Sports Med 2007; 37 (12): 1019-1028
0112-1642/07/0012-1019/$44.95/0
CURRENT OPINION
2007 Adis Data Information BV. All rights reserved.
Criteria for Determination of Maximal
Oxygen Uptake
A Brief Critique and Recommendations for Future Research
Adrian W. Midgley,1 Lars R. McNaughton,1 Remco Polman1 and David Marchant2
1
2
Department of Sport, Health and Exercise Science, University of Hull, Hull, UK
Department of Sport and Physical Activity, Edge Hill University, Ormskirk, UK
Abstract
Although the concept of maximal oxygen uptake (V̇O2max) was conceived as
early as 1923, the criteria used to establish whether a true V̇O2max has been
attained have been heavily criticised. Consequently, an improvement in the
methodology of the existing criteria, or development of new criteria, is required.
In order to be valid across experimental studies, new or improved criteria need to
be independent of exercise modality, test protocol and subject characteristics. One
procedure that has shown potential for yielding valid V̇O2max criteria is the
verification phase, which consists of a supramaximal constant speed run to
exhaustion performed after the incremental phase of a V̇O2max test. A peak
oxygen uptake (V̇O2peak) in the verification phase that is similar (within the
tolerance of measurement error, e.g. within 2%) to the V̇O2max value attained in
the incremental phase would indicate that a true V̇O2max has been elicited.
Verification of the maximal heart rate would also indicate that a subject has given
a maximum effort. Although the validity of the present methodology for identifying an oxygen uptake (V̇O2) plateau is questionable, a V̇O2 plateau criterion based
on the individual slope of the V̇O2-work-rate relationship should improve its
validity. This approach also allows determination of the ‘total V̇O2 plateau’,
which is in contrast to currently used V̇O2 plateau criteria that are based on the
difference in V̇O2 between only two test stages or V̇O2 data points. The ratings of
perceived exertion scale has been criticised for being a one-dimensional measure
of physical effort and V̇O2max criteria based on a multidimensional psychophysiological approach should increase validity. Visual analogue scales can be used to
assess aspects such as muscular pain, determination and overall perceived effort.
Furthermore, they are easy to complete and have demonstrated good reliability
and validity in clinical and health settings. Future research should explore these
and other potential approaches to developing new or improved V̇O2max criteria, so
that, ultimately, a standardised set of V̇O2max criteria can be established. At
present, however, the greatest challenge is identifying V̇O2max criteria that remain
valid across studies.
Although the concept of maximal oxygen uptake
(V̇O2max) was conceived as early as 1923,[1] the
validity of some of the test procedures, such as the
recommended test duration[2] and appropriate
�Midgley et al.
1020
breath-by-breath data averaging methods[3] have not
been adequately supported by experimental research. Another procedure that has not undergone
rigorous scientific scrutiny is the application of criteria used to establish whether a ‘true’ V̇O2max has
been attained (hereafter referred to as V̇O2max criteria). The application of valid and objective V̇O2max
criteria is for quality assurance during experimental
research, so that invalid V̇O2max values, due to poor
subject effort[4] or inappropriate test protocols,[2] do
not confound the interpretation of the findings. This
may be particularly important when comparing the
results of cross-sectional studies, as opposed to longitudinal studies, where a consistent effort during
repeated testing for the latter, may be comparatively
more important. This article provides a brief critique
of currently used V̇O2max criteria and makes recommendations for future research that might identify
criteria that possess greater validity than those currently used.
1. Currently Used Maximal Oxygen
Uptake (V̇O2max) Criteria
Howley et al.[5] reported the frequency with
which V̇O2max criteria were used in studies published in Medicine and Science in Sports and Exercise between October 1993 and May 1994 (table I).
We surveyed studies published between October
2005 and May 2006 in the same journal (table I),
which highlights that despite heavy criticism,[5-7] the
use of V̇O2max criteria has changed little over the
past 12 years. There appears to be no change in the
type or number of criteria used, or the consistency in
the threshold values used to define each criterion.
However, in the original 1993–4 survey, 76% of
studies reported one or more V̇O2max criteria, compared with 44% in our 2005–6 survey. The criticisms that have been directed at the V̇O2max criteria[5-7] may be the cause of this apparent reduction in
their use. Small sample bias relating to these
surveys, or a change in editorial decisions regarding
acceptance of studies not reporting V̇O2max criteria,
are also possible explanations. In an attempt to
provide a broader view of currently used V̇O2max
criteria, we also surveyed studies published in four
2007 Adis Data Information BV. All rights reserved.
prominent (based on impact factor) sports science
and applied physiology journals between August
2005 and July 2006 (table I). This larger survey
further emphasises the considerable variation in currently used V̇O2max criteria, as well as the relatively
high percentage (62%) of studies that do not use or
report criteria.
2. A Brief Critique of Current
V̇O2max Criteria
Howley et al.[5] highlighted that the oxygen uptake (V̇O2) plateau, respiratory exchange ratio, and
blood lactate criteria originated from experimental
studies conducted over 40 years ago.[4,8,9] Several
authors have suggested that since these studies used
specific exercise modalities, test protocols and subjects, directly applying any of these criteria to studies using different experimental methodology and
subjects is unlikely to be valid.[5,10-12] Moreover, we
question the validity of the criteria in relation to the
methodology and subjects used in the original studies.
A V̇O2 plateau is defined as a small or no increase in V̇O2 in response to an increase in work
rate[4] and is used to demonstrate that the rate of
oxygen transport and utilisation has reached its limit. However, unless an absolute plateau is used (i.e.
no increase in V̇O2), a V̇O2 plateau indicates only
that the rate of change in the V̇O2-work-rate relationship has slowed, not that V̇O2 has reached its
maximum. The peak value achieved may instead be
related to the subject’s limit of exercise tolerance or
level of effort, rather than a limit of oxygen transport
and utilisation. The term peak oxygen uptake
(V̇O2peak) has been considered more appropriate
where no V̇O2 plateau is evident.[13] However, the
terms V̇O2max and V̇O2peak have been used inconsistently and we believe the term V̇O2peak should be
used only in clinical settings where exercise tolerance is symptom limited in conjunction with a
pathophysiological condition. This suggestion is
based on the observation that when subjects perform
two identical V̇O2max tests, but demonstrate a V̇O2
plateau in only one of the tests, there is no appreciable difference in V̇O2max between the two
Sports Med 2007; 37 (12)
�Maximal Oxygen Uptake Criteria
1021
Table I. Criteria used for maximal oxygen uptake (V̇O2max) determination in: 29 studies published in Medicine and Science in Sports and
Exercise (MSSE) between October 1993 and May 1994;[5] 39 studies published in MSSE between October 2005 and May 2006; and 207
studies published in four prominent (based on impact factor) sports medicine and applied physiology journals between August 2005 and
July 2006
Criterion
Value used
MSSE
1993–4
MSSE
2005–6
Four journals
2005–6
7
22
128
Unspecified
3
7
28
Absolute plateau
1
0
2
≤2.1 mL/kg/min
4
1
10
≤100 mL/min
0
0
5
≤150 mL/min
3
1
14
≤200 mL/min
0
1
2
≤280 mL/min
1
0
0
V̇O2 less than predicted
1
0
0
≥10 mmol/L
0
0
3
≥8 mmol/L
1
1
6
≥1.20
0
0
1
≥1.15
0
0
9
≥1.13
1
0
0
≥1.12
0
0
1
≥1.10
7
13
55
≥1.08
0
0
1
≥1.05
2
0
3
≥1.00
4
1
5
Plateau
1
1
4
None stated
V̇O2 plateau
BLa concentration
RER
Heart rate
±5 beats/min APMHR
3
3
3
±10 beats/min APMHR
0
1
16
±15 beats/min APMHR
1
0
0
≥100% APMHR
2
1
13
≥95% APMHR
0
1
8
≥90% APMHR
3
1
11
≥85% APMHR
0
1
3
Within 1 SD of APMHR
0
0
1
Close to APMHR
0
0
1
≥19
?
1
1
≥18
?
2
5
≥17
?
0
1
V̇O2max verification
<135 mL/min
?
0
1
V̇E/V̇O2
>30–35
RPE
?
1
1
Reduced pedal rate
?
3
14
Subject exhaustion
?
1
9
Lower limb fatigue
?
0
2
Signs of intense effort
?
0
2
Dyspnoea
?
0
1
APMHR = age-predicted maximal heart rate; BLa = blood lactate; RER = respiratory exchange ratio; RPE = rating of perceived exertion;
V̇E = minute ventilation; V̇O2 = oxygen uptake; ? indicates not surveyed/reported by Howley et al.[5]
tests.[11,14] The V̇O2 plateau criterion is particularly
limited when the plateau threshold value is not relat-
2007 Adis Data Information BV. All rights reserved.
ed to the expected change in V̇O2 for each stage
increment for a particular individual. The V̇O2 pla-
Sports Med 2007; 37 (12)
�1022
teau criterion threshold of ≤150 mL/min (or ≤2.1
mL/kg/min) first introduced by Taylor et al.,[4] was
based on a mean increase in V̇O2 of 299 ± 86 mL/
min per stage increment for all subjects. The
standard deviation of the mean V̇O2 response indicates that the expected change in V̇O2 for each stage
increment, for some subjects, would have been less
than the V̇O2 plateau criterion threshold (e.g. assuming a normal distribution, 2.5% of subjects would
have an expected change in V̇O2 for each stage
increment <130 mL/min [299 mL/min minus 1.96
SD]). This problem is particularly evident when
directly applying the V̇O2 plateau criterion of Taylor
et al.[4] to test protocols incorporating small increments, where the change in V̇O2 per stage increment
will be comparatively small. Conversely, using the
mean subject V̇O2 response will result in the V̇O2
plateau criterion threshold being a relatively small
percentage of some subjects’ change in V̇O2 for
each stage increment. These subjects would less
likely satisfy the V̇O2 plateau criterion.
Several V̇O2max criteria are based on surpassing
threshold values for the respiratory exchange ratio
and heart rate during the exercise test, or threshold
values for post-exercise blood lactate concentration,
and are used as evidence that the subject has given a
maximum effort. However, the large between-subject variation in these variables means that many
subjects will satisfy these criteria during submaximal efforts. For example, Duncan et al.[7] reported a
mean maximal post-exercise blood lactate concentration of 14.3 ± 2.7 mmol/L, indicating that most
subjects would probably have achieved the 8 mmol/
L criterion threshold if they stopped exercising some
time before reaching their limit of exercise tolerance. A large between-subject variation also means
that some subjects may not satisfy a particular criterion even when a maximum effort is given. This
limitation may be more pronounced for the heart
rate criterion based on the attainment of a percentage of the age-predicted maximal heart rate
(HRmax), since the 95% confidence interval for agepredicted HRmax has been reported to be as large as
45 beats/min.[15] The ability to satisfy particular
criteria may also be subject specific. For example,
2007 Adis Data Information BV. All rights reserved.
Midgley et al.
endurance-trained individuals have a lower capacity
for anaerobic metabolism than sprint-trained individuals,[16] and may find it more difficult to satisfy
the blood lactate and respiratory exchange ratio criteria. Although we are unaware of any studies that
have directly investigated this possibility, mean
maximal respiratory exchange ratios for endurance
athletes that are well below common threshold values for this criteria, have been reported (e.g. Meyer
et al.[17]). A statistically significant decrease in the
mean maximal respiratory exchange ratio in response to endurance training, and in association with
an enhancement of V̇O2max and the ventilatory
threshold, has also been reported.[18]
Relatively limited attention has been given to the
psychophysiological components associated with
the determination of V̇O2max, with research primarily focusing on Borg’s concept of perceived exertion,
measured using Borg’s 15-point Ratings of Perceived Exertion (RPE) Scale.[19] Hutchinson and
Tenenbaum[20] have been critical of this one-dimensional approach to the measurement of perceived
exertion, and their findings support previous research[21-23] in demonstrating that several distinct
inputs (sensory-discriminative, motivational-affective and cognitive-evaluative), perceived to different
degrees during exertion, influence the perception of
effort. Measurement of these variables has been
effectively operationalised through direct questions
during exertion. For example, Hutchinson and
Tenenbaum[20] asked participants to rate their levels
of muscular pain (sensory-discriminative), determination (motivational-affective) and effort (cognitive-evaluative) during physical exertion. The authors concluded that these sensations representing
different dimensions of effort are perceived distinctly during exercise, and operate differently over the
duration of an exertive task. Consequently, the validity of RPE and other single-item measures of
effort, is questionable, and multidimensional measures that better represent the complex psychophysiological nature of effort are required. The potential
lack of objectivity of psychological measures[24]
may also be an important limitation to the use of
RPE as a valid and reliable V̇O2max criterion. ObjecSports Med 2007; 37 (12)
�Maximal Oxygen Uptake Criteria
tivity may be particularly compromised if researchers do not give appropriate pre-test instructions to
subjects on how to interpret the RPE scale. Reduced
pedal rate and power output have been used as
objective measures to indicate that a subject has
given a maximal effort. However, the reduced pedal
rate or power output may be due to a lack of effort,
rather than an indication that a maximum effort has
been given.
An observation that highlights the limitations of
the currently used V̇O2max criteria is that we are
unaware of any studies that have reported that one or
more subjects did not satisfy the required V̇O2max
criteria. It would be hard to believe that all subjects
performing V̇O2max tests in these studies gave a
maximum effort. Possible explanations are that the
current criteria have insufficient sensitivity to detect
subjects who did not give a maximal effort, or
perhaps that some researchers have decided on appropriate criteria post hoc, to ensure no subjects
have to be omitted from their study. The lack of
standardisation of appropriate V̇O2max criteria certainly leaves the procedure of assessing the quality
of a V̇O2max test susceptible to misuse.
Although this brief critique has focused on the
limitations of using criteria for assessing the quality
of a V̇O2max test, it is noteworthy that this problem
is relevant to all test protocols used in experimental
research, where subjects are asked to push themselves to the limit of their exercise tolerance. Time
trials and measures of time to exhaustion, in particular, are common in sport and exercise science research.[25,26] To the best of our knowledge, however,
criteria have never been used in maximal tests other
than V̇O2max tests, to establish whether a maximal
effort has been given. This highlights an important
area for future research.
3. Future Research Directions
In view of the criticisms directed at currently
used V̇O2max criteria,[5-7,10-12] it would be difficult to
argue against the view that an improvement in the
methodology of the existing criteria, or development
of new criteria, is required. The remainder of this
article discusses potential directions for future re 2007 Adis Data Information BV. All rights reserved.
1023
search that may eventually identify valid and robust
V̇O2max criteria.
3.1 Verification Phase
Thoden et al.[27] recommended that after the incremental phase of a V̇O2max test, athletes should
rest for 5–15 minutes and then perform a constant
speed run to exhaustion that is a speed equivalent to
one stage higher than the last completed stage in the
incremental phase. Thoden et al.[27] termed this latter
procedure the ‘exhaustive phase’, and then later, the
‘verification phase’.[28] Although the verification
phase was used only once in studies published in
four journals surveyed over a 12-month period
(table I), two recent studies involving sedentary
individuals during cycling ergometry[29] and endurance athletes during treadmill running[11] reported
that this procedure shows potential for yielding valid
V̇O2max criteria. A V̇O2peak in the verification phase
that is similar (within the tolerance of measurement
error, e.g. within 2%[11]) to the V̇O2max value attained in the incremental phase would indicate a
high probability that a true V̇O2max has been elicited. In addition to V̇O2max verification, Midgley et
al.[11] suggested that HRmax verification would indicate that a subject has given a maximum effort, since
it is improbable that a subject could give identical
submaximal efforts during two exercise bouts with
different characteristics (i.e. incremental exercise
compared with a single square wave bout of exercise).[6]
One of the main criticisms directed at current
V̇O2max criteria is that they are specific to the exercise modalities, test protocols and subjects that were
used in the studies where the criteria originated.[5,10-12] Since exercise modality, test protocol and
subject characteristics will always vary between researchers and experimental studies, standardised
V̇O2max criteria would need to be independent of
these variables if they are to remain valid across
studies. The V̇O2max and HRmax verification criteria
appear to be independent of these variables because
the criteria are not reliant on comparisons between
the results of studies using different exercise modalities, test protocols and subjects. The test protocol
Sports Med 2007; 37 (12)
�Midgley et al.
1024
2007 Adis Data Information BV. All rights reserved.
VO2 (mL/min)
.
3000
150
2000
100
1000
50
Heart rate (beats/min)
200
4000
0
0
0
100 200 300 400 500 600 1200 1300 1400
Time (sec)
200
4000
.
3000
150
2000
100
1000
50
Heart rate (beats/min)
b
VO2 (mL/min)
0
0
0 200 400 600 800 1000
Time (sec)
1800
200
3000
150
2000
100
1000
50
.
Heart rate (beats/min)
c
4000
0
0
0
20
0
40
0
60
0
80
0
10
0
12 0
0
14 0
0
16 0
00
24
0
26 0
00
A potential limitation of the verification phase is
that due to accumulated fatigue during the incremental phase, for some subjects, the verification
phase may be too short to allow V̇O2 and heart rate
to reach their maximum.[11] Performing the incremental and verification phases on separate days[12,31]
may increase time to exhaustion in the verification
phase, by eliminating the residual fatigue effects of
the preceding incremental phase when performed on
the same day. Limitations to this approach are that
an extra visit to the laboratory would be required and
the day-to-day variation in V̇O2max[14] would reduce
the robustness of the verification procedure.
Thoden[28] recommended that the verification phase
can be extended by performing it at the same, or a
lower speed, than the peak speed attained in the
incremental phase. This approach has been used in
experimental studies by Day et al.[6] and Rossiter et
al.[29] that both involved cycling ergometry and male
subjects with a wide range of age and levels of
fitness. However, this approach does not incorporate
the principle of a V̇O2 plateau, in that V̇O2 demand
has increased due to increased exercise intensity, but
V̇O2 cannot increase sufficiently to meet this demand.[1] A multi-stage verification phase incorporating one or more relatively short stages of submaximal exercise, followed by a supramaximal effort
may improve the verification procedure by allowing
V̇O2 and heart rate more time to reach maximal
values before volitional exhaustion occurs. Since the
verification phase shows promise for yielding valid
a
.
VO2
Heart rate
VO2 (mL/min)
independence of the verification criteria has been
supported by a study that reported no statistically
significant differences between maximal V̇O2 and
heart rate values in the incremental and verification
phases of three different V̇O2max test protocols that
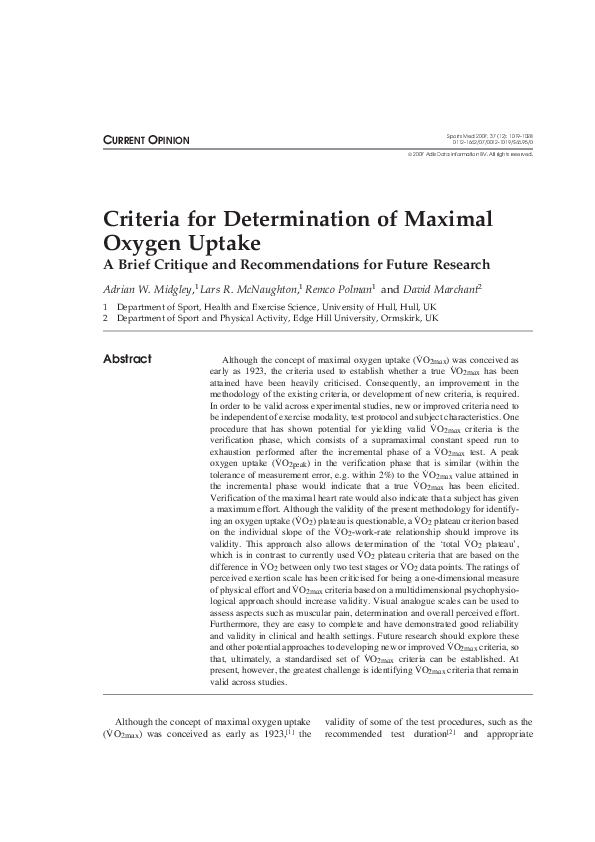
each incorporated a verification phase.[30] Figure 1
shows the V̇O2 and heart rate responses of a representative subject from this study during the incremental and verification phases of the three test protocols. Further research is required to establish the
efficacy of the verification phase for yielding
V̇O2max criteria that remain valid across studies
using different experimental methodology and subjects.
Time (sec)
Fig. 1. Oxygen uptake (V̇O2) and heart rate responses of a
34-year-old, regional level, male long-distance runner during three
maximal oxygen uptake (V̇O2max) tests, each incorporating different
incremental test phases.[30] The incremental phases were: (a) a
continuous protocol with 1-minute stage durations; (b) a discontinuous protocol with 2-minute stage durations and 30-second rest
periods; and (c) a discontinuous protocol with 3-minute stage durations and 30-second rest periods. Each incremental phase was
followed by a 10-minute rest phase and a verification phase. The
verification phase consisted of a run to exhaustion at a speed that
was equivalent to one stage higher than the last completed stage in
the incremental phase. The similarities between the maximal V̇O2
and heart rate values in the incremental and verification phases
confirms (verifies) that V̇O2max and the maximal heart rate were
elicited during the increment phases. The horizontal dashed and
dotted lines are to aid comparison of V̇O2max and heart rate values
attained in the incremental and verification phases.
Sports Med 2007; 37 (12)
�Maximal Oxygen Uptake Criteria
V̇O2max criteria, future research should investigate
different verification test protocols and criteria to
improve the validity and utility of this procedure.
3.2 Oxygen Uptake Plateau
The threshold value for the V̇O2 plateau criterion
has typically been based on some arbitrary value, or
the mean change in V̇O2 per stage increment for a
research sample. The expected change in V̇O2 based
on the American College of Sports Medicine metabolic equation (V̇O2 = [10.8 • W/m] + 7) has also
been used to determine whether a V̇O2 plateau has
occurred.[32] Although the validity of these approaches is questionable,[33] we believe that this
does not exclude the V̇O2 plateau from being used
as a valid V̇O2max criterion. However, research is
required to develop new methodology for the identification of a valid and reliable V̇O2 plateau criterion.
Since there is between-subject variation in the
change in V̇O2 for any particular increase in exercise intensity,[4] the V̇O2 plateau criterion would be
valid only if it was based on the individual slope of
the V̇O2-exercise intensity relationship.[6] This approach also allows determination of the ‘total V̇O2
plateau’, which can be defined as the total deviation
from linearity of the V̇O2-exercise intensity relationship. This is in contrast to currently used V̇O2
plateau criteria that are based on the difference in
V̇O2 between only two stages or V̇O2 data points.
The major limitation of using only two V̇O2 data
points is that the determination of V̇O2 is associated
with random errors of measurement, which during
repeated measurements would scatter around the
true value.[34] This ‘noise’ in V̇O2 data may result in
the false identification of a V̇O2 plateau, and may be
particularly problematic in pseudo-ramp protocols
that are characterised by small increments in speed
or power output. Furthermore, differences in V̇O2
between stages, as the basis for the identification of
the V̇O2 plateau, is not feasible for ramp protocols.
The V̇O2 plateau criterion could be based on the
difference between the expected V̇O2 for the last
stage of the test, calculated from the V̇O2-exercise
intensity relationship and the actual value attained
during the last stage. An appropriate V̇O2 plateau
2007 Adis Data Information BV. All rights reserved.
1025
threshold value is difficult to ascertain, but should
be sufficiently stringent to indicate that the V̇O2
response has slowed enough to suggest that the
individual’s rate of oxygen transport and utilisation
was at or approaching its maximum. Future research
should investigate the validity and reliability of a
V̇O2 plateau criterion based on the individual slope
of the V̇O2-work-rate relationship, as well as identifying an appropriate plateau threshold value.
3.3 Psychological Measures
Based on current evidence, the validity of RPE
and other single-item measures of perceived effort
for evaluating the quality of a V̇O2max test, is questionable. Hutchinson and Tenenbaum[20] recommended the development and use of a more reliable and
valid multidimensional assessment that more accurately captures perceptions of effort and fatigue and
we further suggest that this approach should be
considered for the development of new V̇O2max
criteria. Such measures should take the form of
visual analogue scales, which are easy to complete
and have demonstrated good reliability and validity
in clinical and health settings.[35] In order to establish whether participants have given a maximal effort and to indicate the limiting factors to further
sustain a V̇O2max test, visual analogue scales can be
used to assess aspects such as muscular pain, determination, and overall perceived effort.[20,36] For example, a V̇O2max criterion could be based on attaining a value of at least 8 on each visual analogue
scale incorporating a range of 0–10. In addition to
evaluating the relative level of effort a subject has
given, a multidimensional approach may also provide an insight into why a subject has not given a
maximal effort. This information may prove useful
for developing strategies in the future that increase
the likelihood that a subject will give a maximum
effort during a V̇O2max test.
Lack of objectivity may be viewed as a limitation
to the development of psychological measures for
use as valid and reliable V̇O2max criteria. Appropriate anchoring labels for scale values and verbal
instructions by the researcher prior to testing[37]
should help increase objectivity. Environmental and
Sports Med 2007; 37 (12)
�1026
personal aspects may influence psychological measures and environmental variables such as distracting stimuli and the presence and behaviour of others
(including the researchers) would need to be standardised as much as possible during the development and use of psychology-based V̇O2max criteria.
In addition to multi-dimensional approaches to
measuring perceived effort during a V̇O2max test, we
believe that a subject’s willingness and perceived
ability to give a maximal effort should be assessed
immediately prior to the test. Evidence suggests that
psychological variables such as task-specific determination, perceived competence in exertion tolerance, willingness to invest effort, and physical selfefficacy greatly influence perseverance with physical exertion.[38] Not considering a subject’s psychological readiness to provide a maximum effort may
therefore be an important omission. Measurement of
psychological readiness to give a maximal effort
during a V̇O2max test could easily be achieved.
Tenenbaum et al.[38] reported an effective and simple
approach for strength and endurance tasks, with pretask questions of “how confident are you in tolerating this exertion and discomfort?” (specific selfefficacy), “how determined and committed are you
to perform the task?” (degree of commitment) and
“how much effort do you intend to put into the
task?” (effort investment). This ‘auxiliary’ information could be used to better interpret formal V̇O2max
criteria. For example, a low score on “how much
effort do you intend to put into the task?” may help
support V̇O2max criteria that indicate a subject has
given a poor effort. Additionally, such psychological readiness profiling may allow a researcher to
make an informed judgement whether to continue
with a V̇O2max test that may result in invalid physiological data, due to poor subject motivation, for
example. Psychological readiness profiling for maximal testing could be an interesting area for future
research.
4. Conclusions
The currently used V̇O2max criteria have been
heavily criticised in relation to their validity and
applicability across studies. Additionally, previous
2007 Adis Data Information BV. All rights reserved.
Midgley et al.
studies have typically used several criteria, but there
has been no agreement on how many criteria should
be used, or the proportion that need to be satisfied to
confirm the validity of the V̇O2max test results. With
this lack of standardisation, researchers may be
tempted to decide on criteria post hoc, to ensure that
no subjects have to be omitted from their study. The
above limitations considerably reduce the confidence that the subjects in an experimental study
elicited a ‘true’ V̇O2max, or that a maximum effort
was given. The credibility of V̇O2max as a robust
measure of cardiorespiratory fitness could therefore
be questioned, particularly for cross-sectional studies where comparisons between studies may be affected by differences in experimental methods, or
the subjects under investigation. This point is also
relevant for performance measures such as the peak
power output[39] or treadmill speed,[40] often associated with V̇O2max tests.
In view of the above limitations, we believe that
future research should attempt to identify a new set
of standardised V̇O2max criteria. In order to be universally applied, each criterion needs to be independent of exercise modality, test protocol and subject
characteristics. In this regard, the verification procedure and the V̇O2 plateau criterion based on the
individual slope of the V̇O2-work-rate relationship
have shown promise. We also recommend a multidimensional psychophysiological approach to
evaluating the relative degree of effort, to replace
the one-dimensional measure of the currently used
RPE scale. Psychological measures that assess the
subject’s willingness to give a maximum effort
before the test might also provide useful ‘auxiliary’
information, particularly in relation to a subject’s
readiness for maximal testing.
A major consideration for the development of a
new set of standardised V̇O2max criteria is how to
interpret the criteria when they have not all been
satisfied. In fact, how well all V̇O2max criteria agree
with each other may be a good indication of the
specificity and sensitivity[12] of the criteria in detecting whether or not an individual has elicited
V̇O2max or given a maximum effort. If all V̇O2max
criteria demonstrate a high degree of specificity and
Sports Med 2007; 37 (12)
�Maximal Oxygen Uptake Criteria
sensitivity, they should either all be satisfied, or all
not satisfied.
Howley et al.[5] suggested that published guidelines are required to promote uniformity in V̇O2max
testing procedures. We further suggest that these
guidelines, such as an American College of Sports
Medicine Position Stand, should recommend a standardised set of V̇O2max criteria. At present, however, the greatest challenge is identifying V̇O2max
criteria that remain valid across studies that are
using different test methodology and subjects.
Acknowledgements
No sources of funding were used to assist in the preparation of this article. The authors have no conflicts of interest
that are directly relevant to the content of this article.
References
1. Hill AV, Lupton H. Muscular exercise, lactic acid, and the
supply and utilization of oxygen. Q J Med 1923; 16: 135-71
2. Buchfuhrer MJ, Hansen JE, Robinson TE, et al. Optimizing the
exercise protocol for cardiopulmonary assessment. J Appl
Physiol 1983; 55: 1558-64
3. Robergs RA, Burnett AF. Methods used to process data from
indirect calorimetry and their application to V̇O2max. J Exerc
Physiol 2003; 6: 44-57
4. Taylor HL, Buskirk E, Henschel A. Maximal oxygen intake as
an objective measure of cardio-respiratory performance. J Appl Physiol 1955; 8: 73-80
5. Howley ET, Bassett Jr DR, Welch HG. Criteria for maximal
oxygen uptake: review and commentary. Med Sci Sports Exerc
1995; 27: 1292-301
6. Day JR, Rossiter HB, Coats EM, et al. The maximally attainable
V̇O2 during exercise in humans: the peak vs maximum issue. J
Appl Physiol 2003; 95: 1901-7
7. Duncan GE, Howley ET, Johnson BN. Applicability of V̇O2max
criteria: discontinuous versus continuous protocols. Med Sci
Sports Exerc 1997; 29: 273-8
8. Astrand PO. Experimental studies of physical working capacity
in relation to sex and age. Copenhagen: Ejnar Munksgaard,
1952
9. Issekutz B, Birkhead NC, Rodahl K. Use of the respiratory
quotients in assessment of aerobic work capacity. J Appl
Physiol 1962; 17: 47-50
10. Cumming GR, Borysyk LM. Criteria for maximum oxygen
uptake in men over 40 in a population survey. Med Sci Sports
1972; 4: 18-22
11. Midgley AW, McNaughton LR, Carroll S. Verification phase as
a useful tool in the determination of the maximal oxygen
uptake of runners. Appl Physiol Nutr Metab 2006; 31: 541-8
12. Stachenfeld NS, Eskenazi M, Gleim GW, et al. Predictive
accuracy of criteria used to assess maximal oxygen consumption. Am Heart J 1992; 123: 922-5
13. Meyer T, Scharhag J, Kindermann W. Peak oxygen uptake:
myth and truth about an internationally accepted reference
value. Z Kardiol 2005; 94: 255-64
2007 Adis Data Information BV. All rights reserved.
1027
14. Katch VL, Sady SS, Freedson P. Biological variability in maximum aerobic power. Med Sci Sports Exerc 1982; 14: 21-5
15. Londeree BR. Influence of age and other factors on maximal
heart rate. J Cardiac Rehabil 1984; 4: 44-9
16. Medbo JI, Sejersted OM. Acid-base and electrolyte balance
after exhausting exercise in endurance-trained and sprinttrained subjects. Acta Physiol Scand 1985; 125: 97-109
17. Meyer T, Welter JP, Scharhag J, et al. Maximal oxygen uptake
during field running does not exceed that measured during
treadmill exercise. Eur J Appl Physiol 2003; 88: 387-9
18. Hoffman RL. Effect of training at the ventilatory threshold on
the ventilatory threshold and performance in trained distance
runners. J Strength Cond Res 1999; 13: 118-23
19. Borg GA. Perceived exertion. Exerc Sport Sci Rev 1974; 2:
131-53
20. Hutchinson JC, Tenenbaum G. Perceived effort: can it be considered gestalt? Psychol Sport Exerc 2006; 7: 463-76
21. Hardy CJ, Rejeski WJ. Not what, but how one feels: the measurement of affect during exercise. J Sport Exerc Psychol
1989; 11: 304-17
22. McAuley E, Courneya KS. The subjective exercise experience
scale (SEES): development and preliminary validation. J Sport
Exerc Psychol 1994; 16: 163-77
23. Parfitt G, Markland D, Holmes C. Responses to physical exertion and psychological affect in the early stages of exercise.
Percept Mot Skills 1994; 80: 259-66
24. Rosenberg S. Objectivity in psychology and philosophy. Am
Psychol 1980; 35: 219-22
25. Burgomaster KA, Heigenhauser GJ, Gibala MJ. Effect of shortterm sprint interval training on human skeletal muscle carbohydrate metabolism during exercise and time-trial performance. J Appl Physiol 2006; 100: 2041-7
26. Basset FA, Chouinard R, Boulay MR. Training profile counts
for time-to-exhaustion performance. Can J Appl Physiol 2003;
28: 654-66
27. Thoden JS, MacDougall JD, Wilson BA. Testing aerobic power.
Ithaca (NY): Mouvement Publications Inc., 1982
28. Thoden JS. Testing aerobic power. In: MacDougall JD, Wenger
HA, Green HJ, editors. Physiological testing of the highperformance athlete. 2nd ed. Champaign (IL): Human Kinetics, 1991: 107-73
29. Rossiter HB, Kowalchuk JM, Whipp BJ. A test to establish
maximum O2 uptake despite no plateau in the O2 uptake
response to ramp incremental exercise. J Appl Physiol 2006;
100: 764-70
30. Midgley AW, McNaughton LR, Carroll S. Time at V̇O2max
during intermittent treadmill running: test protocol dependent
or methodological artefact? Int J Sports Med. Epub 2007 May
11
31. Morgan DW, Baldini FD, Martin PE, et al. Ten kilometer
performance and predicted velocity at V̇O2max among welltrained male runners. Med Sci Sports Exerc 1989; 21: 78-83
32. Wingo JE, Lafrenz AJ, Ganio MS, et al. Cardiovascular drift is
related to reduced maximal oxygen uptake during heat stress.
Med Sci Sports Exerc 2005; 37: 248-55
33. Saitoh M, Matsunaga A, Kamiya K, et al. Comparison of
cardiovascular responses between upright and recumbent cycle
ergometers in healthy young volunteers performing low-intensity exercise: assessment of reliability of the oxygen uptake
calculated by using the ACSM metabolic equation. Arch Phys
Med Rehabil 2005; 86: 1024-9
Sports Med 2007; 37 (12)
�Midgley et al.
1028
34. Wyndham CH, Strydom NB, Maritz JS, et al. Maximum oxygen
intake and maximum heart rate during strenuous work. J Appl
Physiol 1959; 14: 927-36
35. Nyenhuis DL, Stern RA, Yamamoto C, et al. Standardization
and validation of the visual analogue mood scales. Clin Neuropsychol 1997; 11: 407-15
36. Ueda T, Nabetani T, Teramoto K. Differential perceived exertion measured using a new visual analogue scale during pedaling and running. J Physiol Anthropol 2006; 25: 171-7
37. Noble BJ, Robertson RJ. Perceived exertion. Champaign (IL):
Human Kinetics, 1996
38. Tenenbaum G, Hall HK, Calcagnini N, et al. Coping with
physical exertion and negative feedback under competitive and
self-standard conditions. J Appl Soc Psychol 2001; 31:
1582-626
2007 Adis Data Information BV. All rights reserved.
39. Schabort EJ, Killian SC, St Clair Gibson A, et al. Prediction of
triathlon race time from laboratory testing in national
triathletes. Med Sci Sports Exerc 2000; 32: 844-9
40. Noakes TD, Myburgh KH, Schall R. Peak treadmill running
velocity during the V̇O2max test predicts running performance.
J Sports Sci 1990; 8: 35-45
Correspondence: Dr Adrian W. Midgley, Department of
Sport, Health and Exercise Science, University of Hull,
Cottingham Road, Hull, HU6 7RX, UK.
E-mail: A.W.Midgley@hull.ac.uk
Sports Med 2007; 37 (12)
�
 Adrian Midgley
Adrian Midgley