, B., & Allard, C. (2007). Feasibility study on ‘Supervised Drug Consumption’
options in the City of Victoria. Victoria: Centre for Addictions Research of BC (CARBC).
Fischer, B., & Coghlan, M. (2007). Crack in North American cities: The neglected
‘epidemic’. Addiction, 102, 1340–1341.
Fischer, B., Firestone Cruz, M., & Rehm, J. (2006). Illicit opioid use and its key characteristics: A select overview and evidence from a Canadian multi-site cohort of
illicit opioid users (OPICAN). Canadian Journal of Psychiatry, 51, 624–634.
Fischer, B., Manzoni, P., & Rehm, J. (2006). Comparing injecting and non-injecting
illicit opioid users in a multisite Canadian sample (OPICAN cohort). European
Addiction Research, 12, 230–239.
Fischer, B., & Poland, B. (1998). Exclusion, risk and governance: Reflections on ‘community policing’ and ‘public health’. Geoforum, 29, 187–197.
�300
A. Ivsins et al. / International Journal of Drug Policy 22 (2011) 292–300
Fischer, B., Powis, J., Firestone Cruz, M., Rudzinski, K., & Rehm, J. (2008). Hepatitis C
virus transmission among oral crack users: Viral detection on crack paraphernalia. European Journal of Gastroenterology & Hepatology, 20, 29–32.
Fischer, B., Rehm, J., Patra, J., Kalousek, K., Haydon, E., Tyndall, M., et al. (2006). Crack
across Canada: Comparing crack and non-crack users in a multi-city cohort of
opioid and other street drug users. Addiction, 101, 1760–1770.
Fischer, B., Rudzinski, K., Ivsins, A., Gallupe, O., Patra, J., & Krajden, M. (2010). Social,
health and drug use characteristics of primary crack users in mid-sized communities in British Columbia, Canada. Drugs: Education, Prevention, and Policy,
17(4), 333–353.
Harwick, L., & Kershaw, S. (2003). The needs of crack-cocaine users: Lessons to
be learnt from a study into the needs of crack-cocaine users. Drugs: Education,
Prevention & Policy, 10, 121–135.
Harzke, A. J., Williams, M. L., & Bowen, A. M. (2009). Binge use of crack cocaine
and sexual risk behaviors among African-American, HIV-positive users. AIDS
and Behavior, 13, 1106–1118.
Haydon, E., & Fischer, B. (2005). Crack use as a public health problem in Canada –
call for an evaluation of ‘safer crack use kits’. Canadian Journal of Public Health,
96, 185–188.
Health Canada. (2004). I-Track: Enhanced surveillance of risk behaviours among injecting drug users in Canada (pilot survey report). Ottawa: Surveillance and Risk
Assessment Division, Centre for Infectious Disease Prevention and Control, Population and Public Health Branch, Health Canada.
Health Canada. (2006). Enhanced surveillance of risk behaviours among injection drug
users in Canada – Phase I report. Victoria, BC: Vancouver Island Health Authority
(VIHA).
Inciardi, J. A., & Surratt, H. L. (2001). Drug use, street crime, and sex-trading among
cocaine-dependent women: Implications for public health and criminal justice
policy. Journal of Psychoactive Drugs, 33, 379–389.
Ivsins, V., Chow, C., Marsh, D., Macdonald, S., Stockwell, T., & Vallance, K. (2010).
Drug use trends in Victoria and Vancouver, and changes in injection drug use after
the closure of Victoria’s fixed site needle exchange University of Victoria. Centre for
Addictions Research of BC.
James, D. (2007). Harm reduction policy background paper. Alberta: Alberta Alcohol
and Drug Use Commission.
Jones, D. L., Irwin, K. L., Inciardi, J., Bowser, B., Schilling, R., Word, C., et al. (1998).
The high-risk sexual practices of crack-smoking sex workers recruited from the
streets of three American cities. The Multicenter Crack Cocaine and HIV Infection
Study Team. Sexually Transmitted Diseases, 25, 187–193.
Kerr, T., Small, D., & Wood, E. (2005). The public health and social impacts of drug
market enforcement: A review of the evidence. International Journal of Drug
Policy, 16, 210–220.
Leonard, L., DeRubels, E., Pelude, L., Medd, E., Birkett, N., & Seto, J. (2008). “I inject
less as I have easier access to pipes” Injecting, and sharing of crack-smoking
materials, decline as safer crack-smoking resources are distributed. International
Journal of Drug Policy, 19, 255–264.
MacNeil, J., & Pauly, B. (2010). Impact: A case study examining the closure of a large
urban fixed site needle exchange in Canada. Harm Reduction Journal, 7 (Article
11).
Maher, L., & Dixon, D. (1999). Policing and public health: Law enforcement and
harm minimization in a street-level drug market. British Journal of Criminology,
39, 488–512.
Malchy, L., Bungay, V., & Johnson, J. (2008). Documenting practices and perceptions
of ‘safer crack use’: A Canadian pilot study. International Journal of Drug Policy,
19, 339–341.
Manzoni, P., Brochu, S., Fischer, B., & Rehm, J. (2006). Determinants of property crime
among illicit opiate users outside of treatment across Canada. Deviant Behaviour,
27, 351–376.
Maranda, M., Han, C., & Rainone, G. (2004). Crack cocaine and sex. Journal of Psychoactive Drugs, 36, 315–322.
Marcias, J., Palacios, R. B., Claro, E., Vargas, J., Vergara, S., Mira, J. A., et al. (2008).
High prevalence of hepatitis C virus infection among noninjecting drug users:
Association with sharing the inhalation implements of crack. Liver International,
28, 781–786.
McMahon, J., & Tortu, S. (2003). A potential hidden source of hepatitis C infection
among noninjecting drug users. Journal of Psychoactive Drugs, 35, 455–460.
O’Byrne, P., & Holmes, D. (2008). Evaluating crack pipe distribution in Canada: A
systems change case study. Addiction Research Theory, 16, 181–192.
Porter, J., & Bonilla, L. (1993). Crack users’ cracked lips: An additional HIV risk factor.
American Journal of Public Health, 83, 1490–1491.
Porter, J., Bonilla, L., & Drucker, E. (1997). Methods of smoking crack as a potential risk
factor for HIV infection: Crack smokers’ perceptions and behavior. Contemporary
Drug Problems, 24, 219–347.
Rhodes, T. (2002). The ‘risk environment’: A framework for understanding
and reducing drug-related harm. International Journal of Drug Policy, 13,
85–94.
Rhodes, T., Mikhailova, L., Sarang, A., Lowndes, C. M., Rylkov, A., Khutorskoy, M., et al.
(2003). Situational factors influencing drug injecting, risk reduction and syringe
exchange in Togliatti City, Russian Federation: A qualitative study of micro risk
environment. Social Science and Medicine, 57, 39–54.
Rhodes, T., Kimber, J., Small, W., Fitzgerald, J., Kerr, T., Hickman, M., et al. (2006). Public injecting and the need for safer environment interventions in the reduction
of drug related harm. Addiction, 101, 1384–1393.
Robson, C. (2002). Real world research: A resource for social scientists and
practitioner–researchers (2nd ed.). Blackwell Publishers.
Roy, E., Haley, N., Leclerc, P., Boivin, J. F., Cedras, L., & Vincelette, J. (2001). Risk factors
for hepatitis C virus infection among street youths. Canadian Medical Association
Journal, 165, 557–560.
Scheinmann, R., Hagan, H., Lelutiu-Weinberger, C., Stern, R., Des Jarlais, D. C., Flom,
P. L., et al. (2007). Non-injection drug use and hepatitis C virus: A systematic
review. Drug and Alcohol Dependence, 89, 1–12.
Schonnesson, L. N., Atkinson, J., Williams, M. L., Bowen, A., Ross, M. W., & Timpson, S.
C. (2008). A cluster analysis of drug use and sexual HIV risks and their correlates
in a sample of African-American crack cocaine smokers with HIV infection. Drug
and Alcohol Dependence, 97, 44–53.
Schonnesson, L. N., Williams, M., Atkinson, J., & Timpson, S. (2009). Factors associated
with depressive symptoms in African American crack cocaine smokers. Journal
of Substance Use, 14, 161–174.
Shannon, K., Ishida, T., Morgan, R., Bear, A., Oleson, M., Kerr, T., et al. (2006). Potential
community and public health impacts of medically supervised safer smoking
facilities for crack cocaine users. Harm Reduction Journal, 3, 1–8.
Shannon, K., Rusch, M., Morgan, R., Oleson, M., Kerr, T., & Tyndall, M. (2008). HIV and
HCV prevalence and gender-specific risk profiles of crack cocaine smokers and
dual users of injection drugs. Substance Use and Misuse, 43, 521–534.
Small, W., Rhodes, T., Wood, E., & Kerr, T. (2007). Public injection settings in Vancouver: Physical environment, social context and risk. International Journal of Drug
Policy, 18, 27–36.
Strike, C., Leonard, L., Millson, M., Anstice, S., Berkeley, N., & Medd, E. (2006). Ontario
Needle Exchange Programs: Best practice recommendations. Toronto: Ontario Needle Exchange Coordinating Committee.
Sulkowski, M. S., & Thomas, D. L. (2003). Hepatitis C in the HIV-infected person.
Annals of Internal Medicine, 138, 197.
Surratt, H. L., Inciardi, J. A., Kurtz, S. P., & Kiley, M. C. (2004). Sex work and drug use
in a subculture of violence. Crime & Delinquency, 50, 43.
Tempalski, B., Flom, P. L., Friedman, S. R., Des Jarlais, D. C., Friedman, J. J., McKnight, C., et al. (2007). Social and political factors predicting the presence of
syringe exchange programs in 96 US metropolitan areas. American Journal of
Public Health, 97, 437.
Tortu, S., Neaigus, A., McMahon, J., & Hagen, D. (2001). Hepatitis C among noninjecting drug users: A report. Substance Use and Misuse, 36, 523–534.
Tortu, S., McMahon, J., Pouget, E., & Hamid, R. (2004). Sharing of noninjection druguse implements as a risk factor for hepatitis C. Substance Use and Misuse, 39,
211–224.
Valdez, A., Kaplan, C. D., & Curtis, R. L., Jr. (2007). Aggressive crime, alcohol and drug
use, and concentrated poverty in 24 US urban areas. The American Journal of Drug
and Alcohol Abuse, 33, 595–603.
Wallace, J. I., Porter, J., Weiner, A., & Steinberg, A. (1997). Oral sex, crack smoking,
and HIV infection among female sex workers who do not inject drugs. American
Journal of Public Health, 87, 470.
Watters, J., & Biernacki, P. (1989). Targeted sampling: Options for the study of hidden
populations. Social Problems, 36, 416–430.
Werb, D., Wood, E., Small, W., Strathdee, S., Li, K., Montaner, J., et al. (2008). Effects
of police confiscation of illicit drugs and syringes among injection drug users in
Vancouver. International Journal on Drug Policy, 19, 332–338.
Werb, D., DeBeck, K., Kerr, T., Li, K., Montaner, J., & Wood, E. (2010). Modelling crack
cocaine use trends over 10 years in a Canadian setting. Drug and Alcohol Review,
29, 271–277.
Wodak, A., & Cooney, A. (2006). Do needle syringe programs reduce HIV infection among injecting drug users: A comprehensive review of the international
evidence. Substance Use & Misuse, 41, 777–813.
�
 Mel Krajden
Mel Krajden