Group
Reports
&
&
&
&
&
&
&
&
&
&
Journal of Perinatology ( 2002 ) 22, S27 – S32 doi:10.1038/sj.jp.7210807
The participants divided into four groups on days 3 and 4 of the
workshop to discuss and prepare recommendations on the following
four areas:
Components of community-based interventions to improve
perinatal and newborn outcomes?
Appropriate study designs and key variables for studies on
community-based interventions to improve perinatal and
newborn outcomes?
Steps and factors in moving from research to implementation?
Eliciting community mobilization and focused community
participation to promote neonatal health?
&
&
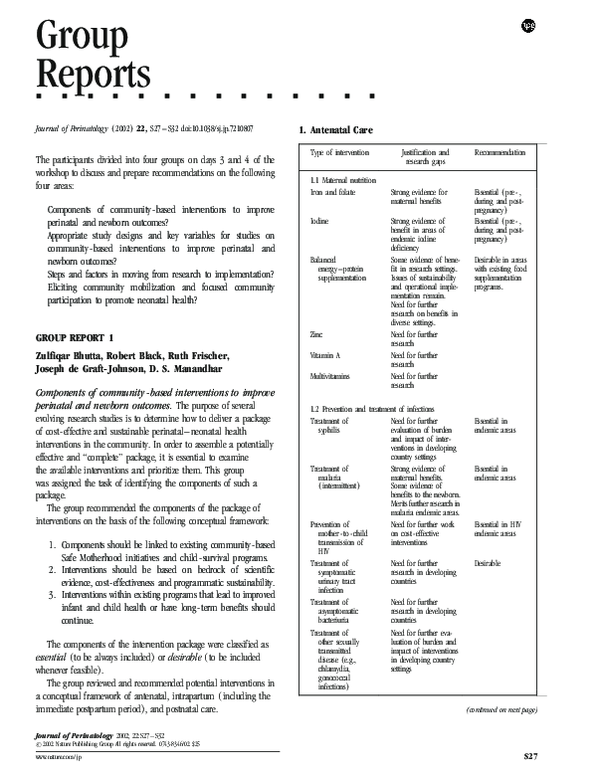
Type of intervention
1.1 Maternal nutrition
Iron and folate
Iodine
Balanced
energy – protein
supplementation
Zinc
Zulfiqar Bhutta, Robert Black, Ruth Frischer,
Joseph de Graft-Johnson, D. S. Manandhar
Vitamin A
1. Components should be linked to existing community-based
Safe Motherhood initiatives and child-survival programs.
2. Interventions should be based on bedrock of scientific
evidence, cost-effectiveness and programmatic sustainability.
3. Interventions within existing programs that lead to improved
infant and child health or have long-term benefits should
continue.
The components of the intervention package were classified as
essential (to be always included) or desirable (to be included
whenever feasible).
The group reviewed and recommended potential interventions in
a conceptual framework of antenatal, intrapartum (including the
immediate postpartum period), and postnatal care.
&
1. Antenatal Care
GROUP REPORT 1
Components of community-based interventions to improve
perinatal and newborn outcomes. The purpose of several
evolving research studies is to determine how to deliver a package
of cost-effective and sustainable perinatal–neonatal health
interventions in the community. In order to assemble a potentially
effective and ‘‘complete’’ package, it is essential to examine
the available interventions and prioritize them. This group
was assigned the task of identifying the components of such a
package.
The group recommended the components of the package of
interventions on the basis of the following conceptual framework:
&
Multivitamins
Justification and
research gaps
Recommendation
Strong evidence for
maternal benefits
Essential ( pre - ,
during and postpregnancy )
Essential ( pre - ,
during and postpregnancy )
Strong evidence of
benefit in areas of
endemic iodine
deficiency
Some evidence of benefit in research settings.
Issues of sustainability
and operational implementation remain.
Need for further
research on benefits in
diverse settings.
Need for further
research
Need for further
research
Need for further
research
1.2 Prevention and treatment of infections
Treatment of
Need for further
syphilis
evaluation of burden
and impact of interventions in developing
country settings
Strong evidence of
Treatment of
malaria
maternal benefits.
( intermittent )
Some evidence of
benefits to the newborn.
Merits further research in
malaria endemic areas.
Need for further work
Prevention of
on cost - effective
mother - to - child
interventions
transmission of
HIV
Need for further
Treatment of
research in developing
symptomatic
countries
urinary tract
infection
Treatment of
Need for further
asymptomatic
research in developing
bacteriuria
countries
Need for further evaTreatment of
luation of burden and
other sexually
impact of interventions
transmitted
in developing country
disease ( e.g.,
settings
chlamydia,
gonococcal
infections )
Desirable in areas
with existing food
supplementation
programs.
Essential in
endemic areas
Essential in
endemic areas
Essential in HIV
endemic areas
Desirable
(continued on next page)
Journal of Perinatology 2002; 22:S27 – S32
# 2002 Nature Publishing Group All rights reserved. 0743-8346/02 $25
www.nature.com / jp
S27
�Group Reports
(continued )
Type of intervention
Detection and
treatment of
bacterial
vaginosis
1.3 Behavioral issues
Birth preparedness
Education
into seeking
antenatal care
Counseling
on benefits
of exclusive
breastfeeding
Improved nutrition
in pregnancy
Recognition of
danger signs
for seeking
emergency
obstetric care
Education on
high risk
pregnancies,
e.g., previous
stillbirths or
perinatal deaths
(continued )
Justification and
research gaps
Recommendation
Need for further
research
Cord cutting and care
Essential
Essential
Essential
Essential
Training of the birth
attendant and families in recognition
of birth complications
that impact on newborn health and require speedy referral,
e.g., malpresentation,
prolonged labor,
eclampsia, antepartum hemorrhage,
cord prolapse
Hand - washing by birth
attendant, clean
surface
Care of the baby during
the delivery of the
placenta
� Drying and wrapping the baby
� Placing the baby on
the mother’s abdomen or to the breast
S28
Use of clean disposable blade
� Use of clean tie
� Clean cord and
leave uncovered
Basic resuscitation
including:
Justification and
research gaps
Recommendation
Further operational
research is needed to
assess the utilization of
safe birth kits versus
other approaches, and
the impact of cord
antisepsis on neonatal
outcomes
Essential
Need for further
operational research,
especially at the
domiciliary and
community level
Essential
Need for behavioral
and operational
research
Proven benefits
Essential
�
Essential
Tactile stimulation
Positioning
� Mouth - to - mouth
or bag - mask
resuscitation
Avoidance of inappro priate oxytocic use
�
�
Need for further
research on benefits
for perinatal / newborn
outcomes
Desirable
Immediate breast feeding
2. Intrapartum Care and Immediate Postpartum Care
The group underscored the importance and the need for skilled
health care at birth, but recognized that the nature of individuals
providing this care would differ according to health systems and
countries. The emphasis should be on the requisite skills necessary
for safe birth in domiciliary settings.
Type of intervention
Type of intervention
Justification and
research gaps
Recommendation
Well - known complications that impact on
fetal – neonatal survival
Essential
Essential
Need for research on the
optimal timing of cord
cutting in relation to
placental delivery
Essential
Essential
3. Postnatal Care
Type of intervention
Keeping the baby warm
� Delay bathing by
6 hours or more
� Kangaroo Mother Care
� Swaddling
� Co - bedding
� Warm room
Weighing the baby
Exclusive breast - feeding
Cup and spoon feeding of
expressed breast milk
for low birth weight
infants
Hygiene and skin care
Eye care
Justification and
research gaps
Recommendation
Need for operational
research
Essential
Need for research on
alternative methods
( e.g., anthropometry )
to identify low birth
weight babies
Proven benefits
Well - established
benefits
Desirable
Need for formative
and operational
research
Proven benefit
Essential
Essential
Essential
Essential in
endemic areas
Journal of Perinatology 2002; 22:S27 – S32
�Group Reports
(continued )
Type of intervention
Education of families
and caregivers for
recognition of danger
signs on care seeking
and referral of a sick
newborn
Education of families and
caregivers in recognition of danger signs for
neonatal sepsis and
care seeking / referral /
treatment
Treatment of
neonatal sepsis
Justification and
research gaps
Need for further research
into use of a clinical
algorithm to identify
sick newborns, domiciliary management of
the sick newborn, if
referral not possible.
Operational research
also needed on how to
overcome barriers to
identify sick newborns
and how to promote
effective referral
pathways
Need for research to
validate criteria of sepsis
in diverse settings.
Need for research on
microbiology of organisms causing sepsis
Several possibilities exist
for treatment of sepsis
Selection of antibiotics
should be based on
microbiology of organisms, national drug
policy, cost effectiveness
and feasibility of delivery. Need for research
into different approaches
for treating neonates
with sepsis in the community, including domiciliary management.
Recommendation
Essential
Essential
Key Outcome Indicators
The choice of outcome indicators depends on the duration
and size of the study. These two factors affect the likelihood of
achieving changes in outcome indicators such as neonatal mortality
rate. The indicators that are expected to change due to intervention
should be specified at the outset. If a process indicator is used as an
outcome, it should also be used in the estimation of sample size.
For studies on community-based interventions to improve perinatal and neonatal health, the following indicators were recommended:
Essential
Note: The group highlighted the need to consider approaches to
domiciliary management of the newborn in the context of the health
system. Thus, it is important to emphasize the need to strengthen
referral pathways, improve quality of care at the primary and
secondary referral centers, and ensure linkage with maternal
postnatal care.
GROUP REPORT 2
Saadet Arsan, Paul Arthur, Abdullah Baqui,
Simon Cousens, Ashok Deorari, Shams El Arifeen, David
Osrin, Izaz Rasul, Indira Narayanan
Appropriate study designs and key variables for studies on
community-based interventions to improve perinatal and
neonatal outcomes. In order to maximize the gains from different
studies, it is essential to have standardized design and methodology.
Only then can the results be compared and, possibly, pooled. There
should be an agreement on key outcome variables and date
collection methods: This group addressed these key issues.
Journal of Perinatology 2002; 22:S27 – S32
Study Design
The optimal study design to demonstrate the impact of an
intervention on a behavior or a health outcome is the randomized
controlled trial. Current knowledge about community care of
neonates is not at a stage where intervention packages can be taken
to trial without the need for randomization and controls. The use of
controls raises ethical and design issues. One way to address these
concerns is to introduce interventions in a stepwise fashion.
The packages of interventions should be examined for effectiveness, while individual interventions need to be tested for efficacy.
� Essential: Neonatal mortality rate
� Desirable: Perinatal mortality rate, stillbirth rate, early
neonatal mortality rate, late neonatal mortality rate, fresh
stillbirths plus neonatal mortality rate.
It was recommended that cost be estimated, as it is essential
descriptive information in these studies.
Depending on the scope of the study and the precision of the
evaluation tools employed, the following additional information may
be gathered:
Maternal morbidity
Fresh stillbirth/all stillbirths
Cause-specific neonatal mortality
Birth weight (or surrogates)
Proportion of low birth weight infants
Birth-weight-specific mortality
Proportion of preterm infants
Incidence of neonatal morbidities, especially birth asphyxia
and sepsis
� Delivery sites, skilled or unskilled care at birth
� Choice and use of providers, utilization of health system
resources
�
�
�
�
�
�
�
�
Process Indicators
One or more process indicators could be used as outcome variables.
Generating information on practices is more important than
information on knowledge; and observation or demonstration of
activities is preferable to reporting or recall of activities.
Qualitative assessment must be an integral part of the studies as
ethnographic investigation may yield extremely useful information
for the program.
S29
�Group Reports
The specific process indicators recommended were skilled health
care at birth, immediate care at birth, thermal control, clean
practices at birth, resuscitation, cord care, early initiation and
exclusivity of breast-feeding, eye care, immunization, recognition of
danger signs, care seeking, and postnatal care by a skilled provider.
Many of these indicators need further definition and validation.
Considerations in Data Collection
Data collection may be continuous or periodic. Both have their
advantages and disadvantages. A decision needs to be taken
beforehand whether specific information will be collected from the
control group or not. The process of data collection may affect the
outcomes in the control population. The greater the quantum of
process information collected, the higher the cost of the study and the
more intense the effect on the control group. One way to neutralize
this effect is to exclude informants from subsequent periodic
assessments. As far as possible, studies should develop their own
evaluation system and not rely on routinely collected data.
Studies need to take into consideration the issues of loss to followup, variable exposure to intervention, dispersion or congruity of
intervention and control areas, intra- and intercluster movement,
and problems of emigration or temporary movement of subjects. All
providers within the community should be enumerated.
Standard and accepted definitions and tools should be used. The
studies may address the development of additional necessary tools as
a part of their activities.
GROUP REPORT 3
Elaine Albernaz, Abhay Bang, Gary Darmstadt,
Judith Moore, N. C. Saxena, Uzma Syed
Moving from research to implementation. The ultimate aim of
action research is to develop interventions for incorporation into
health programs. However, all community-based research does not
necessarily lead to program-ready interventions and approaches.
This group was assigned the task of defining the attributes of
interventions that make them amenable to implementation in the
program setting and the steps required to achieve that.
Criteria
The decision to move from research to implementation depends on
several considerations:
1. Is the problem of sufficient magnitude and/or severity in
the population to take up the intervention on a
programmatic scale?
The importance of a given health problem varies from country
to country. There is no universal threshold of neonatal mortality
rate at which a program targeted to newborn infants needs to be
initiated. Each country should set national goals for neonatal
health indicators.
S30
2. Is the intervention effective?
The intervention should have been demonstrated as effective
under field conditions in more than one site and under more than
one set of conditions. There is often a need for an intermediate step of
effectiveness studies between the initial efficacy trial and
implementation. The intervention should potentially be able to
address the problem on a national level. The acceptable level of
impact depends on many factors such as the cost, the ease of
implementation and potential for adverse effects.
3. Is the intervention cost-effective?
The intervention should be cost-effective and affordable by the
country.
4. Is the intervention acceptable?
It is essential to ensure the acceptability of the intervention among
decision makers, professional leaders, health workers and the
community.
5. Is the intervention sustainable?
Sustainability is a fundamental issue in community programs.
Embarking on a program that cannot be sustained in the long
run does more harm than good to the cause. Vertical programs
may be more easily scaled up than an integrated, multicomponent
program, but sustainability may be compromised.
6. Is there an ethical urgency?
There is a threshold beyond which it is unethical to withhold an
intervention from the community that has impact and only a limited
chance of causing adverse effects.
Steps
After the above criteria regarding the intervention are met, the
following steps are required in order to effectively implement the
intervention in a program:
� Build consensus among political leaders and other
stakeholders that implementation of the intervention is
essential. Generating political will and momentum may be a
major bottleneck to the launch of a program. Therefore,
there is a need to take along all the stakeholders including
national and regional policy makers, professional groups,
human rights groups, women’s groups and the media.
Opinion makers who are likely to oppose the program
should be included in deliberations from the beginning.
� Select the implementing agency, which could be a
department within the government, private sector, or an
NGO, or a combination of these.
� Constitute a group that adapts the intervention to national or
regional circumstances. It is possible that some elements of
the package are dropped or modified.
� Prepare a blueprint for implementation of the intervention,
taking into account the burden of the problem, perceived
community demand for the intervention, resource needs,
health system strengths/weaknesses, private sector/community assets and available tools.
Journal of Perinatology 2002; 22:S27 – S32
�Group Reports
� Start the phase-wise implementation of the program. Initial
communities should be selected carefully to provide for a fair
chance of success of the program.
� Monitor and evaluate the program. There is a need to
regulate the implementation of the program to ensure that
the program improves over time. Aspects of the package may
lose relevance over time as the magnitude of the target
problem(s) changes, requiring fine-tuning of the program.
The above process will need to be repeated at the local level
to make microlevel adjustments.
health because infants are often born at home and the care of
newborns in developing countries is often conditioned by traditional
beliefs, practices, and behaviors that may require change for
improved outcomes. The deliberations of this group were focused on
the need, principles, and methodology of community mobilization.
Why Community Mobilization and Participation
� Focus of the program is on the infants of the community;
hence, its involvement is a moral and ethical obligation.
� Newborn essential care packages consist primarily of
GROUP REPORT 4
Nabeela Ali, Anthony Costello, Lisa Howard-Grabman,
Vinod K. Paul, Jose Martines
Eliciting community mobilization and focused community
participation to promote neonatal health. Community
acceptance and participation in health care programs is a
fundamental prerequisite for its sustainability and success.
Investigators engaged in community-based research aimed to be
translated into programs must build in a component of community
mobilization from the outset. This is particularly so for neonatal
�
�
�
�
behavior change, requiring changes in individual, family,
and community behaviors and norms.
Success of community-based interventions depends on
community acceptance of the interventions.
Involvement of communities in research planning, implementation of interventions and evaluation can help to reduce
lag time for implementation, upscaling, and expansion.
Communities can contribute resources that may not be
available to the health system alone.
Community involvement in monitoring and evaluation
provides community perspective on quality of care,
appropriateness, and feasibility of interventions.
Figure 15. The community action cycle for community mobilization (Courtesy, Lisa Howard-Graham ).
Journal of Perinatology 2002; 22:S27 – S32
S31
�Group Reports
� Community participation breaks barriers to implementation,
� Consider issues of coverage of all strata including those most
helps program teams to troubleshoot, and develop practical
solutions.
� Outcomes of community participation go beyond health to
include self-efficacy and collective efficacy, and strengthened
community capacity to identify priorities and address them.
� Community participation is the key to long-term sustainability of program interventions and outcomes.
affected by the problem with emphasis on marginalized or
disadvantaged groups.
Ensure appropriate involvement of ‘‘gatekeepers,’’ opinion
leaders, and decision makers (including private practitioners).
Develop strategies to ensure continuing community interest
in the initiative (e.g., identifying successes and celebrating
them).
Ensure that the team has a clear understanding of economic,
social, political, and cultural context.
Work in accordance with the community calendars and
schedules.
Make the program management culture as participatory and
open to supporting new approaches. Do not punish team
members for mistakes; learn from them.
Keep focused on the program goal; put a monitoring system
in place with community review of findings.
Ensure adequate contact with the community to maintain
desired level of action.
Determine your program policy and philosophy with regard
to incentives for community participation in the context of
long-term sustainability of the program and not for shortterm gains.
�
�
�
Some Basic Principles of Community Participation/
Mobilization
� Set specific goals around which to mobilize the community.
� Define your community (it could be just a ‘‘core group,’’ or
�
�
supporting groups and individuals, or a broader community).
� Be apolitical. Do not indulge in local politics.
� Be transparent and honest; explain the goals of the program
�
to the community and share what you can do and what you
cannot do.
Respect community values and concerns as well as
hierarchies and culture.
Define and redefine your role in relation to communities as
they strengthen their capacity in order to encourage growing
autonomy.
If you do not know why something is happening, ask
community members.
Be flexible. Not all communities are the same and not all
groups within communities are the same.
Define process objectives for community mobilization related
to underlying themes that contribute to the health problem
(e.g., exploring the value of newborns’ and mothers’ lives,
gender equity, shared responsibility for quality care).
Draw upon successful models in similar situations.
�
�
�
�
�
�
�
Community Action Cycle
Community action cycle describes the steps in community
mobilization. It consists of the following sequence of activities:
prepare to mobilize, organize community for action, explore the
health issues and set priorities, plan together, act together, evaluate
together and scale up. Figure 15 depicts the details of these steps.
�
Issues in Scaling Up
� The methodology needs to be affordable and feasible in order
to be scaled up.
� Consensus should be built around adopting a particular
model/approach.
� Partnerships are essential to achieve larger scale impact and
it is crucial to define goals of the partnership and program,
roles and responsibilities, coordination mechanisms, and
indicators of success/performance.
� Partners in scaling up could be social scientists, NGOs,
government, communities, private sector, economists, and
other technical specialists.
� Advocacy with the leaders is required to ensure acceptance of
the scaling-up initiative.
Gaps
Issues in Implementation of a Community Mobilization
Effort
� There are only a few examples of scaling-up experiences and
� Ensure that design is feasible and affordable on a large scale.
� Develop capacity of facilitators for community mobilization
community participation programs at different scales and in
different settings.
� Only a limited experience is documented on the impact of
community participation approaches combined with communication strategies such as social marketing, mass media,
and interpersonal communication and counseling.
� While estimating cost-effectiveness, the investigators often
overlook gains in community capacity as a part of the
broader benefit to the program.
through a combination of training and field experience.
(This is a technical discipline with a defined set of skills.)
� Foster community acceptance of the project and its team at
the outset.
� Build on other existing programs and activities in the
community.
� Build on prevalent positive practices in the community.
S32
approaches to scaling up in community mobilization.
� There is a paucity of research on impact evaluation of
Journal of Perinatology 2002; 22:S27 – S32
�
 Ruth Frischer
Ruth Frischer