The American Journal of Pathology, Vol. 174, No. 6, June 2009
Copyright © American Society for Investigative Pathology
DOI: 10.2353/ajpath.2009.080941
Immunopathology and Infectious Diseases
Compartmentalization of Immune Responses in
Human Tuberculosis
Few CD8⫹ Effector T Cells but Elevated Levels of FoxP3⫹
Regulatory T Cells in the Granulomatous Lesions
Sayma Rahman,* Berhanu Gudetta,†
Joshua Fink,* Anna Granath,‡ Senait Ashenafi,*§
Abraham Aseffa,¶ Milliard Derbew,储
Mattias Svensson,* Jan Andersson,*,**
and Susanna Grundström Brighenti*
From the Center for Infectious Medicine,* and the Division of
Infectious Diseases,** Department of Medicine, the Ear, Nose and
Throat Clinic,‡ Department of Clinical Sciences, Intervention and
Technology (CLINTEC), Karolinska Institutet, Karolinska
University Hospital, Stockholm, Sweden; the Departments of
Paediatrics,† Pathology,§ and Surgery,㛳 Faculty of Medicine,
Addis Ababa University and Tikur Anbessa Hospital, Addis
Ababa, Ethiopia; and the Armauer Hansen Research Institute,¶
Addis Ababa, Ethiopa
Immune responses were assessed at the single-cell
level in lymph nodes from children with tuberculous
lymphadenitis. Tuberculosis infection was associated
with tissue remodeling of lymph nodes as well as
altered cellular composition. Granulomas were significantly enriched with CD68ⴙ macrophages expressing the M. tuberculosis complex-specific protein antigen MPT64 and inducible nitric oxide synthase.
There was a significant increase in CD8ⴙ cytolytic T
cells surrounding the granuloma; however, CD8ⴙ T
cells expressed low levels of the cytolytic and antimicrobial effector molecules perforin and granulysin in
the granulomatous lesions. Quantitative real-time
mRNA analysis revealed that interferon-␥ , tumor necrosis factor-␣ , and interleukin-17 were not up-regulated in infected lymph nodes, but there was a significant induction of both transforming growth factor-
and interleukin-13. In addition , granulomas contained an increased number of CD4ⴙFoxP3ⴙ T cells
co-expressing the immunoregulatory cytotoxic Tlymphocyte antigen-4 and glucocorticoid-induced tumor necrosis factor receptor molecules. Low numbers of CD8ⴙ T cells in the lesions correlated with
high levels of transforming growth factor- and
FoxP3ⴙ regulatory T cells, suggesting active immunosuppression at the local infection site. Compartmentalization and skewing of the immune response toward a regulatory phenotype may result in an
uncoordinated effector T-cell response that reduces
granule-mediated killing of M. tuberculosis-infected
cells and subsequent disease control. (Am J Pathol
2009, 174:2211–2224; DOI: 10.2353/ajpath.2009.080941)
Infection with Mycobacterium tuberculosis (Mtb) is a major
cause of morbidity and mortality in large parts of the
world and considered one of the most important global
health problems. Protective immunity to tuberculosis (TB)
in humans depends on both CD4⫹ and CD8⫹ T cells;
however cell-mediated immune responses rarely result in
complete eradication of infection. On antigen-specific T
cell activation, effector cytokines are produced that promote macrophage activation and control of Mtb growth,
partly through the production of reactive oxygen and
nitrogen intermediates, including nitric oxide (NO). However, Mtb-infected macrophages that fail to eradicate
the bacteria promote the generation of chronic inflammation and formation of granulomas.1 Mtb-infected
macrophages residing in the granuloma subsequently
recruit T cells to the area of infection, in an attempt to
organize and contain the infection.2,3 Despite vigorous
immune reactivity at the site of infection, Mtb has evolved
strategies to survive in the granulomas, resulting in infection that persists for extended periods of time. This may
Supported in part by grants from the Swedish Society for Medical Research, the Swedish Foundation for Strategic Research, Sida/SAREC, the
Swedish Research Council, the Swedish Heart and Lung Foundation and
the National Board of Health and Welfare.
Accepted for publication February 26, 2009.
Address reprint requests to Dr. Susanna Brighenti, Center for Infectious Medicine, F-59, Karolinska University Hospital Huddinge, 141 86
Stockholm, Sweden, E-mail: susanna.brighenti@ki.se.
2211
�2212
Rahman et al
AJP June 2009, Vol. 174, No. 6
be partly explained by the finding that the adaptive immune response to human TB is delayed compared with
most other infections or immunizations, allowing the initial
bacterial population to expand markedly in host macrophages that organizes the granulomatous response before induction of cell-mediated immunity.4
Rapid onset of a Th1 cytokine response, including
primarily interferon (IFN)-␥5 and tumor necrosis factor
(TNF)-␣,6 has been shown to be instrumental in the development of protective TB immunity. More recently it has
also been proposed that Th17 cells, which produce interleukin (IL)-17 and IL-23, may contribute to inflammation,7 induction of antimicrobial peptides and recruitment
of Th1 cytokine producing CD4⫹ T cells, resulting in
restricted Mtb growth in the lungs.8 Thus, induction and
kinetics of the Th17 response may be critical for the
triggering of Th1 cells and subsequent macrophage and
effector T cell activation at the primary site of TB infection.
In contrast to a Th1/Th17 response, a Th2 or anti-inflammatory cytokine profile characterized by production of
IL-4/IL-5/IL-139 or IL-10/transforming growth factor
(TGF)-10 respectively, has been associated with loss of
immune control and increased dissemination of Mtb.11
Delayed or inappropriate T cell activation, leading to
inadequate production of inflammatory cytokines, may
therefore result in the immunopathogenesis characteristic of clinical TB.
A Th1 cytokine response promotes the activation of
cytolytic T cells (CTLs) that express different cytolytic
effector molecules inside cytoplasmic granules. It has
been demonstrated that the granule-associated antimicrobial molecule granulysin can kill intracellular Mtb bacilli through osmotic lysis in cooperation with the cytolytic
protein perforin.12,13 Indeed, granulysin and perforin
have been shown to be co-expressed in human CD8⫹
CTLs after exposure to Mtb-infected macrophages, suggesting that these molecules constitute a multifunctional
unit of the T cell response with the capacity to attract and
kill TB-infected target cells.14 The coordinated expression of granulysin and IFN-␥ correlates with clinical improvement of TB disease,15,16 providing additional evidence that multiple effector functions are crucial in
protective immunity to TB. Therefore, a selective dysfunction in the expression of Th1 cells and subsequent CTL
function could alter the host’s ability to generate sterilizing TB immunity. Accumulation and activation of regulatory T (Treg) cells at the site of TB infection may prevent
the development of polyfunctional T cell responses.17
Natural or induced Treg cells are a heterogeneous population of CD4⫹ T cells and some Treg cell subsets
co-express activation markers such as CD25, cytotoxic
T-lymphocyte antigen-4 (CTLA-4) and glucocorticoid-induced tumor necrosis factor receptor (GITR), while the
most rigorous marker for these cells is the transcription
factor forkhead box p3 (FoxP3). Treg cells are known to
suppress excess immune activation and thus prevent the
development of immunopathology, including inhibition of
Mtb-induced production of IFN-␥ in CD4⫹ T cells18 –20
and the cytolytic function of CD8⫹ CTLs,21–24 which
could lead to chronic infection instead of pathogen
clearance.
In this report, we have examined if clinical TB infection
in treatment naïve children was associated with an inadequate Th1 response and low expression of cytolytic and
antimicrobial molecules. Spatial assessment including
tissue morphology, cellular composition and distribution
of inflammatory and immunosuppressive markers was
performed at the single-cell level in lymphoid tissue of
children with local TB-lymphadenitis. Moreover, compartmentalization of the CTL response was determined in the
local environment of the TB granuloma. Our aim was to
study potential alterations in the expression of cytokines
and cytolytic effector molecules in TB infected lymph
nodes and determine whether induction of Treg cells
could play a role in establishment of disease. Here, we
present the first evidence demonstrating a deficiency in
CD8⫹ T cells and cytolytic effector molecules, perforin
and granulysin, at the site of infection in human TB lesions. Reduced numbers of CTLs expressing low levels
of perforin and granulysin, correlated with an elevated
frequency of FoxP3⫹ Treg cells inside the granulomas.
These results suggest that an imbalance in the proportion
of effector T cells to Treg cells, present at the site of
infection, may contribute to establishment of TB infection.
Materials and Methods
Patients
A one year prospective study was performed and included 21 HIV-negative children, 3 to 10 years old, with a
regional or local lymphadenopathy suggestive of TB. This
included patients with a persistent (⬎3 to 8 weeks) enlargement of a non-tender, palpable lymph node in the
cervical or submandibular areas of the neck as determined by physical examination by an experienced clinician. Common clinical symptoms were fever, cough,
sweating, and anorexia. Lymph nodes in the neck region
were surgically removed from children with persistent
swelling of one or multiple lymph nodes. Chest X-ray was
normal (ie, no signs of pulmonary lesions) in all enrolled
study subjects, suggesting a local lymphadenopathy
without involvement of a pulmonary infection. Accordingly, cases of systemic or pulmonary infection were
excluded from the study as were children with previous or
ongoing treatment with anti-TB drugs. Children included
in the study were recruited at the Department of Pediatrics and Child Health, Tikur Anbessa Hospital, Addis
Ababa, Ethiopia, with parent’s or guardian’s approval
and signed informed consent. All children were previously vaccinated with Bacille Calmette Guerin (BCG) and
had an average body mass index of 14.3 (compared with
16 among Swedish age-matched controls). At surgery, a
lymph node biopsy and a blood sample (5 to 10 ml) was
obtained from the study subjects. Serum was used for
viral screening for HIV, cytomegalovirus, Epstein-Barr virus, rubella, and adenovirus by PCR. Stool and urine
samples showed no signs of an invasive parasitic disorder. Patients were divided into two groups; TB-positive(⫹) lymphadenitis (n ⫽ 11) and TB-negative(⫺) nonspecific lymphadenitis (n ⫽ 10) (Table 1). A definite TB
�Few CD8⫹ Effector T Cells in Human TB
2213
AJP June 2009, Vol. 174, No. 6
Table 1.
Clinical and Microbiological Demography of Children with a Local Lymphadenitis*
Patient No.
#1
#2
#3
#4
#5
#6
#7
#8
#9
#10
#11
#12
#13
#14
#15
#16
#17
#18
#19
#20
#21
Sex†
Age (years, months)
BMI‡
TB-culture§
Histology¶
PCR㛳
Antibiotic treatment**
M
M
F
F
F
F
F
F
F
M
F
F
F
F
F
M
F
M
M
M
M
3y
7y
4y
6y
9y
4y6m
6y6m
7y2m
3y7m
7y
4 y 11 m
10 y
8y
4y
3y2m
4y9m
4y8m
6y7m
9y3m
6 y 11 m
4y5m
16.5
14.3
15.4
12.7
13.7
15.8
11.5
12.7
16.3
13.2
15.3
12.8
14
16.9
14.2
14.8
14.3
15.4
13
13.1
14.7
pos (⫹)
pos (⫹)
pos (⫹)
pos (⫹)
pos (⫹)
pos (⫹)
pos (⫹)
pos (⫹)
pos (⫹)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
TB
TB
TB
TB
TB
TB
TB
TB
TB
TB
TB
not TB
not TB
not TB
not TB
not TB
not TB
not TB
not TB
not TB
not TB
Mtb
Mtb
Mtb
Mtb
Nd
Mtb
Mtb
Mtb
Mtb
Mtb
Mtb
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
neg (⫺)
cured
improved
nd
cured
cured
cured
cured
cured
cured
cured
cured
cured
improved
cured
cured
cured
improved
cured
improved
cured
cured
*All children were in the age of 3 to 10 years and had clinical symptoms of a local TB-lymphadenitis including chronic (⬎3 to 8 weeks) non-tender
swelling of lymph nodes in the neck region as well as a normal pulmonary X-ray. Biopsy and blood samples were collected from the children before
initiation of antibiotic treatment.
TB diagnosis was based on clinical symptoms, X-ray, TB culture, histology and PCR.
†
Sex; M ⫽ male; F ⫽ female.
‡
BMI ⫽ body mass index.
§
Tissue homogenate from biopsy were used for TB culture. TB positive culture ⫽ pos(⫹); TB negative culture ⫽ neg(⫺).
¶
Histopathological analysis of formalin-fixed lymph node biopsies was performed by a pathologist and determined as either a granulomatous
reaction consistent with tuberculosis (TB) or as a reactive follicular hyperplasia consistent with chronic non-specific lymphadenitis (not TB).
㛳
TB-specific PCR on DNA obtained from tissue biopsy. Mycobacterium tuberculosis ⫽ Mtb, not determined ⫽ nd, negative ⫽ neg(⫺).
**Patients #1 to #11 were treated with conventional anti-TB drugs: rifampicin, isoniazid, pyrazinamid and streptomycin, whereas patients #12 to #21
were treated with the broad-spectrum antibiotic amoxicillin. Not determined ⫽ nd.
diagnosis was based on a positive TB-culture of tissue
homogenate and/or histopathological evidence of a
granulomatous reaction as well as amplification of TBDNA by PCR. Lymph node biopsies obtained from the
children were divided into three parts; one for TBculture and PCR, one for histology, and one (snapfrozen and stored at ⫺85°C) for future immunological
analysis. TB-culture was performed using the established Løwenstein-Jensen methodology whereas typing was done on DNA extracts from heat killed isolates.
Tissue homogenate from lymph node biopsies were
decontaminated in 1% NaOH containing 3% SDS, and
neutralized in 0.1% sulfuric acid containing 0.0008%
bromocresol-purple. After centrifugation, tissue pellets
were resuspended in 1 ml of 7H9 media that were
inoculated in Løwenstein-Jensen tubes, one tube containing glycerol and another tube containing pyruvate.
The culture media were incubated at 37C° up to 8
weeks with weekly observation for growth. Isolates
were confirmed as Mtb using PCR-based deletion
analysis including specific primers for RD4, RD9, and
RD10 according to established procedures.25,26 H&E
staining was used for histopathological tissue analysis
of the lymph node samples performed by a specialized
pathologist at the Armauer Hansen Research Institute.
TB-pos(⫹) specimens (n ⫽ 11) revealed a granulomatous reaction with multinucleated giant cells, epithelioid cell clusters and tissue necrosis consistent with
TB (Table 1). The histology of TB-neg(⫺) lymph node
samples (n ⫽ 10) typically demonstrated a reactive
follicular hyperplasia characteristic of chronic nonspecific inflammation (Table 1). After surgery, children
with culture-confirmed TB were treated with standard
anti-TB drugs (rifampicin, isoniazid, pyrazinamide, and
streptomycin) whereas children with non-specific lymphadenitis were treated with broad-spectrum antibiotics
(amoxicillin), which normally cured their lymphadenitis
(Table 1).
Lymphoid tissue (tonsils) from age-matched children
(n ⫽ 10; M/F: 5/5; age: 3 to 10 years) undergoing tonsillectomy due to non-infectious tonsil hyperplasia were used as
controls for immunocytochemical staining. The uninfected
controls were recruited at the Karolinska University Hospital,
Huddinge, Sweden. Ethical permission for this study was
obtained in both Ethiopia and Sweden and children were
only recruited into the study after parent’s or guardian’s approval and signed informed consent.
Immunohistochemistry and Confocal Analysis of
Frozen Tissue Sections
Cryopreserved lymphoid tissue biopsies were embedded in OCT-compound (Tissue-TEK, Sakura) and cut into
8 m thick sections, mounted on HTC microscope slides
(Histolabs, Gothenburg, Sweden) and fixed in 4% formaldehyde (Sigma, Stockholm, Sweden) for 15 minutes.
Immunohistochemistry was performed according to the
ABC-method as previously described.27 Positive staining
was developed using a diaminobenzidine substrate
�2214
Rahman et al
AJP June 2009, Vol. 174, No. 6
(Vector Laboratories, Burlingame, CA) while hematoxylin
was used for nuclear counterstaining. We used acquired
computerized image analysis to quantify immunohistochemical staining in situ by transferring digital images of
the stained tissue samples from a DMR-X microscope to
a computerized Quantimet 5501W image analyzer (Leica
Microsystems, Germany).28 Positive immunostaining was
quantified at the single-cell level in 10 to 50 high-power
fields using a Qwin 550 software program (Leica Imaging
Systems, Germany).29 Protein expression was determined as the percent positive area of the total relevant
cell area (fibrotic and necrotic tissue areas were excluded) where the total cell area was defined as the
nucleated and cytoplasmic area within the tissue biopsy.
The complete tissue section scanned had a mean size of
4.5 ⫻ 106 m2. Immunohistochemistry slides were coded
and each staining was assessed independently by two
individuals in a blinded fashion, generally resulting in
⬍10% intra-assay variation. For image analysis of TBpos(⫹) lymph nodes, positive immunostaining determined from total tissue sections was compared with image analysis of the granulomatous lesions (granulomas)
only. Here the same tissue section was assessed twice;
once for immunohistochemical analysis of total lymph
node tissue and once again for analysis including tuberculous granulomas only. Differentiation between total and
granulomatous tissue was performed using the tissue
excluder function of the soft ware. Specific granulomas
were counted and individually assessed using the in situ
soft ware and visual identification of granulomas. On
average, TB-pos(⫹) lymph node sections contained 10 to
20 granulomas with a mean size of 2 ⫻ 106 m2 included
in the image analysis. Tissue sections stained with secondary antibodies only were used as negative controls.
The specificity of the primary antibodies used had previously been tested, particularly in human lymphoid tissue.27,29 –32 Two-color staining was performed using
indirect immunofluorescence and analysis performed
using a filter-free spectral confocal microscope (Leica
TCS SP2 AOBS).
Antibodies
Primary antibodies were CD3, CD4, and CD8 (BD),
elastase/neutrophil, CD56, CD68, MAC387, CD45RA,
CD45RO, CD20, polyclonal Mycobacterium bovis (pAbBCG) (Dako, Glostrup, Denmark), collagen type I (Abcam, Cambridge, UK), iNOS (BD/Transduction Laboratories, San Jose, CA) and nitrotyrosine (n-tyr) (Upstate,
Lake Placid, NY), DC-SIGN, granzyme A (clone CB9),
CTLA-4 (BD/Pharmingen, San Diego, CA), perforin (clone
p16-17) (Mabtech, Stockholm, Sweden), GITR (R&D systems, Abingdon, UK), FoxP3 (Novus Biologicals, Littleton,
CO), and TGF- (Santa Cruz Biotechnology Inc., Santa
Cruz, CA) Affinity purified human granulysin was kindly
provided by Dr. Alan Krensky and Dr. Carol Clayberger,
Stanford University, CA. An affinity purified rabbit polyclonal antibody directed against the secreted Mtb-protein MPT64 was helpfully provided by Prof. Harald Wiker
and Prof. Lisbet Svinland, Bergen University, Norway.
iNOS was used as an indirect marker for NO production
whereas NO metabolism was detected using n-tyr. FoxP3
and co-expression of CTLA-4 and GITR were used as
markers to detect Treg cells. MPT64 detects an Mtbspecific antigen33 while the use of cross-reactive pAbBCG for detection of Mtb-antigens in Ziehl-Neelsen negative tissue samples has recently been described.34
CD1a (Dako, Glostrup, Denmark) and DC-SIGN (BD/
Pharmingen, San Diego, CA) were used to distinguish the
dendritic cell population from CD4⫹ T cells in the lymph
nodes. Furthermore, double-staining with CD4 and CD3,
revealed that most CD4⫹ cells in the lymph node were T
cells.
Biotinylated secondary antibodies, goat anti-mouse
IgG, rabbit anti-goat IgG and swine anti-rabbit F(ab⬘)2,
were purchased from Dako. For dual staining, tissues
were stained with rat anti-human CD8 or CD4 (Serotec,
Oxford, UK) and mouse anti-human CD68, granzyme A,
perforin, FoxP3, GITR, and CTLA-4, as well as rabbit
anti-human granulysin and rabbit polyclonal MPT64 followed by the appropriate Alexa Fluor-conjugated secondary Ab (Molecular Probes, Eugene, Oregon).
mRNA Extraction and Real-Time PCR of Frozen
Sections from Human Lymphoid Tissue
RNA was extracted from frozen tissue sections (2 ⫻ 50
m) using the Ambion RiboPure extraction kit according
to the manufacturers instructions. RNA was reverse transcribed using superscript reverse transcriptase (Invitrogen, Carlsbad, CA) and random hexanucleotide primers
(Roche, Mannheim, Germany). Amplification of ubiquitin
C, CD4, IFN-␥, TNF-␣, IL-17A, CD8, granzyme A, perforin, granulysin, FoxP3, TGF-, IL-10, and IL-13 cDNA
was performed using the ABI PRISM 7700 sequence
detection system and commercial FAM dye-labeled TaqMan MGB probes and primers (Applied Biosystems, Foster City, CA). Ubiquitin C was tested together with a panel
of commonly used house-keeping genes and was selected as our calibrator as the expression was shown to
be constitutive and stable in both test and control samples. Hence, Ct values for the different mRNAs were
normalized to ubiquitin C and relative expression was
determined using the Livak method.35 The Ct values obtained for TB-pos(⫹) and TB-neg(⫺) lymphadenitis were
compared with that of control tonsil tissue and data are
presented as fold change of mRNA in the infected groups
compared to controls.
Statistical Analysis
Due to the small sample size in each group (n ⫽ 10 to
11), the data are mostly presented as median ⫾ interquartile range (IQR). Values from 2 individual experiments are shown. Non-parametric analyses used to calculate indicated P values, included a Mann Whitney test
(when comparing two unmatched samples), a Wilcoxon
signed rank test (when comparing two matched samples)
or a Kruskal-Wallis test (when comparing more than two
groups). A P value ⬍0.001 was considered extremely
�Few CD8⫹ Effector T Cells in Human TB
2215
AJP June 2009, Vol. 174, No. 6
significant (***), a P value between 0.001 and 0.01 was
considered very significant (**), a P value between 0.01
and 0.05 was considered significant (*) whereas a P
value ⬎0.05 was considered not significant (ns). Statistical analyses were performed in GraphPad Prism-4.
inflammation ie, non-specific lymphadenitis. This group was
dominated by cases of lymphadenitis caused by bacteria or
possibly parasites, since all biopsy samples were negative
for a panel of viral pathogens that are most commonly
associated with pediatric lymphadenopathy (HIV, cytomegalovirus, Epstein-Barr virus, rubella, and adenovirus). Lymphadenopathy among TB-neg⫺) children was
cured or improved after treatment with the broad-spectrum
antibiotic, amoxicillin. Immunological analysis was performed on frozen lymph nodes biopsies obtained from TBpos(⫹) and TB-neg(⫺) lymphadenitis cases before treatment, as well as from one group of age-matched Swedish
control children with tonsil hyperplasia.
Microscopic analysis revealed that follicular and parafollicular areas of the TB-pos(⫹) tissue were disturbed by the
expansion of confluent granulomas, whereas normal lymphoid structure and cellular architecture was maintained in
the TB-neg(⫺) and control tonsil group (Figure 1A). Despite
extensive tissue remodeling associated with TB infection,
the presence of CD3⫹ T cells was easily detected within the
tissue (Figure 1A). Furthermore, granulomatous lesions in
Results
TB Infection is Associated with Extensive Tissue
Remodeling and Altered Cellular Composition in
Infected Lymph Nodes
All patients (age 3 to 10 years) included in this study had
clinical symptoms of a local subacute TB-lymphadenitis.
Based on TB diagnosis, the patients were divided into two
groups: TB-positive(⫹) and TB-negative(⫺) cases (Table
1). TB-pos(⫹) children had culture and/or histology/PCR
proven TB and responded to treatment with conventional
anti-TB drugs. In contrast, TB-neg(⫺) patients were considered to suffer from a reactive non-specific lymph node
A
TB-pos(+) lymphadenitis
TB-neg(-) lymphadenitis
Uninfected control tonsil
GC
CD3
GC
125 µm
TB-pos(+) lymphadenitis
Uninfected control tonsil
C
TB
-p
% Cellularity of lymphoid tissue
os
(+
)l
ym
ph
TB
ad
-n
en
eg
it i
(-)
s
ly
m
ph
U
ni
ad
nf
en
ec
iti
te
s
d
co
nt
ro
lt
on
si
l
B
CD68
90
***
70
GC
50
E
***
***
**
***
**
D
20
-S
IG
N
C
D
68
M
AC
38
7
M
PT
64
C
GC
30
25
20
15
10
5
0
C
D
D
GC
GC
% positive area of total cell area
50
40
*
30
*
20
Collagen type I
10
O
A
R
D
45
D
C
C
45
R
8
4
D
D
C
C
D
3
0
C
CD8
CD4
30
TB-pos(+) lymphadenitis
TB-neg(-) lymphadenitis
50 µm
Uninfected control tonsil
Figure 1. Induction of tissue remodeling and
altered cellular composition in TB-infected
lymph nodes. A: The images demonstrate tissue
morphology and CD3 immunohistological staining in TB-pos(⫹) and TB-neg(⫺) lymph nodes
as well as uninfected control tonsil. Magnification ⫽ original ⫻50. B: Expression and distribution of CD68, CD8 and collagen type I in TBpos(⫹) lymph nodes compared with uninfected
control tonsil. Granulomatous lesions in TBpos(⫹) lymphadenitis are marked with a solid
line. Magnification ⫽ original ⫻125. GC indicates germinal centers or follicles in lymphoid
tissue. Staining was performed using immunohistochemistry and positive cells are shown in
brown (diaminobenzidine) whereas negative
cells are counterstained blue with hematoxylin.
C: Mean cellularity (⫾SD) of TB-pos(⫹) and
TB-neg(⫺) lymphadenitis compared with uninfected control, respectively, was estimated in the
analysis. Data are presented as % cellularity of
lymphoid tissue, in a box and whisker plot. D:
In situ computerized image analysis was used to
assess median expression (⫾IQR) of the indicated APC markers and Mtb-specific antigen
MPT64 or (E) T cell markers in TB-pos(⫹) compared with TB-neg(⫺) lymphadenitis as well as
uninfected control tonsils. Data are presented as
% positive area of the total cell area. Statistical
significance of differences in tissue cellularity
and protein expression was determined by a
non-parametric Kruskal-Wallis test, TB-pos(⫹)
lymphadenitis versus TB-neg(⫺) lymphadenitis
versus uninfected control. The statistical significance of the indicated P values was determined
as: *P ⬍ 0.05, **P ⬍ 0.01, ***P ⬍ 0.001 and P ⬎
0.05 ns (not significant).
�2216
Rahman et al
AJP June 2009, Vol. 174, No. 6
TB-pos(⫹) lymph nodes were enriched with CD68⫹ macrophages and CD4⫹ T cells, while CD8⫹ T cells were
predominantly located in the T cell rich peri-granulomatous
areas (Figure 1B). Granulomatous inflammation induced by
Mtb was also associated with tissue fibrosis involving widespread collagen deposition (TB-pos(⫹): 20.8%; Control tonsil: 2.5%) (Figure 1B).
To determine whether TB infection involved altered
cellular composition of lymph node tissue, in situ image
analysis was performed at the single cell level. As illustrated in Figure 1C, the median cellularity of TB-pos(⫹)
lymph node tissue was significantly lower (P ⬍ 0.001)
compared with TB-neg(⫺) lymphadenitis and control tonsil tissue (Figure 1C). The reduction in cellularity was
primarily due to a decreased proportion of CD20⫹ B cells
in TB infected lymph nodes (Figure 1D). In contrast, we
observed increased frequencies of DC-SIGN⫹ dendritic
cells, CD68⫹ macrophages and MAC387⫹ monocytes
and neutrophils in TB-pos(⫹) lymph nodes compared
with both TB-neg(⫺) (P ⬍ 0.05) and control (P ⬍ 0.001)
tissue (Figure 1D). Expression of mycobacterial protein
antigens in lymphoid tissue including cross-reactive
M.bovis (data not shown) and the Mtb-specific MPT64
protein, was highly significant (P ⬍ 0.001) in TB-pos(⫹)
cases (Figure 1D). No TB antigen was evident in the other
groups. Importantly, the proportion of CD3⫹ and CD4⫹ T
cells was unaltered in TB-pos(⫹) compared with uninfected control tissue whereas the proportion of CD8⫹ T
cells was increased (P ⬍ 0.05) (Figure 1E). TB-pos(⫹)
lymph nodes also had a significantly (P ⬍ 0.05) higher
number of memory CD45RO⫹ T cells compared with
control samples, while the number of naïve CD45RA⫹ T
cells was similar in the three groups compared (Figure
1E). Thus, lymph node TB was associated with extensive
tissue remodeling and altered cellular composition involving reduced B cell numbers but increased proportions of macrophages, dendritic cells and relatively stable T cell numbers. These observations encouraged us to
perform a more detailed spatial analysis of the T cell
response associated with persistent TB-lymphadenitis.
Weak Induction of Inflammatory Cytokines and
Cytolytic Effector Molecules in TB Infected
Lymph Nodes
Quantitative real-time PCR analysis was performed to
investigate the cytokine profile and expression of T cellassociated cytolytic effector molecules in TB infected
lymph nodes. Relative change in mRNA extracted from
lymphadenitis cases were compared with uninfected
control tonsil. Consistent with in situ protein analysis,
mRNA levels of CD4 remained unchanged while CD8
mRNA was significantly up-regulated in TB-pos(⫹) and
TB-neg(⫺) lymphadenitis cases compared with control
tonsil tissue (Figure 2A). Interestingly, induction of the
important anti-TB cytokines IFN-␥ and TNF-␣ was poor
and IL-17 was significantly lower in TB-pos(⫹) lymphadenitis cases compared with controls (Figure 2A). Moreover, whereas mRNA expression of the granule-associated effector molecule granzyme A was significantly
increased, both perforin and granulysin remained low in
TB-pos(⫹) lymphadenitis (Figure 2A). In contrast, all cytolytic effector molecules were significantly higher in TBneg(⫺) lymphadenitis (Figure 2A).
Next, we aimed to determine tissue expression of cytolytic and antimicrobial effector molecules at the protein
level. Since in situ assessment of IFN-␥, TNF-␣, and IL-17
protein in lymphoid tissue resulted in too few positive
cells (⬍0.5%) to perform computerized image analysis,
we focused on protein analysis of granzyme A, perforin,
granulysin, and iNOS. Quantitative in situ image analysis
revealed a significant increase in granzyme A (P ⬍
0.001) and perforin (P ⬍ 0.01) but not granulysin in
TB-pos(⫹) lymph nodes compared with control tonsils
(Figure 2B). These T cell-associated effector molecules
were also up-regulated in TB-neg(⫺) lymphadenitis (grzA:
P ⬍ 0.05; pfn: P ⬍ 0.01; grs: P ⬍ 0.01) compared with
uninfected controls (Figure 2B). In contrast, induction of
iNOS (P ⬍ 0.001) was evident only in TB-pos(⫹) lymphadenitis (Figure 2B). Despite a significant increase in
perforin protein expression in TB-pos(⫹) lymph nodes,
the ratio of perforin- and granulysin expressing cells to
total CD8⫹ T cells remained low at both protein and
mRNA level (data not shown). In contrast, granzyme A
expression was significantly increased in the CD8⫹ T
cells (mRNA: P ⬍ 0.04, protein: P ⬍ 0.05), providing
evidence of T cell activation since this molecule is not
expressed in naïve T cells. The ratio of granzyme A, perforin
and granulysin expressing cells to total CD8⫹ T cells was
low in both TB-neg(⫺) lymphadenitis and in controls.
Microscopic analysis of TB-pos(⫹) lymph nodes revealed that the macrophage-associated effector molecule
iNOS was primarily produced inside the granulomas,
whereas granzyme A was expressed in granulomatous as
well as non-granulomatous areas (Figure 2C). Instead, perforin and granulysin were strictly expressed in the nongranulomatous areas outside the TB lesions (Figure 2C).
Confocal microscopy revealed that co-expression of granzyme A, perforin and granulysin was evident in CD8⫹ T
cells primarily located in the parafollicular areas of TBpos(⫹) lymph node tissue (Figure 2D). While perforin and
granulysin expression was restricted to CD8⫹ T cells, double-staining showed that expression of granzyme A was
also evident in a limited number of CD4⫹ T cells (below 15%
of all positive cells). Together, these findings suggests that
the spatial organization of the cytolytic T cell response in
TB-pos(⫹) lymph nodes are suboptimal.
Low Levels of CD8⫹ T cells and T cellassociated Cytolytic Effector Molecules in
MPT64-positive Lymph Node Granulomas
To determine in more detail the tissue distribution of T
cell-associated cytolytic effector molecules within TBpos(⫹) lymph nodes, we performed comprehensive microscopic analyses as outlined in Figure 3A. Expression of the
MPT64 protein, which is a 26-kDa secreted Mtb-specific
protein, was strictly localized to the granulomatous lesions
within infected lymph nodes (Figure 3A). To study functional
immune responses in close proximity to infected cells, in situ
�Few CD8⫹ Effector T Cells in Human TB 2217
AJP June 2009, Vol. 174, No. 6
A
TNF-α
IFN-γγ
IL-17
TB
-p
Fold change of mRNA Fold change of mRNA
os
(+
)l
ym
TB
ph
-n
ad
eg
en
(-)
iti
s
l
y
U
m
ni
ph
nf
ad
ec
e
te
ni
d
tis
co
nt
ro
lt
on
si
l
TB
-p
os
(+
)l
ym
TB
ph
-n
ad
eg
en
(-)
it i
s
l
y
U
m
ni
p
ha
nf
ec
de
te
ni
d
tis
co
nt
ro
lt
on
si
l
TB
-p
os
(+
)l
ym
TB
ph
-n
ad
eg
en
(-)
it i
s
l
y
U
m
ni
p
ha
nf
ec
de
te
ni
d
tis
co
nt
ro
lt
on
si
TB
l
-p
os
(+
)l
ym
TB
ph
-n
ad
eg
en
(-)
it i
s
l
ym
U
ni
ph
nf
ad
ec
en
te
d
iti
s
co
nt
ro
lt
on
si
l
CD4
10
10000
1
1
100
1
0.1
1
0.1
0.01
0.01
0.01
0.01
0.001
CD8
100
10
*
10
*
*
100
Perforin
100
1
1
1
0.1
0.1
8
**
Uninfected control tonsil
D
CD8-granzyme A
granzyme A
***
10
Granulysin
10
0.1
TB-pos(+) lymphadenitis
**
*
**
10
1
C
**
0.1
0.1
B
6 ***
4
Granzyme A
100
***
S
O
iN
TB-pos(+) lymphadenitis
TB-neg(-) lymphadenitis
CD8-perforin
perforin
n
Pf
G
rs
2
0
G
rz
A
% positive area of total cell area
10
10
iNOS
granulysin
Uninfected control tonsil
CD8-granulysin
GC
150 µm
Figure 2. Activated T cells produce suboptimal
levels of inflammatory cytokines and cytolytic
effector molecules in TB infected lymph nodes.
A: Cytokine profile and expression of T cellassociated cytolytic effector molecules in lymphoid tissue was determined using quantitative
real-time PCR. Fold change of CD4 mRNA and
pro-inflammatory cytokines IFN-␥, TNF-␣, and
IL-17, as well as CD8 mRNA and cytolytic effector molecules granzyme A, perforin, granulysin
to ubiquitin C mRNA in TB-pos(⫹) lymph nodes
was compared with that of TB-neg(⫺) lymph
nodes and uninfected control tissue. Data are
presented as fold change of mRNA in a box and
whisker plot and the dotted line represents a
relative difference of 1. B: In situ computerized
image analysis was used to assess median expression (⫾IQR) of cytolytic and antimicrobial
effector molecules in TB-pos(⫹) compared with
TB-neg(⫺) lymphadenitis as well as uninfected
control tonsils. Data are presented as % positive
area of the total cell area. C: The expression and
distribution of granzyme A, perforin, granulysin
and iNOS in TB-pos(⫹) lymph nodes was compared with uninfected control tonsil. Staining
was performed using immunohistochemistry
and arrows indicate positive (brown staining)
cells whereas negatively stained cells are counterstained with hematoxylin. Granulomatous lesions in TB-pos(⫹) lymphadenitis are marked
with a solid line. GC indicates germinal centers
or follicles in the tonsil tissue. Magnification ⫽
original ⫻125. D: Immunofluorescent staining
and confocal microscopy showed local distribution and co-expression of CD8⫹ T cells (red;
Alexa-594), granzyme A, perforin and granulysin (green; Alexa-488) in the parafollicular area
of a TB-pos(⫹) lymph node. Arrows indicate
double-positive cells in yellow. Magnification ⫽
original ⫻300. Statistical significance of differences in mRNA and protein expression was determined by a non-parametric Kruskal-Wallis
test (TB-pos(⫹) lymphadenitis versus TBneg(⫺) lymphadenitis versus uninfected control). The statistical significance of the indicated P values was determined as: *P ⬍ 0.05,
**P ⬍ 0.01, ***P ⬍ 0.001 and P ⬎ 0.05 ns (not
significant).
50 µm
image analysis was performed on the granulomatous lesions and compared with total lymph node tissue (Figure
3A). Assessment of cellularity in lymph node granulomas
revealed that the median cell density was 50%, which was
similar to total lymph node tissue (data not shown). The
morphology of granulomas found in the lymph node biopsies, varied from smaller cellular clusters to large granulomas containing a necrotic core. Statistically significant differences in tissue expression of different markers were
generally representative for all granulomas in a patient and
also comparing different patients within a group. Granulomatous lesions were associated with a higher proportion of
CD68⫹ macrophages (P ⫽ 0.001) expressing functional
iNOS (P ⫽ 0.002) as determined by the expression of the
NO metabolite nitro-tyrosine (P ⫽ 0.002) (Figure 3B). In
addition, granulomatous lesions expressed significantly
higher levels of M. bovis-specific protein antigens (P ⫽
0.001) as well as the Mtb-specific antigen MPT64 (P ⫽
0.008) (Figure 3B), which co-localized to CD68⫹ macrophages (Figure 3C). In contrast, MPT64 and CD8 showed
no evidence for overlapping or proximate expression (Figure 3C), suggesting that Mtb-antigen expressing cells and
CD8⫹ T cells were segregated from one another in the
tissue. As a consequence, profoundly reduced numbers
(P ⫽ 0.001) of CD8⫹ and CD56⫹ T and NK cells expressing the cytolytic effector molecules, perforin and granulysin,
was found in granulomatous lesions compared with total
lymph node tissue (Figure 3D). Interestingly, granzyme A
was maintained at comparable levels at both sites (Figure
3D). As a result, the ratio of granzyme A to total CD3⫹ T
cells was significantly increased in both total lymph node
tissue (P ⬍ 0.01) and granulomatous lesions (P ⬍ 0.001)
compared with TB-neg(⫺) lymphadenitis (data not shown)
and uninfected control tonsil (Figure 3E). However, the ratio
of perforin- and granulysin-expressing cells to total CD3⫹ T
cells was unaltered in granulomas compared with uninfected controls, indicating that these effector molecules
were specifically down-regulated inside the granuloma (Figure 3E). Accordingly, immunofluorescence and confocal
microscopy analysis revealed co-expression of perforin and
�2218
Rahman et al
AJP June 2009, Vol. 174, No. 6
B
Granulomatous
lesions
Total lymph
node tissue
Figure 3. Expression and distribution of APCs,
mycobacterial antigens, T cells and cytolytic effector molecules in total TB-pos(⫹) lymph node
tissue compared with granulomatous lesions. A:
The Mtb-specific protein antigen, MPT64, was
predominantly expressed inside tuberculous
granulomas. An excluder function of the image
analysis software program was used to determine protein expression in total TB-pos(⫹)
lymph node tissue compared with the granulomatous lesions (solid line). B: In situ computerized image analysis was used to assess median
expression (⫾IQR) of CD68⫹ macrophages,
iNOS, and n-tyr, and mycobacterial antigens,
BCG and MPT64, in total lymph node tissue as
compared with protein expression in the granulomatous lesions. C: Confocal images reveal
double-staining of CD68 or CD8 (red; Alexa
594) with Mtb-antigen MPT64 (green; Alexa488). Arrows indicate double-positive cells in
yellow and single-positive cells in red and
green. Magnification ⫽ original ⫻200. D: In situ
imaging was used to determine median expression (⫾ IQR) of CD8⫹ and CD56⫹ T and NK
cells, granzyme A, perforin and granulysin in
total lymph node tissue compared with protein
expression in the granulomatous lesions. The
data are presented as % positive area of total cell
area. E: Computerized image analysis was used
to determine the relative expression of effectors
and total CD3⫹ T cells in lymphoid tissue. The
ratios of granzyme A (grzA), perforin (pfn) and
granulysin (grs) expression to total CD3⫹ T cell
expression in total TB-pos(⫹) lymph node tissue compared with granulomatous lesions and
uninfected control are presented. The median
values of paired expression of effectors and
CD3⫹ T cells from all individual patients are
shown. F: Confocal microscopy illustrate distribution and co-expression of perforin (green;
Alexa-488) and granulysin (red; Alexa-594) in
the granulomatous lesions and T cell rich areas
of a TB-pos(⫹) lymph node. Arrows indicate
single-positive cells inside the granuloma but
also double-positive cells in yellow outside the
granuloma. Note the granular and polarized coexpression of the cytolytic effector molecules in
cells located outside the lesion. Magnification ⫽
original ⫻200 and ⫻600. Statistical significance
of differences in protein expression was determined by a non-parametric Wilcoxon signed
rank test (total TB-pos(⫹) lymph node tissue
versus granulomatous lesions). The statistical
significance of the indicated P values was determined as: **P ⬍ 0.01, ***P ⬍ 0.001 and P ⬎ 0.05
ns (not significant).
**
30
***
20
**
***
10
S
nty
M r
.b
ov
i
M s
PT
64
O
68
0
D
50 µm
**
40
iN
MPT64 antigen
% positive area of total cell area
TB-pos(+) lymphadenitis
C
A
Total lymph node tissue
Granulomatous lesion
C
CD8-MPT64
CD68-MPT64
Granuloma
Effector cell to CD3 cell ratio
E
***
10
8
6
4
*** ***
***
Pf
n
G
rs
G
rz
A
56
D
C
D
8
2
0
C
% positive area of total cell area
D
0,1
0,08
0,06
0,04
0,02
0
3
3
D3
C D / CD s / C
n
A/
r
rz
G
Pf
G
Total lymph node tissue
TB-pos(+) lymphadenitis
(total lymph node tissue)
Granulomatous lesion
TB-pos(+) lymphadenitis
(granulomatous lesions)
Uninfected control tonsil
Area outside granuloma
Granuloma
Perforin-granulysin
F
50 µm
50 µm
granulysin primarily in non-granulomatous areas outside
Mtb granulomas while mainly a few single-expressing cells
were present in the granulomatous lesions (Figure 3F).
Therefore, the CTL deficiency in the lesions was characterized by reduced numbers of CD8⫹ and CD56⫹ cells and a
low expression of perforin and granulysin (Figure 3D) including little co-expression of these cytolytic effectors in
CTLs (Figure 3F). Instead the granuloma was enriched with
CD68⫹ macrophages expressing the Mtb-protein antigen
MPT64 (Figure 3C). Collectively, these results demonstrate
a selective down-modulation of CTLs at the site of infection
10 µm
in the granulomas as compared with CTLs present in nongranulomatous areas.
Low CD8⫹ T cell Numbers Correlate with an
Increased Expression of FoxP3 and TGF- in
MPT64-Positive Lymph Node Granulomas
Our results indicated that CTL-mediated anti-microbial
activity was mainly associated to the parafollicular area of
TB-pos(⫹) lymphnodes, whereas the granulomatous le-
�Few CD8⫹ Effector T Cells in Human TB
2219
AJP June 2009, Vol. 174, No. 6
Figure 4. Expression and distribution of FoxP3
and TGF- in total TB-pos(⫹) lymph node tissue compared with granulomatous lesions. A:
Expression of immunoregulatory molecules and
anti-inflammatory as well as Th2 cytokines in
lymphoid tissue was determined using quantitative real-time PCR. Fold change of FoxP3 mRNA
and cytokines TGF-, IL-10, IL-13 to ubiquitin C
mRNA in TB-pos(⫹) lymph nodes was compared with that of TB-neg(⫺) lymph nodes and
uninfected control tissue. Data are presented as
fold change of mRNA in a box and whisker plot
and the dotted line represents a relative difference of 1. B: Immunohistochemical analysis of
MTP64, CD8, FoxP3, and TGF- expression in a
TB-pos(⫹) lymph node; both granulomatous lesion (solid line) and non-granulomatous areas
outside the granuloma are shown. Arrows indicate positive (brown staining) cells whereas
negatively stained cells are counterstained with
hematoxylin. Magnification ⫽ original ⫻125. C:
Confocal analysis of Treg cell expression in a
granuloma. Upper panel shows co-expression
of CD4 (red; Alexa-594) and FoxP3 (green; Alexa-488) at a high (⫻125) and low (⫻600) magnification. Note the nuclear staining pattern of
FoxP3, whereas CD4 is located at the surface of
positive cells. Lower panel shows co-expression
of CTLA-4 (red; Alexa-594) and GITR (green;
Alexa-488) as well as CD4 (red; Alexa-594) and
CTLA-4 (green; Alexa-488) inside a granuloma.
Arrows indicate double-positive cells. Magnification ⫽ original ⫻200 and ⫻600. (D) Computerized image analysis was used to determine the
median expression (⫾IQR) of CD4⫹ T cells,
FoxP3 Treg cells, CTLA-4, GITR, and TGF- in
total lymph node tissue compared with protein
expression in the granulomatous lesions. The
data are presented as % positive area of total cell
area. E: Computerized image analysis was used
to determine the relative expression of CD8⫹ T
cells and FoxP3⫹ Treg cells in lymphoid tissue.
The ratios of total CD8⫹ T cells to total FoxP3⫹
Treg cells expressed in total TB-pos(⫹) lymph
node tissue compared with granulomatous lesions
as well as TB-neg(⫺) lymphadenitis and uninfected control are presented. The median values of
paired expression of CD8⫹ T cells and FoxP3⫹
Treg cells from all individual patients are shown.
*P ⬍ 0.05, **P ⬍ 0.01 and ***P ⬍ 0.001.
sions contained few CTLs producing low levels of cytolytic effector molecules. Therefore we investigated
whether an enrichment of Treg cells at the site of infection
in the granuloma, could help to explain the failure to
induce CTLs producing perforin and granulysin. Quantitative real-time PCR analysis revealed that mRNA for
FoxP3 as well as TGF- and IL-13, was significantly upregulated in the TB infected tissue, whereas there was no
change in mRNA expression of IL-10 (Figure 4A) and IL-4
(data not shown). In situ imaging demonstrated that opposed to CD8⫹ T cells, the numbers of FoxP3⫹ and
TGF-⫹ cells were increased at the site of infection in the
granuloma (Figure 4B). Hence, the expression of CD8⫹ T
cells was inversely correlated to FoxP3⫹ Treg cells. Furthermore, two-color staining and confocal microscopy
confirmed that FoxP3⫹ cells mainly belonged to the
CD4⫹ T cell subset located in the granulomas (Figure
4C). Additionally, there was an enrichment of CTLA-4 and
GITR double-positive cells inside the granuloma compared with the surroundings areas and CTLA-4 was
mainly expressed on CD4⫹ T cells (Figure 4C).
In situ image analysis confirmed that granulomatous
lesions contained similar numbers of CD4⫹ T cells and
significantly higher levels of FoxP3⫹ Treg cells (P ⫽
0.002) compared with total lymph node tissue (Figure
4D). Expression of CD45RA was significantly reduced
(P ⫽ 0.001) whereas CD45RO expression was unchanged in granulomas compared with total lymph node
tissue, suggesting that there were few naïve T cells in the
lesions (data not shown). CTLA-4 and GITR were also
expressed at significantly higher levels (P ⫽ 0.001; P ⫽
0.007) at the site of infection in the granuloma (Figure
4D). Furthermore, TGF- was expressed at a fivefold
higher level in the granulomas and was significantly (P ⫽
0.008) up-regulated as compared with total lymph node
tissue (Figure 4D). In accordance with the mRNA analysis, TGF- levels in TB-pos(⫹) lymph nodes (5,62%) were
significantly higher (P ⬍ 0.001) compared with TBneg(⫺) lymphadenitis (1,95%) and uninfected controls
(0,09%). Interestingly, the ratio of CD8⫹ T cells to
FoxP3⫹ Treg cells was significantly (P ⫽ 0.003) lower in
granulomatous lesions compared with total lymph node
�2220
Rahman et al
AJP June 2009, Vol. 174, No. 6
tissue, TB-neg(⫺) lymphadenitis and uninfected controls
(Figure 4E). In addition, the mRNA and protein ratio of
IFN-␥/FoxP3 and IL-17/FoxP3 was significantly lower in
TB-pos(⫹) lymphadenitis compared with uninfected controls (data not shown). Together, these results demonstrate
an imbalance in the proportion of effector T cells to Treg
cells present at the site of infection in TB-lymphadenitis.
Discussion
The immunological mechanisms involved in the pathogenesis of human TB are poorly understood. In this study,
we explored immune cell effector functions at the site of
infection in treatment naïve children with a recent diagnosis of local TB-lymphadenitis. We demonstrated that
TB infection was accompanied by considerable remodeling of lymphoid tissue, including granuloma formation
and enhanced deposition of collagen type I. Despite this
tissue remodeling, the level of CD4⫹ and CD8⫹ T cells
remained stable whereas the B cell compartment was
significantly reduced. In addition, our results suggest a
weak induction of pro-inflammatory cytokines IFN-␥,
TNF-␣, and IL-17, as well as cytolytic granule-associated
effector molecules, perforin and granulysin, in TB infected lymph node tissue. Interestingly, there was a compartmentalization of the immune response resulting in
surprisingly low numbers of CD8⫹ T cells expressing low
levels of perforin and granulysin in the granulomatous
lesions that were enriched in macrophages expressing
iNOS and the Mtb-specific protein antigen MPT64. Besides, CD8⫹ T cells present in the TB lesions had little
co-expression of cytolytic effector molecules. A weak
induction of inflammatory cytokines and important anti-TB
effector molecules correlated with up-regulated numbers
of FoxP3⫹ Treg cells and elevated expression of TGF-
and IL-13, in patients with persistent TB-lymphadenitis.
There was also a relative increase in TGF- as well as
FoxP3⫹ Treg cells co-expressing CTLA-4 and GITR inside Mtb granulomas. Our present findings support the
hypothesis that Treg cells induced or accumulated in
response to TB infection may act locally to suppress
immune activation at the site of bacterial replication.
It is generally believed that NO is an important first line
of defense that limits or prevents early intracellular growth
of mycobacteria. However, even though NO has been
determined to be important for TB control in the
mouse,36,37 the clinical relevance of NO produced in
human TB infection38,39 has not been properly evaluated.
Importantly, oxidative stress and/or NO produced on
chronic inflammatory conditions may inhibit T cell activation and expansion.40 It has been shown that murine
CD8⫹ T cells are significantly more sensitive to APCderived NO as compared with CD4⫹ T cells41 or CD4⫹
CD25⫹ Treg cells.42 Accordingly, we demonstrate that
CD8⫹ T cells were mostly found in the parafollicular
areas outside the granuloma and were not co-localized
with MPT64-positive macrophages, suggesting that CTLs
cannot mediate killing of TB infected cells inside the
lesions. Possibly, high local concentrations of NO inside
the granulomas may restrict bacterial growth but simul-
taneously prevent important CTL responses. This type of
immune suppression of pathogen-specific effector T cells
may have severe clinical consequences on disease progression and requires further investigation.
Previous studies suggest that functional CD8⫹ T cells
are required in sterilizing immunity to TB43-45 and that TB
infected cells can be lysed by CTLs expressing perforin46 and granulysin.47 Adults16 and children48 with
active TB had significantly lower plasma granulysin levels
compared with controls, suggesting that granulysin is
important in eradication of TB infected cells. In a recent
study, it was also reported that granulysin and perforin,
but not FasL, contribute to the capacity of human peptide-specific CD4⫹ T cell clones to lyse infected target
cells and to inhibit intracellular mycobacterial growth.49
Interestingly, patients with mutations in the gene encoding perforin possess deficient lymphocyte cytotoxicity
due to a severely reduced capacity to degranulate and
lyse infected cells, which results in an inability to induce
target cell killing.50 Accordingly, it has been determined
that both acute and chronic HIV infection in adults is
associated with deficient expression of perforin in HIVspecific CD8⫹ effector T cells.29,51 Inadequate differentiation of CD8⫹ T cells and activation of dendritic cells
due to lack of CD4⫹ T cell help may partly explain this
insufficient HIV response.52 Similarly, active immunosuppression induced in TB may inhibit cytolytic activity and
bacterial clearance due to functional inactivation and a
subsequent inability of CD4⫹ T cells to provide necessary help to CTLs.
Although it is known that CD4⫹ T cells producing IFN-␥
are essential for protective immunity in TB, it is very likely
that antigen-specific polyfunctional T cells characterized
by the coordinated expression of multiple effector functions, including other inflammatory cytokines, chemokines and effector molecules contribute to achieve full
protection against TB.53,54 Recently it was described that
a subset of Mtb-specific multifunctional CD4⫹ effector
memory T cells co-expressing granulocyte macrophage
colony-stimulating factor (GM-CSF), IFN-␥, and TNF-␣
were increased in children with latent but not active TB.53
A coordinated T cell expression of perforin and granulysin with IFN-␥55,56 or CCL514 has also been shown to be
required for control of mycobacterial growth and curative
host responses in patients with TB.16 Interestingly, depletion of IL-17 during Mtb infection in mice reduced chemokine expression and subsequent accumulation of
IFN-␥ producing CD4⫹ T cells in the lung, suggesting
that Th17 cells regulate infiltration of CD4⫹ T cells with
anti-mycobacterial properties at the site of infection.8
More than 20% of cytokine-producing CD4⫹ T cells in
peripheral blood of healthy, mycobacteria-exposed
adults expressed IL-17.57 In addition, Mtb-specific memory T cells have been found to produce substantial
amounts of both IFN-␥ and IL-17.58 Thus, the quality and
magnitude of multiple T cell effector functions most certainly serves as an immune correlate of disease protection and is therefore important in the immunopathogenesis of TB.
Previously, we have demonstrated that perforin and
granulysin are deficient in pathological lung biopsies
�Few CD8⫹ Effector T Cells in Human TB 2221
AJP June 2009, Vol. 174, No. 6
from adult patients with active pulmonary TB.39 Interestingly, despite an elevated infiltration of T cells, perforin
and granulysin expression was selectively low in the TB
lesions compared with distal lung parenchyma. In TB
lymphadenitis, T cells co-expressing both perforin and
granulysin were mostly found in the parafollicular areas
whereas granulomas primarily contained low levels of
single-positive cells. Thus, in both TB infected lung39 and
lymph nodes it seems as if this CTL defect is compartmentalized, being locally restricted to the granulomatous
lesions. Granzyme A was abundantly expressed in both
lung39 and lymph node granulomas, indicating that the
impairment of perforin and granulysin in CD8⫹ T cells is
selective. Although it has previously been described that
CD8⫹ T cells are mainly found in the peripheral regions
of the granuloma in human,3,59 murine60 and bovine61
TB, this phenomenon has never been properly investigated. An outer mantle of activated CD8⫹ T cells may be
enough to restrain granuloma advancement but may be
insufficient to mediate contact-dependent killing of infected cells and eradication of infection.
TB is a pathogen associated with delayed type hypersensitivity (DTH) and chronic inflammation, which often
results in extensive fibrosis and tissue destruction. Th2
and anti-inflammatory cytokines such as IL-4, IL-13, IL10, and TGF-, have the important function of preventing
severe immunopathology in TB infection, but if produced
in excess before CTL activation, these cytokines efficiently antagonize Th1 induced TB-immunity.62 In this
study, we found a significant induction of TGF- and also
IL-13, with a less pronounced induction of IL-10 and no
change in IL-4 mRNA levels compared with the control.
Premature induction of an immunosuppressive response
may blunt important CTL activity and instead enhance
pathological alterations in TB infected tissue. Here it has
been shown that high levels of TGF- correlate with massive fibrosis and deposition of collagen type I in the
lymphatic tissue of SIV infected rhesus macaques.63 It is
well-established that IL-4 and IL-13 can subvert Th1mediated immunity and promote inappropriate activation
of macrophages.9 Here, stimulation of peripheral blood
CD4⫹ T cells from BCG-vaccinated cattle enhanced transcription of perforin, granulysin and IFN-␥ but also IL-4
and IL-13.64 In addition, Mtb granulomas in the human
lung that were positive for IL-4 were always positive for
IFN-␥.65 Novel findings also provide evidence that IL-4
and IL-13 abrogated IFN-␥ induced autophagy and autophagy-mediated killing of intracellular mycobacteria in murine and human macrophages.66 These results suggest that
a Th1 response is mounted simultaneously with a Th2 response, which may prevent full protection provided by Th1induced immunity. Thus, long-term control of TB infection
may require a coordinated Th1 response together with inhibition of a Th2/immunoregulatory response.
In murine TB, Treg cells accumulate in high numbers
in the lung67 including all sites where CD4⫹ T cells are
found, specifically perivascular/peribronchiolar regions and within lymphoid aggregates of pulmonary
granulomas.17 Several recent studies report that CD4⫹
CD25⫹FoxP3⫹ natural Treg cells are increased in the
blood and at disease sites in human TB.68-70 Recently, it
was also shown that antigen-specific induction of FoxP3
was predictive for active versus latent TB infection in
humans.71 Treg cell-mediated suppression of CTL activity in viral infections21-24,72 and cancer73,74 has previously been described to involve impaired proliferation,
degranulation and expression of perforin and granzymes
in dysfunctional CD8⫹ T cells. Human Treg cells from
hepatitis C patients, could suppress proliferation and the
intracellular expression of perforin in activated CD8⫹ T
cells, which may explain the low frequencies and retarded maturation state of virus-specific CTLs.23 Functional impairment of retrovirus-specific CD8⫹ T cells
have been shown to be associated with an expansion of
CD25⫹FoxP3⫹ T cells in vivo.72 Accordingly, in vivo depletion of CD25⫹ Treg cells significantly enhanced
CD8⫹ T cell responses to virus-transformed cells.24,75 In
this study, a significantly decreased ratio of CD8⫹ T cells
to FoxP3⫹ Treg cells was found in the granulomatous
lesions of TB infected lymph nodes. Interestingly, patients with a progressive HIV infection have been shown
to have significantly increased levels of FoxP3 mRNA76
but low levels of perforin in CD8⫹ CTLs51 as compared
with HIV non-progressors. Accumulation of FoxP3⫹
Tregs at the site of viral replication seems to involve a
redistribution of Treg cells from blood to lymphoid tissue.32
Kinter et al have demonstrated that CD25⫹FoxP3⫹ Treg
cells isolated from both lymph nodes and peripheral
blood significantly suppress HIV-specific CTL function.22,77 Importantly, the suppressive activity by tissueassociated Treg cells at the site of infection in the lymph
nodes was particularly potent, especially in patients with
high levels of plasma viremia.22 An early Treg cell response during acute SIV infection may contribute to viral
persistence by prematurely limiting the CTL response
before the infection is cleared.78 In addition it has been
shown that increased numbers of intratumoral Treg cells
correlated with low numbers of CD8⫹ T cells in biopsy
specimens from patients with B-cell non-Hodgkin’s lymphoma.74 This supports functional findings in vitro showing that intratumoral Treg cells inhibit granule production
in CD8⫹ T cells, thus making lymphoma B cells resistant
to CTL-mediated apoptosis. Similar findings in clinical
TB, suggest that immunosuppression observed in patients with active TB is associated with naturally occurring
Treg cells expressing high levels of mRNA for FoxP3,
TGF-, and IL-4.79 One function of TGF- could be to
repress IL-23R expression and subsequent Th17 cell
differentiation, instead favoring the development of
FoxP3⫹ Treg cells.80 Numerous studies also provide evidence that Treg cells could suppress antigen-specific
IFN-␥ production by human T cells, by which mechanism
they would limit immunopathology but also down-regulate cellular immunity.18-19,20,81 Thus, local CD4⫹ T cell
responses could also be inhibited, which may result in a
failure to recruit CD8⫹ effector T cells to the granulomatous lesions in TB. Altogether, these data propose a
function of Treg cells in dampening the magnitude of the
CTL response at the site of infection, suggesting that
Treg cells might play a key role in the control of cellular
immune responses during persistent TB.
�2222
Rahman et al
AJP June 2009, Vol. 174, No. 6
In conclusion, this study provided evidence that the
adaptive immune response in establishment of clinical TB
was skewed toward a suppressive or regulatory phenotype that may inhibited proper immune activation and
down-regulated the host response at the local site of
infection. This Th2/Treg immune response may have antagonized a Th1/Th17 response and simultaneously prevented the action of CTLs, especially during later stages
of TB infection. These results suggest that proper anti-TB
immunity was not present in the granuloma which is the
main site of bacterial replication and containment. Compartmentalization of the immune response in human TB
could be part of the reason why Mtb is never completely
eradicated but instead develops into a chronic infection.
These important findings merit further investigation, as a
potential CTL dysfunction may lead to bacterial escape,
therefore representing a novel and disease-relevant
mechanism by which Mtb evades cellular immunity. New
immunotherapies may involve targeting of certain subpopulations of Th2/Treg cells to enhance cell-mediated
immune responses that are down-regulated in patients
with TB.
6.
7.
8.
9.
10.
11.
12.
Acknowledgments
We sincerely thank Azeb Tadesse, Meseret Habtamu and
Ato Alemayehu at Armauer Hansen Research Institute,
Addis Ababa, Ethiopia, for technical assistance in the
laboratory and Dr. Ingela Berggren, SME, Karolinska University Hospital Solna, Sweden, for clinical and scientific
support. Study nurse Aregash Aragie and Dr. Amha Mekash
at Tikur Anbessa Hospital, Addis Ababa, Ethiopia, provided invaluable help organizing patient recruitment and
case record forms. We also thank Prof. Markus Maeurer
at the Section for Clinical Immunology, Dr. Sven Hoffner
at the Dept. of Bacteriology and the personnel at the P3
safety laboratory, Swedish Institute for Infectious Disease
Control, Sweden, for providing excellent laboratory facilities as well as technical support. Anette Hofmann and
Cecilia Andersson at the Center for Infectious Medicine,
Karolinska Institutet, Sweden, provided invaluable technical help with confocal microscopy and immunohistochemical staining respectively.
References
1. Davis JM, Ramakrishnan L: The role of the granuloma in expansion and
dissemination of early tuberculous infection. Cell 2009, 136:37– 49
2. Fenhalls G, Stevens-Muller L, Warren R, Carroll N, Bezuidenhout J,
Van Helden P, Bardin P: Localisation of mycobacterial DNA and
mRNA in human tuberculous granulomas. J Microbiol Methods 2002,
51:197–208
3. Ulrichs T, Kosmiadi GA, Trusov V, Jorg S, Pradl L, Titukhina M,
Mishenko V, Gushina N, Kaufmann SH: Human tuberculous granulomas induce peripheral lymphoid follicle-like structures to orchestrate
local host defence in the lung. J Pathol 2004, 204:217–228
4. Wolf AJ, Desvignes L, Linas B, Banaiee N, Tamura T, Takatsu K, Ernst
JD: Initiation of the adaptive immune response to Mycobacterium
tuberculosis depends on antigen production in the local lymph node,
not the lungs. J Exp Med 2008, 205:105–115
5. Newport MJ, Huxley CM, Huston S, Hawrylowicz CM, Oostra BA,
Williamson R, Levin M: A mutation in the interferon-gamma-receptor
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
gene and susceptibility to mycobacterial infection. N Engl J Med
1996, 335:1941–1949
Keane J, Gershon S, Wise RP, Mirabile-Levens E, Kasznica J,
Schwieterman WD, Siegel JN, Braun MM: Tuberculosis associated
with infliximab, a tumor necrosis factor alpha-neutralizing agent.
N Engl J Med 2001, 345:1098 –1104
Lockhart E, Green AM, Flynn JL: IL-17 production is dominated by
gammadelta T cells rather than CD4 T cells during Mycobacterium
tuberculosis infection. J Immunol 2006, 177:4662– 4669
Khader SA, Bell GK, Pearl JE, Fountain JJ, Rangel-Moreno J, Cilley
GE, Shen F, Eaton SM, Gaffen SL, Swain SL, Locksley RM, Haynes L,
Randall TD, Cooper AM: IL-23 and IL-17 in the establishment of
protective pulmonary CD4⫹ T cell responses after vaccination and
during Mycobacterium tuberculosis challenge. Nat Immunol 2007,
8:369 –377
Rook GA: Th2 cytokines in susceptibility to tuberculosis. Curr Mol
Med 2007, 7:327–337
de la Barrera S, Aleman M, Musella R, Schierloh P, Pasquinelli V,
Garcia V, Abbate E, Sasiain Mdel C: IL-10 down-regulates costimulatory molecules on Mycobacterium tuberculosis-pulsed macrophages and impairs the lytic activity of CD4 and CD8 CTL in tuberculosis patients. Clin Exp Immunol 2004, 138:128 –138
Lienhardt C, Azzurri A, Amedei A, Fielding K, Sillah J, Sow OY, Bah B,
Benagiano M, Diallo A, Manetti R, Manneh K, Gustafson P, Bennett S,
D’Elios MM, McAdam K, Del Prete G: Active tuberculosis in Africa is
associated with reduced Th1 and increased Th2 activity in vivo. Eur
J Immunol 2002, 32:1605–1613
Stenger S, Hanson DA, Teitelbaum R, Dewan P, Niazi KR, Froelich
CJ, Ganz T, Thoma-Uszynski S, Melian A, Bogdan C, Porcelli SA,
Bloom BR, Krensky AM, Modlin RL: An antimicrobial activity of cytolytic T cells mediated by granulysin. Science 1998, 282:121–125
Dieli F, Troye-Blomberg M, Ivanyi J, Fournie JJ, Krensky AM, Bonneville
M, Peyrat MA, Caccamo N, Sireci G, Salerno A: Granulysin-dependent
killing of intracellular and extracellular Mycobacterium tuberculosis by
Vgamma9/Vdelta2 T lymphocytes. J Infect Dis 2001, 184:1082–1085
Stegelmann F, Bastian M, Swoboda K, Bhat R, Kiessler V, Krensky
AM, Roellinghoff M, Modlin RL, Stenger S: Coordinate expression of
CC chemokine ligand 5, granulysin, and perforin in CD8⫹ T cells
provides a host defense mechanism against Mycobacterium tuberculosis. J Immunol 2005, 175:7474 –7483
Dieli F, Sireci G, Caccamo N, Di Sano C, Titone L, Romano A, Di Carlo
P, Barera A, Accardo-Palumbo A, Krensky AM, Salerno A: Selective
depression of interferon-gamma and granulysin production with increase of proliferative response by Vgamma9/Vdelta2 T cells in children with tuberculosis. J Infect Dis 2002, 186:1835–1839
Sahiratmadja E, Alisjahbana B, Buccheri S, Di Liberto D, de Boer T,
Adnan I, van Crevel R, Klein MR, van Meijgaarden KE, Nelwan RH,
van de Vosse E, Dieli F, Ottenhoff TH: Plasma granulysin levels and
cellular interferon-gamma production correlate with curative host responses in tuberculosis, while plasma interferon-gamma levels correlate with tuberculosis disease activity in adults. Tuberculosis (Edinb) 2007, 87:312–321
Scott-Browne JP, Shafiani S, Tucker-Heard G, Ishida-Tsubota K,
Fontenot JD, Rudensky AY, Bevan MJ, Urdahl KB: Expansion and function of Foxp3-expressing T regulatory cells during tuberculosis. J Exp
Med 2007, 204:2159 –2169
Garg A, Barnes PF, Roy S, Quiroga MF, Wu S, Garcia VE, Krutzik SR,
Weis SE, Vankayalapati R: Mannose-capped lipoarabinomannanand prostaglandin E2-dependent expansion of regulatory T cells in
human Mycobacterium tuberculosis infection. Eur J Immunol 2008,
38:459 – 469
Li L, Lao SH, Wu CY: Increased frequency of CD4(⫹)CD25(high)
Treg cells inhibit BCG-specific induction of IFN-gamma by CD4(⫹) T
cells from TB patients. Tuberculosis (Edinb) 2007, 87:526 –534
Li L, Wu CY: CD4⫹ CD25⫹ Treg cells inhibit human memory gammadelta T cells to produce IFN-gamma in response to M tuberculosis
antigen ESAT-6. Blood 2008, 111:5629 –5636
Iwashiro M, Messer RJ, Peterson KE, Stromnes IM, Sugie T, Hasenkrug
KJ: Immunosuppression by CD4⫹ regulatory T cells induced by chronic
retroviral infection. Proc Natl Acad Sci USA 2001, 98:9226 –9230
Kinter A, McNally J, Riggin L, Jackson R, Roby G, Fauci AS: Suppression of HIV-specific T cell activity by lymph node CD25⫹ regulatory T cells from HIV-infected individuals. Proc Natl Acad Sci USA
2007, 104:3390 –3395
�Few CD8⫹ Effector T Cells in Human TB
2223
AJP June 2009, Vol. 174, No. 6
23. Rushbrook SM, Ward SM, Unitt E, Vowler SL, Lucas M, Klenerman P,
Alexander GJ: Regulatory T cells suppress in vitro proliferation of
virus-specific CD8⫹ T cells during persistent hepatitis C virus infection. J Virol 2005, 79:7852–7859
24. Suvas S, Kumaraguru U, Pack CD, Lee S, Rouse BT: CD4⫹CD25⫹ T
cells regulate virus-specific primary and memory CD8⫹ T cell responses. J Exp Med 2003, 198:889 –901
25. Parsons LM, Brosch R, Cole ST, Somoskovi A, Loder A, Bretzel G,
Van Soolingen D, Hale YM, Salfinger M: Rapid and simple approach for identification of Mycobacterium tuberculosis complex
isolates by PCR-based genomic deletion analysis. J Clin Microbiol
2002, 40:2339 –2345
26. Tsolaki AG, Hirsh AE, DeRiemer K, Enciso JA, Wong MZ, Hannan M,
Goguet de la Salmoniere YO, Aman K, Kato-Maeda M, Small PM:
Functional and evolutionary genomics of Mycobacterium tuberculosis:
insights from genomic deletions in 100 strains. Proc Natl Acad Sci USA
2004, 101:4865– 4870
27. Andersson J, Abrams J, Bjork L, Funa K, Litton M, Agren K, Andersson
U: Concomitant in vivo production of 19 different cytokines in human
tonsils. Immunology 1994, 83:16 –24
28. Bjork L, Fehniger TE, Andersson U, Andersson J: Computerized
assessment of production of multiple human cytokines at the singlecell level using image analysis. J Leukoc Biol 1996, 59:287–295
29. Andersson J, Behbahani H, Lieberman J, Connick E, Landay A,
Patterson B, Sonnerborg A, Lore K, Uccini S, Fehniger TE: Perforin is
not co-expressed with granzyme A within cytotoxic granules in CD8 T
lymphocytes present in lymphoid tissue during chronic HIV infection.
Aids 1999, 13:1295–1303
30. Agren K, Andersson U, Litton M, Funa K, Nordlander B, Andersson J:
The production of immunoregulatory cytokines is localized to the extrafollicular area of human tonsils. Acta Otolaryngol 1996, 116:477– 485
31. Behbahani H, Landay A, Patterson BK, Jones P, Pottage J, Agnoli M,
Andersson J, Spetz AL: Normalization of immune activation in lymphoid tissue following highly active antiretroviral therapy. J Acquir
Immune Defic Syndr 2000, 25:150 –156
32. Andersson J, Boasso A, Nilsson J, Zhang R, Shire NJ, Lindback S,
Shearer GM, Chougnet CA: The prevalence of regulatory T cells in
lymphoid tissue is correlated with viral load in HIV-infected patients.
J Immunol 2005, 174:3143–3147
33. Mustafa T, Wiker HG, Mfinanga SG, Morkve O, Sviland L: Immunohistochemistry using a Mycobacterium tuberculosis complex specific
antibody for improved diagnosis of tuberculous lymphadenitis. Mod
Pathol 2006, 19:1606 –1614
34. Ulrichs T, Lefmann M, Reich M, Morawietz L, Roth A, Brinkmann V,
Kosmiadi GA, Seiler P, Aichele P, Hahn H, Krenn V, Gobel UB,
Kaufmann SH: Modified immunohistological staining allows detection of Ziehl-Neelsen-negative Mycobacterium tuberculosis organisms and their precise localization in human tissue. J Pathol 2005,
205:633– 640
35. Livak KJ, Schmittgen TD: Analysis of relative gene expression data
using real-time quantitative PCR and the 2(⫺delta delta C[T])
method. Methods 2001, 25:402– 408
36. Scanga CA, Mohan VP, Tanaka K, Alland D, Flynn JL, Chan J: The
inducible nitric oxide synthase locus confers protection against aerogenic challenge of both clinical and laboratory strains of Mycobacterium tuberculosis in mice. Infect Immun 2001, 69:7711–7717
37. Jung YJ, LaCourse R, Ryan L, North RJ: Virulent but not avirulent
Mycobacterium tuberculosis can evade the growth inhibitory action of
a T helper 1-dependent, nitric oxide Synthase 2-independent defense
in mice. J Exp Med 2002, 196:991–998
38. Nicholson S, Bonecini-Almeida Mda G, Lapa e Silva JR, Nathan C,
Xie QW, Mumford R, Weidner JR, Calaycay J, Geng J, Boechat N,
Linhares C, Rom W, Ho JL: Inducible nitric oxide synthase in pulmonary alveolar macrophages from patients with tuberculosis. J Exp
Med 1996, 183:2293–2302
39. Andersson J, Samarina A, Fink J, Rahman S, Grundstrom S: Impaired
expression of perforin and granulysin in CD8⫹ T cells at the site of
infection in human chronic pulmonary tuberculosis. Infect Immun
2007, 75:5210 –5222
40. Dietlin TA, Hofman FM, Lund BT, Gilmore W, Stohlman SA, van der
Veen RC: Mycobacteria-induced Gr-1⫹ subsets from distinct myeloid
lineages have opposite effects on T cell expansion. J Leukoc Biol
2007, 81:1205–1212
41. Hoffman RA, Mahidhara RS, Wolf-Johnston AS, Lu L, Thomson AW,
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
Simmons RL: Differential modulation of CD4 and CD8 T-cell proliferation by induction of nitric oxide synthesis in antigen presenting cells.
Transplantation 2002, 74:836 – 845
Loeffler M, Kruger JA, Reisfeld RA: Immunostimulatory effects of
low-dose cyclophosphamide are controlled by inducible nitric oxide
synthase. Cancer Res 2005, 65:5027–5030
Flynn JL, Goldstein MM, Triebold KJ, Koller B, Bloom BR: Major
histocompatibility complex class I-restricted T cells are required for
resistance to Mycobacterium tuberculosis infection. Proc Natl Acad
Sci USA 1992, 89:12013–12017
Behar SM, Dascher CC, Grusby MJ, Wang CR, Brenner MB: Susceptibility of mice deficient in CD1D or TAP1 to infection with Mycobacterium tuberculosis. J Exp Med 1999, 189:1973–1980
Lalvani A, Brookes R, Wilkinson RJ, Malin AS, Pathan AA, Andersen
P, Dockrell H, Pasvol G, Hill AV: Human cytolytic and interferon
gamma-secreting CD8⫹ T lymphocytes specific for Mycobacterium
tuberculosis. Proc Natl Acad Sci USA 1998, 95:270 –275
Serbina NV, Liu CC, Scanga CA, Flynn JL: CD8⫹ CTL from lungs of
Mycobacterium tuberculosis-infected mice express perforin in vivo
and lyse infected macrophages. J Immunol 2000, 165:353–363
Gansert JL, Kiessler V, Engele M, Wittke F, Rollinghoff M, Krensky
AM, Porcelli SA, Modlin RL, Stenger S: Human NKT cells express
granulysin and exhibit antimycobacterial activity. J Immunol 2003,
170:3154 –3161
Di Liberto D, Buccheri S, Caccamo N, Meraviglia S, Romano A, Di
Carlo P, Titone L, Dieli F, Krensky AM, Salerno A: Decreased serum
granulysin levels in childhood tuberculosis which reverse after therapy. Tuberculosis (Edinb) 2007, 87:322–328
Klucar P, Barnes PF, Kong Y, Samten B, Tvinnereim A, Spallek R,
Nepom GT, Singh M, Shams H: Characterization of effector functions
of human peptide-specific CD4⫹ T-cell clones for an intracellular
pathogen. Hum Immunol 2008, 69:475– 483
Bryceson YT, Rudd E, Zheng C, Edner J, Ma D, Wood SM, Bechensteen
AG, Boelens JJ, Celkan T, Farah RA, Hultenby K, Winiarski J, Roche PA,
Nordenskjold M, Henter JI, Long EO, Ljunggren HG: Defective cytotoxic
lymphocyte degranulation in syntaxin-11 deficient familial hemophagocytic lymphohistiocytosis 4 (FHL4) patients. Blood 2007, 110:1906 –1915
Andersson J, Kinloch S, Sonnerborg A, Nilsson J, Fehniger TE, Spetz
AL, Behbahani H, Goh LE, McDade H, Gazzard B, Stellbrink H,
Cooper D, Perrin L: Low levels of perforin expression in CD8⫹ T
lymphocyte granules in lymphoid tissue during acute human immunodeficiency virus type 1 infection. J Infect Dis 2002, 185:1355–1358
Lore K, Sonnerborg A, Brostrom C, Goh LE, Perrin L, McDade H,
Stellbrink HJ, Gazzard B, Weber R, Napolitano LA, van Kooyk Y,
Andersson J: Accumulation of DC-SIGN⫹CD40⫹ dendritic cells with
reduced CD80 and CD86 expression in lymphoid tissue during acute
HIV-1 infection. Aids 2002, 16:683– 692
Mueller H, Detjen AK, Schuck SD, Gutschmidt A, Wahn U, Magdorf K,
Kaufmann SH, Jacobsen M: Mycobacterium tuberculosis-specific
CD4⫹, IFNgamma⫹, and TNFalpha⫹ multifunctional memory T cells
coexpress GM-CSF. Cytokine 2008, 43:143–148
Betts MR, Nason MC, West SM, De Rosa SC, Migueles SA, Abraham
J, Lederman MM, Benito JM, Goepfert PA, Connors M, Roederer M,
Koup RA: HIV nonprogressors preferentially maintain highly functional HIV-specific CD8⫹ T cells. Blood 2006, 107:4781– 4789
Temmerman ST, Place S, Debrie AS, Locht C, Mascart F: Effector
functions of heparin-binding hemagglutinin-specific CD8⫹ T lymphocytes in latent human tuberculosis. J Infect Dis 2005, 192:226 –232
Worku S, Hoft DF: Differential effects of control and antigen-specific T
cells on intracellular mycobacterial growth. Infect Immun 2003,
71:1763–1773
Scriba TJ, Kalsdorf B, Abrahams DA, Isaacs F, Hofmeister J, Black G,
Hassan HY, Wilkinson RJ, Walzl G, Gelderbloem SJ, Mahomed H,
Hussey GD, Hanekom WA: Distinct, specific IL-17- and IL-22-producing CD4⫹ T cell subsets contribute to the human anti-mycobacterial
immune response. J Immunol 2008, 180:1962–1970
Acosta-Rodriguez EV, Rivino L, Geginat J, Jarrossay D, Gattorno M,
Lanzavecchia A, Sallusto F, Napolitani G: Surface phenotype and
antigenic specificity of human interleukin 17-producing T helper
memory cells. Nat Immunol 2007, 8:639 – 646
van den Oprd JJ, de Wolf-Peeters C, Facchetti F, Desmet VJ: Cellular
composition of hypersensitivity-type granulomas: immunohistochemical analysis of tuberculous and sarcoidal lymphadenitis. Hum Pathol
1984, 15:559 –565
�2224
Rahman et al
AJP June 2009, Vol. 174, No. 6
60. Gonzalez-Juarrero M, Turner OC, Turner J, Marietta P, Brooks JV,
Orme IM: Temporal and spatial arrangement of lymphocytes within
lung granulomas induced by aerosol infection with Mycobacterium
tuberculosis. Infect Immun 2001, 69:1722–1728
61. Liebana E, Marsh S, Gough J, Nunez A, Vordermeier HM, Whelan A,
Spencer Y, Clifton-Hardley R, Hewinson G, Johnson L: Distribution
and activation of T-lymphocyte subsets in tuberculous bovine lymphnode granulomas. Vet Pathol 2007, 44:366 –372
62. Freeman S, Post FA, Bekker LG, Harbacheuski R, Steyn LM, Ryffel B,
Connell ND, Kreiswirth BN, Kaplan G: Mycobacterium tuberculosis
H37Ra and H37Rv differential growth and cytokine/chemokine induction in murine macrophages in vitro. J Interferon Cytokine Res 2006,
26:27–33
63. Estes JD, Wietgrefe S, Schacker T, Southern P, Beilman G, Reilly C,
Milush JM, Lifson JD, Sodora DL, Carlis JV, Haase AT: Simian immunodeficiency virus-induced lymphatic tissue fibrosis is mediated by
transforming growth factor beta 1-positive regulatory T cells and
begins in early infection. J Infect Dis 2007, 195:551–561
64. Endsley JJ, Hogg A, Shell LJ, McAulay M, Coffey T, Howard C,
Capinos Scherer CF, Waters WR, Nonnecke B, Estes DM, VillarrealRamos B: Mycobacterium bovis BCG vaccination induces memory
CD4⫹ T cells characterized by effector biomarker expression and
anti-mycobacterial activity. Vaccine 2007, 25:8384 – 8394
65. Fenhalls G, Stevens L, Bezuidenhout J, Amphlett GE, Duncan K,
Bardin P, Lukey PT: Distribution of IFN-gamma. IL-4 and TNF-alpha
protein and CD8 T cells producing IL-12p40 mRNA in human lung
tuberculous granulomas. Immunology 2002, 105:325–335
66. Harris J, De Haro SA, Master SS, Keane J, Roberts EA, Delgado M,
Deretic V: T helper 2 cytokines inhibit autophagic control of intracellular Mycobacterium tuberculosis. Immunity 2007, 27:505–517
67. Mason CM, Porretta E, Zhang P, Nelson S: CD4⫹ CD25⫹ transforming growth factor-beta-producing T cells are present in the lung in
murine tuberculosis and may regulate the host inflammatory response. Clin Exp Immunol 2007, 148:537–545
68. Ribeiro-Rodrigues R, Resende Co T, Rojas R, Toossi Z, Dietze R,
Boom WH, Maciel E, Hirsch CS: A role for CD4⫹CD25⫹ T cells in
regulation of the immune response during human tuberculosis. Clin
Exp Immunol 2006, 144:25–34
69. Guyot-Revol V, Innes JA, Hackforth S, Hinks T, Lalvani A: Regulatory
T cells are expanded in blood and disease sites in patients with
tuberculosis. Am J Respir Crit Care Med 2006, 173:803– 810
70. Chen X, Zhou B, Li M, Deng Q, Wu X, Le X, Wu C, Larmonier N, Zhang
W, Zhang H, Wang H, Katsanis E: CD4(⫹)CD25(⫹)FoxP3(⫹) regulatory T cells suppress Mycobacterium tuberculosis immunity in patients with active disease. Clin Immunol 2007, 123:50 –59
71. Wu B, Huang C, Kato-Maeda M, Hopewell PC, Daley CL, Krensky
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
AM, Clayberger C: Messenger RNA expression of IL-8. FOXP3, and
IL-12beta differentiates latent tuberculosis infection from disease.
J Immunol 2007, 178:3688 –3694
Zelinskyy G, Kraft AR, Schimmer S, Arndt T, Dittmer U: Kinetics of
CD8⫹ effector T cell responses and induced CD4⫹ regulatory T cell
responses during Friend retrovirus infection. Eur J Immunol 2006,
36:2658 –2670
Fu J, Xu D, Liu Z, Shi M, Zhao P, Fu B, Zhang Z, Yang H, Zhang H,
Zhou C, Yao J, Jin L, Wang H, Yang Y, Fu YX, Wang FS: Increased
regulatory T cells correlate with CD8 T-cell impairment and poor
survival in hepatocellular carcinoma patients. Gastroenterology 2007,
132:2328 –2339
Yang ZZ, Novak AJ, Ziesmer SC, Witzig TE, Ansell SM: Attenuation of
CD8(⫹) T-cell function by CD4(⫹)CD25(⫹) regulatory T cells in B-cell
non-Hodgkin’s lymphoma. Cancer Res 2006, 66:10145–10152
Haeryfar SM, DiPaolo RJ, Tscharke DC, Bennink JR, Yewdell JW:
Regulatory T cells suppress CD8⫹ T cell responses induced by
direct priming and cross-priming and moderate immunodominance
disparities. J Immunol 2005, 174:3344 –3351
Nilsson J, Boasso A, Velilla PA, Zhang R, Vaccari M, Franchini G,
Shearer GM, Andersson J, Chougnet C: HIV-1-driven regulatory Tcell accumulation in lymphoid tissues is associated with disease
progression in HIV/AIDS. Blood 2006, 108:3808 –3817
Kinter AL, Horak R, Sion M, Riggin L, McNally J, Lin Y, Jackson R,
O’Shea A, Roby G, Kovacs C, Connors M, Migueles SA, Fauci AS:
CD25⫹ regulatory T cells isolated from HIV-infected individuals suppress the cytolytic and nonlytic antiviral activity of HIV-specific CD8⫹
T cells in vitro. AIDS Res Hum Retroviruses 2007, 23:438 – 450
Estes JD, Li Q, Reynolds MR, Wietgrefe S, Duan L, Schacker T, Picker
LJ, Watkins DI, Lifson JD, Reilly C, Carlis J, Haase AT: Premature
induction of an immunosuppressive regulatory T cell response during
acute simian immunodeficiency virus infection. J Infect Dis 2006,
193:703–712
Roberts T, Beyers N, Aguirre A, Walzl G: Immunosuppression during
active tuberculosis is characterized by decreased interferon- gamma
production and CD25 expression with elevated forkhead box P3,
transforming growth factor- beta, and interleukin-4 mRNA levels. J Infect Dis 2007, 195:870 – 878
Zhou L, Lopes JE, Chong MM, Ivanov II, Min R, Victora GD, Shen Y,
Du J, Rubtsov YP, Rudensky AY, Ziegler SF, Littman DR: TGF-betainduced Foxp3 inhibits T(H)17 cell differentiation by antagonizing
RORgammat function. Nature 2008, 453:236 –240
Hougardy JM, Place S, Hildebrand M, Drowart A, Debrie AS, Locht C,
Mascart F: Regulatory T cells depress immune responses to protective antigens in active tuberculosis. Am J Respir Crit Care Med 2007,
176:409 – 416
�
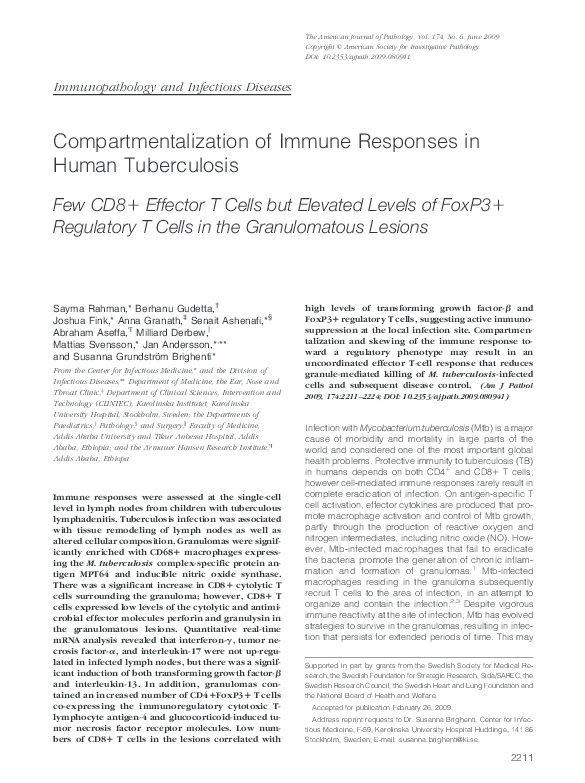
 Abraham Aseffa
Abraham Aseffa