C 2006)
Neuropsychology Review, Vol. 16, No. 1, March 2006 (�
DOI: 10.1007/s11065-006-9001-y
Understanding Obsessive–Compulsive Disorder:
Focus on Decision Making
Paolo Cavedini,1,3 Alessandra Gorini,1,2 and Laura Bellodi1
Published online: 18 May 2006
Current approaches to obsessive-compulsive disorder (OCD) have suggested that neurobiological
abnormalities play a crucial role in the etiology and course of this psychiatric illness. In particular,
a fronto-subcortical circuit, including the orbitofrontal cortex, basal ganglia and thalamus appears to
be involved in the expression of OCD symptoms. Neuropsychological studies have also shown that
patients with OCD show deficits in cognitive abilities that are strictly linked to the functioning of
the frontal lobe and its related fronto-subcortical structures, such as executive functioning deficits
and insufficient cognitive-behavioral flexibility. This article focuses on decision making, an executive
ability that plays a crucial role in many real-life situations, whereby individuals choose between
pursuing strategies of action that involve only immediate reward and others based on long-term
reward. Although the role of decision-making deficits in the evolution of OCD requires further
research, the collected findings have significant implications for understanding the clinical and
behavioral heterogeneity that characterizes individuals with OCD.
KEY WORDS: decision-making; executive functions; gambling task; obsessive–compulsive disorder; reward.
Obsessive–compulsive disorder (OCD) is characterized by the presence of recurrent unwanted thoughts
(obsessions) that increase subjects’ anxiety, often accompanied by persistent and distressing ritualized acts (compulsions) that decrease the anxiety (American Psychiatric
Association, 2000). These symptoms represent a severe
disabling condition and significantly interfere with the
patient’s daily life. The importance of better understanding psychological and neural mechanisms involved in
this disorder is justified by the fact that, at present,
OCD is the fourth most common psychiatric disorder
(El-Sayegh et al., 2003) and is considered one of the
most disabling medical conditions (Murray and Lopez,
1996), with a progressively increasing need for effective
intervention strategies.
Current approaches to OCD suggest that neurobiological abnormalities play a crucial role in its etiology
and course and provide biological models based on direct and indirect investigations of the possible brain circuits involved in the expression of obsessive–compulsive
symptoms. In particular, both direct observations, usually
performed via neuroimaging techniques (Baxter et al.,
1987; Kim et al., 2001; Perani et al., 1995; Swedo et al.,
1989;), and indirect observations from a variety of neuropsychological studies (see Greisberg and McKay, 2003
for a review), provide growing evidence for involvement
of a fronto-subcortical circuit, including orbitofrontal cortex (OFC), basal ganglia, and thalamus, in the expression
of OCD.
From a neuropsychological aspect, the integrity of
this orbitofrontal–striatal–thalamic–orbitofrontal loop is
believed to be specifically related to the cognitive functions termed executive, which are the higher-level mental
processes that modulate sensory, motor, cognitive, memory, and affective abilities (Chamberlain et al., 2005).
Through executive functions we plan future actions,
1 San
Raffaele Scientific Institute, Department of Neuropsychiatric Sciences, Universitá Vita-Salute San Raffaele, Faculty of Psychology,
Milan, Italy.
2 Maastricht University, Department of Psychiatry and Neuropsychology,
Maastricht, The Netherlands.
3 To whom correspondence should be addressed at San Raffaele Hospital
Scientific Institute, Department of Neuropsychiatric Sciences, Universitá Vita-Salute San Raffaele, Faculty of Psychology, 20, Via Stamira
D’Aneona 20127, Milan, Italy; e-mail: cavedini.paolo@hsr.it.
3
C 2006 Springer Science+Business Media, Inc.
1040-7308/06/0300-0003/0 �
�4
monitor our behavior, and alter it in response to specific
feedback and changes in environmental contingencies.
Thus, executive functions depend on the intact functioning of many of the more fundamental cognitive operations,
such as memory and attention.
A relevant cognitive skill linked to the executive
functions is decision-making, the ability to process environmental information in order to make advantageous
decisions. Studies on neurological patients (Bechara et al.,
1996; Damasio, 1994) have shown that the ability to make
helpful real-life decisions, involving choices between actions leading to uncertain outcomes and the ability to calibrate between rewards and punishments, depends on the
integrity of the orbitofrontal cortex and its interconnected
circuits, which are some of the same structures assumed
to be involved in the pathogenesis of OCD.
This article presents a critical review of the available data on the neuropsychological aspects of decisionmaking in OCD, as well as subjects’ perceptions of reward
and punishment. Analysis of this cognitive ability could
help us to better understand OCD behavior, dissecting
the observed clinical and behavioral heterogeneity in the
many ways in which this disorder is expressed. We also
discuss the decision-making deficit in relation to anatomical correlates and emphasize the use of neurocognitive
criteria for subtyping OCD, which can serve as a guide
for development of more specific, and potentially more
successful, behavioral and pharmacological interventions.
AN OVERVIEW OF NEUROBIOLOGICAL
MODELS OF OBSESSIVE–COMPULSIVE
DISORDER
In the last few decades, many investigators have contributed to the hypothesis that OCD involves dysfunctions
in a neuronal loop extending from the orbitofrontal cortex and cingulate gyrus to the striatum (caudate nucleus
and putamen), globus pallidus, thalamus, and back to
the frontal cortex (Saxena et al., 1998; Szeszko et al.,
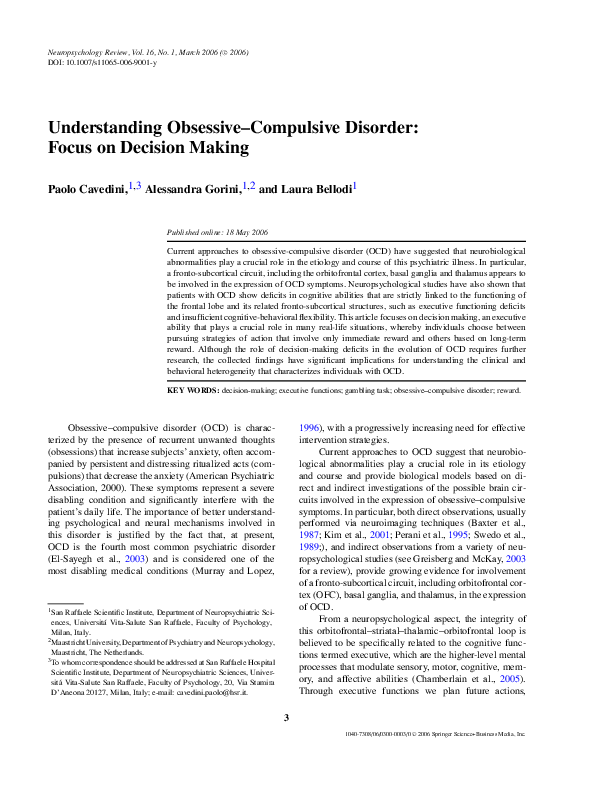
2004) (Fig. 1). Neuroimaging studies have shown that in
OCD patients activity within this cortico–basal ganglia
network is increased at rest (Machlin et al., 1991; Swedo
et al., 1989), accentuated during provocation of symptoms
(Hollander et al., 1995; Mataix-Cols et al., 2004; Rauch
et al., 1994), and attenuated after successful treatment
(Baxter et al., 1992; Rubin et al., 1995; Saxena et al.,
1999).
Both empirical and theoretical studies have shown
that the orbitofrontal cortex (OFC), posited to lie within
the basal ganglia-cortico-thalamic circuit, is strictly implicated in the pathophysiology of OCD. This theory is
P. Cavedini, A. Gorini, and L. Bellodi
Fig. 1. Orbitofrontal striato–thalamo–orbitofrontal loop involved in
the pathogenesis of OCD: there are two antagonistic pathways through
which the striatum influences the globus pallidus internus/substantia
nigra (GPi/SNr) output nuclei. The most well studied of these is the
direct striatal-GPi/SNr pathway that inhibits the GPi/SNr output nuclei,
and thus causes a disinhibition of the thalamus. This direct striatalGPi/SNr pathway is counterbalanced by an indirect pathway from the
striatum to the GPi and SNr that acts to oppose the disinhibition of
the thalamus. By maintaining a balance between the direct and indirect
pathways, the basal ganglia regulates the excitability of the thalamus and
determines what information should be passed to the cortical processing
areas.
supported by neurophysiological (Bannon et al., 2002; Di
Russo et al., 2000; Leocani et al., 2001), neuroradiological
(Jenike et al., 1996; Kim et al., 2001; Scarone et al., 1992;
Stein et al., 1993), and metabolic (Baxter et al., 1987;
Benkelfat et al., 1990; Perani et al., 1995) studies that
have reported a relationship between OCD and brain circuits that are posited to connect the frontal cortex to basal
ganglia structures in the physiological model proposed by
Alexander (1986).
From a biochemical aspect, it has been observed that
the serotonin and the dopamine systems could be especially important in mediation of OCD symptoms (Denys
et al., 2004; Pogarell et al., 2003; Simpson et al., 2003).
In fact, while standardized treatments with selective serotonin reuptake inhibitors in OCD are associated with significant reductions in OFC metabolism, the administration
of dopamine agonists leads to stereotypic behavior and
exacerbates OCD symptoms.
Finally, clinical and behavioral researchers have
shown that typical clinical features of OCD are present
in both humans and nonhumans with lesions in the frontal
lobes and basal ganglia (Pitman, 1982; Rapoport and
Wise, 1988).
Contribution of Neuropsychology
to Understanding OCD
Specific neuropsychological tests have confirmed the
role of the fronto–cortico–subcortical circuit in OCD. For
�Decision-Making in Obsessive–Compulsive Disorder
example, the Tower of Hanoi, the Wisconsin Card Sorting
Test, and the Object Alternation Test, have been used to
investigate the functioning of different brain areas on the
basis of localizatory hypothesis. In particular, OCD patients show a significantly poor performance in the Tower
of Hanoi task, which seems to be sensitive to frontostriatal
circuits and basal ganglia damage (Cavedini et al., 2001;
Mataix-Cols et al., 1999) and in the Object Alternation
Test, which is sensitive to a malfunctioning of the OFC
(Abbruzzese et al., 1995a; Cavedini et al., 1998; GrossIsseroff et al., 1996).
Although the findings are contradictory (Lacerda
et al., 2003), the prevailing empirical evidence appears
to support the notion that OCD patients show normal
performance on the Wisconsin Card Sorting Test, that is
specifically related to the correct functioning of the dorsolateral prefrontal cortex, which is not directly implicated
in OCD (Abbruzzese et al., 1995b; Cavallaro et al., 2003).
Neuroimaging and neuropsychology are complementary
disciplines that provide powerful means for assessing the
structure and function of cortico-striatal circuits. Two
studies (Kwon et al., 2003; Lacerda et al., 2003) combined neuropsychological functioning of OCD patients
with their brain structural abnormalities and metabolic
activity. Correlations between volumetric abnormalities
and metabolic rates, and neuropsychological performance
were found in the prefrontal cortex and subcortical structures (globus pallidus, anterior cingulate gyrus, and putamen) only in the OCD group.
Impaired activation of basal ganglia was also found
by Fernandez and colleagues (Fernandez et al., 2003) who
evaluated changes in cerebral blood flow in OCD and control subjects during the Tower of Hanoi test. This study
supports the supposed modification of the activating systems of basal ganglia functions in OCD compared with
normal subjects. Using the same test, van den Heuvel et al.
(2005) showed a decreased frontal-striatal responsiveness
during planning in OCD patients. These findings support
the hypothesis that decreased prefrontal-striatal responsiveness is associated with impaired planning ability in
OCD patients. Since the described frontal-striatal dysfunction in OCD is independent from state anxiety and
disease symptom severity, they concluded that executive
impairment is a core feature in OCD.
THE ORBITOFRONTAL CORTEX AND
REWARD PERCEPTION
When a malfunctioning of the OFC occurs, subjects
show specific deficits in the perception of reward and
lose the ability to make advantageous decisions in many
5
real-life situations, even if their other cognitive functions
appear intact.
Studies on animals (Mora and Cobo, 1990; Mora
et al., 1979; Nakano et al., 1984; Phillips et al., 1979;)
and humans (Tataranni et al., 1999) have shown that OFC
and the ventromedial prefrontal regions are implicated
in different aspects of reward mechanisms, and now it
seems clear that one of the functions of the OFC is the
association between reward and behavior (Rolls, 2000). It
has also been observed that OFC cells fire in response to
any kind of stimulus whenever the stimulus is presented
as a reinforcer. The OFC reward-related processes work
with far greater sensitivity than other structures of frontal
cortex (i.e., the ventral striatum) do and are responsible
for coding “satiety,” which consists of a reduction in the
motivational value of stimuli after prolonged exposure.
Failure of this process leads to prolonged exposure to
reinforcers.
Perception of Reward in Obsessive–Compulsive
Patients
Clinical observations of OCD patients reveal some
pathological behaviors strictly connected to unadaptive
perception of reward. For example, while in a nonpathological condition the normal desire to wash the hands
after touching a dirty object disappears after the hands
are washed, compulsive washers never perceive “satiety” and continue to feel forced to wash themselves humans (Phillips et al., 2000). At the same time, acting
on compulsions (negative reinforcement), they obtain a
temporary relief of anxiety (reward) but never feel “full”.
Through similar mechanisms, other patients use avoidance behaviours to avoid contact with anxiety-provoking
stimuli and situations. Again, avoidance produces a decrease of subjective anxiety, becoming a sort of reward
(Fig. 2).
In this perspective, compulsive behaviors and obsessive thoughts often appear to completely disrupt planning
of real-life strategies. A life quality compromised, despite a normal cognitive functioning and normal abilities
in problem solving tasks, associates OCD patients with
neurological patients with lesions to the OFC who develop a severe impairment in real-life decision-making.
The extensive literature on ventromedial patients shows
that they often pursue actions that bring some reward in
the immediate future, in spite of severe long-term negative consequences such as the loss of job, home, and
family. These patients show deficits in executive functions and insufficient flexibility in cognitive–behavioral
aspects, which make them oblivious to the future
�6
P. Cavedini, A. Gorini, and L. Bellodi
Fig. 2. The OCD behavioral loop. The appearance of obsessions causes an increase of anxiety that would
spontaneously decrease in time and can be compared to a short-term penalty. The pathways of behavior that OCD
patients follow can be avoidance or acting on compulsions. Both give an immediate reward in terms of anxiety
decrease, but greatly impair the patient’s daily life, representing a long-term penalty. Moreover, compulsions
reinforce obsessive thoughts, perpetuating the obsessive–compulsive mechanism and representing a long-term
penalty.
consequences of their actions (Bechara et al., 1994, 1996,
2000). They pay attention only to their immediate reward
and seem to be unable to modulate their next decisions at
the light of previous errors. In other words, despite normal intellect, ventromedial patients show abnormalities in
decision-making together with abnormalities in emotion
and feeling.
Similarities with OCD behavior are clear: lack of
behavioral flexibility (continuous repetition of the same
behavior), search for an immediate reward (relief of anxiety from compulsions), and blindness to negative future
consequences (compromised life-quality) are also characteristic traits of OCD patients.
A NEUROPSYCHOLOGICAL APPROACH
TO THE STUDY OF DECISION MAKING
Different neuropsychological tests have been proposed for laboratory investigations of functional and
anatomical substrates of decision making. They have been
theoretically distinguished on the basis of how they operationalize the processes involved in decision making
(Bechara et al., 1999). Perhaps some of them are based on
the concept of delay, and others on the notion of risk.
Delay-based tasks require subjects to choose between
small, immediate rewards or larger, delayed rewards and
the optimal choice is to choose delayed rewards. Otherwise, risk-based tasks contain elements of uncertainty,
and in order to succeed participants must adopt a preference for small but certain rewards over larger, uncertain
rewards. These latter tasks are classified as probabilistic
or risk-taking tasks.
The Gambling Task
Here, we consider only the risk-based tasks and, in
particular, we will focus our attention on the very well
known Gambling Task (GT), a card game that detects and
measures decision-making impairment, testing the subject’s ability to balance immediate rewards against longterm negative consequences. This test was initially developed by Damasio et al. (Bechara et al., 1994) to assess the
“myopia for the future” in ventromedial patients because,
as in real life, the task offers them choices that may be
risky, without any obvious explanation of how, when, or
what to choose. In other words, the task resembles realworld contingencies in which we are frequently exposed
to ambiguous situations that do not permit an exact calculation of future outcomes and in which choices must often
be based on approximations and guesses. In particular, the
task assesses the ability of subjects to acquire a preference
through rewards and punishments as represented by gains
and losses of play money.
Briefly stated, the GT requires 100 card selections
from four decks of cards identical in appearance; subjects are asked to maximize their profit starting from a
$2000 loan of play money. To attain this goal they must
find the most advantageous decks and persistently pick up
cards from those decks. After turning over some cards,
subjects are both given money and sometimes asked to
�Decision-Making in Obsessive–Compulsive Disorder
pay a penalty according to a pre-programmed schedule
of reward and punishment. Gains and losses are different
for each card selected from the four decks: decks A and
B are “disadvantageous,” as, though they pay $100, the
penalty amounts are higher, so they cost more in the long
run; decks C and D are “advantageous” because they pay
only $50, but the penalty amounts are lower resulting in
an overall gain in the long run. In summary, decks A and
B are equivalent in terms of overall net loss over the trials,
as are decks C and D; the difference is that in decks A and
C the penalty is more frequent, but of smaller magnitude,
while in decks B and D the penalty is less frequent but of
larger magnitude.
Several studies suggest that the performance at the
GT evaluates the decision-making function mediated by
a ventromedial prefrontal cortex (Bechara et al., 1998;
Grant et al., 2000). In fact, only patients with damage to
the ventromedial, but not to the dorsolateral or dorsomedial sectors of the prefrontal cortex, persist in drawing
cards from the high payout/high penalty decks despite the
ultimately punishing consequences of this behavior.
DECISION-MAKING DEFICIT IN
PSYCHIATRIC CONDITIONS
The experimental strategies used to study decision
making in neurological patients provide parallels and
direct implications for understanding the neurobiological mechanisms of several neuropsychiatric disorders
(Table 1).
In fact, using the GT, many studies have demonstrated similar decision-making impairments in cocaine,
opiate, and alcohol abusers (Bechara et al., 2001a; Grant
et al., 2000; Rogers et al., 1999), who have shown abnormalities in the ventromedial prefrontal cortex during
functional neuroimaging studies (Hommer et al., 1997;
Volkow et al., 1991). Following the line of research that
suggests a possible link between addictive and compulsive
behavior (Volkow and Fowler, 2000) and the previously
discussed evidence of an important involvement of the
brain circuits connecting the frontal cortex to basal ganglia structures in the pathophysiology of OCD, the GT
has also been proposed as a good tool to assess decisionmaking impairment in OCD.
Study of Decision Making in OCD
Starting from these considerations, Cavedini et al.
(2002a) investigated decision-making abilities in OCD
compared to panic disorder patients and healthy control
7
subjects. OCD and panic groups were compared to examine whether the expected poor performance in the GT was
unique to OCD or whether it was also present in other
related anxiety disorders, although there are notable clinical and cognitive differences between these two pathologies. As expected, the results showed different decisionmaking performance between OCD and panic patients. In
fact, the OCD subjects showed a significant preference
for the disadvantageous decks, while panic and control
subjects made significantly more selections from the advantageous decks, avoiding the bad decks. Analysis of the
100 card selections demonstrated that control subjects and
patients with panic disorder started from random choices
and gradually shifted their preferences toward the “good”
decks during the test. By contrast, OCD patients failed
to operate this shift in card selection: they rapidly shifted
their preferences toward the “bad” decks, encouraged only
by the prospect of immediate gain. Analysis of strategies
adopted by OCD patients from the beginning to the end
of the test suggested that during the 100 selections, all
subjects understood the differences that characterize the
four decks but, while control subjects and panic patients
increased the number of advantageous choices, OCD patients deliberately increased the number of disadvantageous selections (Fig. 3). OCD patients appeared to be
encouraged greatly by the prospect of immediate reward,
being less sensitive to the future consequence of their
choices.
Another study (Cavallaro et al., 2003) used the GT to
confirm the hypothesis of a double dissociation between
different frontal lobe dysfunction in schizophrenic versus
OCD patients. They found, as expected, that OCD individuals performed significantly worse at the GT than
schizophrenic patients, confirming a specific involvement of the ventromedial cortex in OCD (Saxena et al.,
1998) not present in the latter, in which the principal
compromised part of the frontal lobe is the dorsolateral prefrontal cortex. Similar results were obtained by
Wilder et al. (1998) who did not find any difference
in GT performance between schizophrenic patients and
controls.
Is Decision-Making Impairment in OCD a Trait
Condition or an Anxiety-Induced Characteristic?
The decision-making impairment observed in OCD
patients seems to be a trait condition instead of an anxietyinduced characteristic. To confirm this hypothesis,
Cavedini et al. (2000) compared the decision-making
performance in OCD and depressed patients, who report
some degree of mental ruminations similar to thoughts or
�8
P. Cavedini, A. Gorini, and L. Bellodi
Table 1. The Gambling Task in Decision-Making Studies: A Review in Psychiatric Disorders
Authors
Wilder et al.
Year
Samples
1998 12 schizophrenic (SCZ)
Bechara et al.
30 healthy control (HC)
2000 30 drug abusers (DA)
24 healthy control (HC)
2001a 41 substance dependent (SD)
Clark et al.
5 ventromedial lesion (VM)
40 healthy control (HC)
2001 15 manic
Grant et al.
Performance at the
Gambling Task
SCZ = HC
SCZ = HC at California Verbal Learning Test, Letter Number
Span, Wisconsin Card Sorting Test
DA < HC
DA = HC at Wisconsin Card Sorting Test
SD = VM
SD = VM = HC at Wais-III, Benton Visual Retention Test and
Rey Auditory Verbal Learning Test
SD = VM at Stroop and Tower of Hanoi
SD < VM and HC at Wisconsin Card Sorting Test
Manic = HC at Tower of London, Spatial Working Memory,
Intradimensional/extradimensional attentional shift and Stroop
Color Tests
Manic < HC at Rapid visual information processing tasks and
Word Test
IED < HC at Facial Emotion Recognition Test and Odor
Identification Test
IED = HC at Working Memory Tests
PG = HC at Weigl’s Sorting Test and Wisconsin Card Sorting
Test
SD < HC
Manic = HC
30 healthy control (HC)
Best et al.
Cavedini et al.
2002 24 intermittent explosive
IED < HC
disorder (IED)
22 healthy control (HC)
2002 20 pathological gamblers (PG) PG < HC
Mitchell et al.
40 healthy control (HC)
2002 20 psychopathic (Psyc)
Psyc < HC
20 healthy control (HC)
Nielen et al.
Cavallaro et al.
Bechara and Martin
Ritter et al.
Cavedini et al.
2002 27 obsessive–compulsive
disorder (OCD)
26 healthy control (HC)
2003 110 schizophrenic (SCZ)
67 obsessive-compulsive
disorder (OCD)
56 healthy control (HC)
2004 substance dependence (SD)
healthy control (HC)
2004 20 schizophrenic (SCZ)
15 healthy control (HC)
2004 59 anorexic (AN)
Performance at Other Neuropsychological Tests
Psyc = HC at Raven’ s Advanced Progressive Matrices and
Intradimensional/extradimensional shift task (attentional
set-shifting)
Psyc < HC Intradimensional/extradimensional shift task (response
reversal)
OCD = HC
OCD < HC
OCD < SCZ
SCZ < OCD and HC at Wisconsin Card Sorting Test
SCZ and OCD < HC at Torre di Hanoi
SD < HC
SD < HC at Delayed nonmatching to sample task
SKZ < HC
SKZ = HC (poor performace) at Wisconsin Card Sorting Test
AN < HC
AN = HC at Wisconsin Card Sorting Test, Weigl’s Sorting Test
and Object Alternation Test
82 healthy control (HC)
Source: NLM-PubMed.
mental compulsions that characterize OCD. Both samples were tested using the GT and compared with a
control group. Both OCD and depressed patients appeared to be compromised in decision-making abilities
when compared with the control group, but a deeper
analysis showed some important differences between
the two groups. In fact, considering their neuropsychological performances and the severity of symptoms,
analysis of covariance showed a significant effect of
symptom severity on the number of disadvantageous
cards selected in affective patients, but not in OCD.
The conclusions were that, although poor performance
seems to be a specific trait of OCD unrelated to the
severity of illness, the decision-making profile of depressed patients correlates with severity of depressive
symptoms and may be considered a state instead of a
trait.
Opposite results has been achieved in OCD in a preliminary study by Nielen et al. (2002), who did not find
any difference between decision-making performance of
27 OCD patients and a group of healthy volunteers. They
found that the ability to adjust choices was independently
associated with both anxiety and OCD severity, suggesting a relationship between symptoms and risk adjustment:
�Decision-Making in Obsessive–Compulsive Disorder
Fig. 3. Strategy of Gambling Task performance of control subjects versus OCD patients, calculated as total number of “advantageous” minus
“disadvantageous” cards selected in each block of 20 cards. (Modified
from Cavedini et al., Neuropsychologia, 40 (2002) 205–211).
patients with high OCD severity tended to take more risks
than patients with moderate OCD. A reasonable explanation for this was that individuals with high trait anxiety
are more reactive to punishment, leading to increased expectancies of punishment (Zinbarg and Mohlman, 1998).
Decision-Making Impairments in the
Obsessive–Compulsive Spectrum
The GT has also been used to assess neuropsychological similarities between OCD and other psychiatric disorders belonging to the so-called “obsessive-compulsive
spectrum” (Hollander, 1998). In an early study, Cavedini
et al. (2002b) tested the GT in a sample of pathological
gamblers, finding that their performance was very similar to that of OCD patients. In fact, they deliberately
chose disadvantageous decks to obtain an immediate reward, careless about the long-term negative effects of their
choices, such as disruptive behavior in gambling and daily
life. Even if limited data are available about the validity of
the diagnosis of pathological gambling and about the etiology of this disorder, these neuropsychological findings
support the hypothesis that pathological gambling belongs
to the OCD spectrum, lying at the impulsive extreme on
the compulsive–impulsive dimension.
In a second study, the GT was administered to a
sample of patients with anorexia nervosa (Cavedini et al.,
2004) and showed that the supposed impairment in decision making did not appear to be related to some measure of illness severity or to gender and age, suggesting the absence of any relationship between nutritional
9
status, severity of symptoms, and general cognitive impairment in these subjects. However, differently to from
OCD, anorexic patients chose cards randomly, showing
a lack of strategy that could be an expression of their
inability to maximize immediate reward or to program
a postponed reward. The psychopathological and behavioral consequences of their decision-making deficiency
could be found in the pathological eating behavior that
patients with anorexia nervosa exhibit. In fact, to obtain
an immediate reward, consisting in the relief of anxiety
elicited by food phobia, and to neutralize the fear of gaining weight, they chose to avoid taking in calories, ignoring
long-term negative consequences of their choices characterized by the progressive and severe inevitable decline
of their physical condition. A review of the literature on
neuropsychological deficits in eating disorders and the
relationship between cognitive deficits and psychosocial
development has proposed a significant association between the presence of neuropsychological deficits and the
development of these disorders (Lena et al., 2004). Further research is necessary to assess the role of executive
functions, in general, and decision making, in particular,
in the etiology of eating disorders.
Even if preliminary, these neuropsychological studies support the hypothesis that these disorders belong to
the OCD spectrum, and could be helpful in the construction of a common neurofunctional model, in spite of a different phenomenological description of these disorders.
NEURAL CORRELATES OF THE GAMBLING
TASK PERFORMANCE
The data mentioned in the previous sections highlight the contribution of neuropsychology to the localizatory hypothesis. In the case of the GT, the investigation
started from specific deficits consequent to circumscribed
cerebral lesions (ventromedial patients) helps us to derive
some anatomical inferences about patients characterized
by similar cognitive impairments. The next step will be to
combine the use of neuropsychological investigation and
neuroimaging techniques.
At present, no imaging data are available for the GT
in OCD, but there are some data regarding the correlation between cerebral activation and the GT performance
in other neurological and psychiatric disorders. For example, Adinoff et al. (2003) observed that in cocainedependent subjects the anterior cingulate and left dorsolateral prefrontal cortex regional cerebral blood flow at rest
were significantly correlated with the performance on the
GT. Similarly, Bolla et al. (2003) observed, in a positron
emission tomography (PET) study, that cocaine abusers
�10
showed greater activation during the GT performance in
the right OFC and less activation in the right dorsolateral
prefrontal cortex and left medial prefrontal cortex compared to a control group, while better GT performance was
associated with greater activation in the right OFC both
in cocaine abusers and in the control group. Other significant results about the contribution of the frontal cortex
in decision making come from Clark et al. (2003), who
showed that, in the GT, patients with right frontal lesions
preferred the risky decks differing from left frontal and
control subjects. Moreover, within the right frontal group,
the preference for the risky decks was correlated with the
total lesion volume and the volume of damage outside of
the ventromedial prefrontal region.
BIOLOGICAL CONSIDERATIONS OF
DECISION-MAKING IMPAIRMENT IN OCD
The comprehension of neurobiological model of
OCD has produced important advances also in clinical and
therapeutical perspectives through the studies of neurotransmitters systems involved in its etiopathogenesis and
the effects of specific drugs on its symptomatology.
A large amount of evidence indicates that chronic
administration of amphetamine can induce enduring reductions in monoamine levels, both dopamine in the striatum and serotonin (5-hydroxytryptamine, 5-HT) in the
prefrontal cortex, as long as a kind of cognitive deficit,
particularly in executive functions, is demonstrated in patients with focal lesions to these neural areas (Ersche et al.,
2005).
Clinical evidence has also indicated that drug abusers
display many of the behavioral traits that are typical of patients with frontal lobe damage (Eslinger and
Damasio, 1985) and emphasize the possible role of the
ascending mesostriatal and mesocortical dopamine systems and the ascending serotonin projection systems in
decision-making processes. In fact, patients with Parkinson’s disease (Bowen et al., 1975; Downes et al., 1989)
as well as nonhuman primates (Brozoski et al., 1979;
Sawaguchi and Goldman-Rakic, 1991), show that altered
dopaminergic function is associated with some of the
cognitive impairments typically seen after damage to the
prefrontal cortex. These impairments can be ameliorated
by pharmacological agents acting on the mesostriatal and
mesocortical dopamine pathways (Arnsten, 1997; Lange
et al., 1992;). Consistent with these observations, subjects with a history of chronic abuse of amphetamine and
cocaine will themselves display decision-making deficits
similar to those present in patients with prefrontal cortex
or striatal damage.
P. Cavedini, A. Gorini, and L. Bellodi
Concerning the involvement of the ascending 5-HT
projection systems, further data come from the observation that normal subjects with a reduced central 5-HT activity after consumption of a tryptophan-depleting amino
acid drink, show decision-making deficits similar to those
seen after focal damage to OFC (Rogers et al., 1999).
A systematic analysis of the effects of neurochemical transmitters on GT performance has been provided
by Bechara and colleagues (Bechara et al., 2001b). By
manipulating dopamine and serotonin receptors, they observed that the blockade of both dopamine and serotonin
interfered with the selection of advantageous decks. In
particular, the dopamine effect seemed restricted to the
earlier part of the GT, when decisions are still guided by
covert knowledge (in this phase the subject is guided by
physiological activation instead of a conscious decision
to act) (Damasio, 1994), while the serotonin effect influenced only the latter part of the task when decisions are
mainly guided by conscious knowledge of which choices
are good or bad. As clearly expressed by Bechara (2003),
these results suggested that covert biasing of decision
might be dopaminergic, whereas overt biasing might be
serotoninergic.
The implication of serotonin in the pathophysiology of OCD justifies the interest in correlating
decision-making with pharmacological effects of proserotoninergic drugs, analyzing the treatment outcome
and the GT performance in different subgroups of OCD
patients. It was observed that after 12 weeks of treatment with a standardized pro-serotonergic medication,
patients could be subdivided into “Responders” and “NonResponders” on the basis of the presence or absence
of a reduction of the Y-BOCS total score greater or
equal to 40% (Cavedini et al., 2002a). It was also noticed that, before the beginning of the treatment, there
were important individual differences in decision-making
performance within the OCD group: responders played
at the GT as well as controls did, whereas the nonresponder patients showed a compromised decision-making
profile. The heterogeneity in decision-making profiles
of OCD could be reasonably considered as a predictive factor of response to anti-obsessive pharmacological treatments and the GT performance may be considered a valid criterion for choosing pharmacological treatment in OCD starting from the observation
that anti-obsessive treatment outcome is increased to
85% of responders choosing an appropriate drug strategy according to the GT performance (Cavedini et al.,
2004).
Another possible valid predictor of positive response
to pro-serotoninergic treatment has been found in the
analysis of genetic variations of 5-HT transporter gene
�Decision-Making in Obsessive–Compulsive Disorder
expressions. Genetical studies have found in OCD three
allelic variations (ll = wild, SS = reduced expression, ls = intermediate) and, in OCD patients without a co-diagnosis for tic disorder, a significant time
per genotype interaction for the Yale-Brown ObsessiveCompulsive score was found: patients with ls genotype showed a greater reduction of obsessive–compulsive
symptoms severity (Di Bella et al., 2002).
Additional studies are needed to assess a possible common role of these two predictive factors (performance at the GT and genotype) to better understand
treatment response mechanisms in OCD (Cavedini et al.,
2002c).
The Somatic Marker Hypothesis
As mentioned earlier, several studies have stressed
the role of the OFC in reward mechanisms (Rahman et al.,
1999). Studying conditioned learning processes and the
ability to modify or suppress responses initially linked
to reward, Rolls (2000) concluded that the OFC plays a
crucial role in the association between external stimuli
and internal reward mechanisms.
The link between external stimuli and internal
states and the possible functions of the prefrontal cortex
have been assessed by the “somatic marker hypothesis”
(Damasio, 1996; Damasio et al., 1991), which hypothesize
that when an individual faces a decision, each alternative
elicits a physiological state that corresponds to an emotional reaction. This “marker” signals act at multiple levels
of operation: some occur overtly (consciously) and some
occur covertly (nonconsciously). The marker signals arise
in bioregulatory processes that are related to emotions and
feelings but also to the physiological state structure and
regulation.
The somatic marker hypothesis provides an account
of deficits in decision-making, positing that they are the
result of defective activation of somatic markers that normally function as covert or overt signposts for helping to
make advantageous choices.
The somatic marker hypothesis has been repeatedly
tested by Bechara et al. (1996, 2000) using measures
of skin conductance responses (SCRs). They observed
that during the administration of the GT, normal subjects begin to avoid the decks with high immediate gains
(disadvantageous decks). They also start to produce anticipatory SCRs before their selection of a disadvantageous response. In contrast,, ventromedial patients continue to select more cards from the disadvantageous decks,
failing to produce any anticipatory SCRs. The insensitivity to punishment seems to be associated with lower
11
than normal punishment SCRs, while the hypersensitivity to reward would be associated with the generation
of reward SCRs with a magnitude higher that normal.
The anticipatory SCR appears to be a component of a
warning to subjects that they are about to make a risky
choice.
Starting from the “somatic marker hypothesis,”
Bechara et al. (1996) showed that the absence of anticipatory skin conductance response in patients with prefrontal
damage is correlated with their insensitivity to future outcomes, positive or negative, suggesting that these subjects
fail to generate somatic signals that would serve as physiological markers in the distinction between advantageous
and disadvantageous choices and are guided primarily by
immediate prospects.
Considering this evidences, the somatic state during the GT performance was also assessed in OCD
(Cavedini et al., 2003). Psychophysiological parameters
such as respiration effort, heart frequency, and muscle
tension were recorded at rest and during the task in 10
OCD patients and 10 healthy controls. Analysis of these
physiological parameters showed that all mean values
were significantly higher in OCD than in healthy subjects at the rest, probably of because of anxiety that characterizes the psychopathological profile of OCD; nevertheless, data from the somatic variations recorded during the task showed that, while all physiological mean
values in control subjects started from a lower level
at rest and increased during the decision-making task,
in OCD this modulation was absent. In a recent study
(Zorzi, 2004) the authors also investigated the SCR activation in a sample of 23 OCD compared to 18 control subjects during the GT. The main finding revealed
that control subjects show an increase in the SCR before and after a disadvantageous choice, while the OCD
patients show a lack of SCR modulation either during
the selection of advantageous or disadvantageous decks.
The absence of a somatic modulatory function in OCD
could be a valid explanation for their deficit in decisionmaking.
Even if these are preliminary results, they encourage further investigation into the somatic marker hypothesis in OCD and, in a larger view, the modulation
of emotions in this psychiatric disorder. In fact, clinical and experimental evidences suggested that the OFC,
presumably through its rich interconnections with limbic cortices and other neural stations deeply implicated
in processes of incentive motivation and reinforcement,
represents an important contact between emotional and
affective information and mechanisms of action selection.
Nevertheless, clinical observation of patients with anxiety disorders also suggests the presence of heterogeneous
�12
mechanisms of emotional processing, such as different
patterns of avoidance behavior or ability to decondition
from phobic stimuli. These considerations will address
future pathways of neuropsychological and neurophysiological research in psychiatric disorders, particularly in
OCD.
CONCLUSIONS
This article describes the state of the art concerning
the neuropsychological aspects and clinical implications
of decision-making in OCD. Unlike in other areas of neuropsychology, literature on decision-making in psychiatric disorders is scarce, but there are sufficient data to
support the hypothesis that deeper investigations in this
area could provide a better understanding of the pathophysiology of OCD and related disorders.
Mental disorders are considered to arise in the
brain and the new goal of “scientific psychopathology”
(Andreasen, 1997) is to identify the neural mechanisms
of normal cognitive processes and to understand how
they are injured in mental illnesses. Besides the classical
psychiatric classifications based on convergence of signs,
symptoms, outcome, and patterns of familial aggregation,
integration between neuropsychology, neuroanatomy, and
neurobiology allows the development of sophisticated and
powerful models that explain the cognitive dysfunction
of psychiatric patients based on knowledge of normal
brain/mind function.
Use of multiple neuroscience techniques, such as
neuropsychological measures in conjunction with psychophysiological and functional neuroradiological ones,
indicates that the neural mechanisms of mental illness can
be understood as a dysfunction in specific neural circuits
and that their functions and dysfunctions can be influenced
or altered by a variety of internal and external states.
With regard to OCD, the combined use of different
techniques has shown that the decision-making impairment is specifically related to the functioning of the ventromedial prefrontal cortex. Similarly, neuroimaging and
pharmacological studies have suggested the role of serotonin and dopamine systems in the expression of OCD
symptoms as well as in decision-making performance.
Combined use of different lines of investigation is
aimed to dissect the phenotypic heterogeneity of OCD
that risks to reduce the power and to obscure the findings coming from experimental and clinical investigations
and that is underestimated by most of the current models of OCD. The presence of different symptoms, from
intrusive thoughts to checkers or washer rituals, the differences observed in the level of patients’ insights and
P. Cavedini, A. Gorini, and L. Bellodi
the different responses to anti-obsessive pharmacological treatment suggest the existence of different biological subtypes of OCD. Studies on the neuropsychology of
decision-making processes and related neurophysiological substrates could be a helpful approach to characterize
possible sources of homogeneity between different patterns of disease, according to the direction proposed by
Mataix-Cols et al. (2004, 2005) of a multidimensional
model that may extend beyond the traditional nosological
boundaries of OCD and closely related phenotypes.
Moreover, a deeper investigation of the role of the
somatic state modulation in OCD patients during the GT
could be useful in formulating a model for the role of anxiety in this disorder. The main point that remains unclear is
if the anxiety that characterizes OCD is responsible for the
impairment in decision-making or if the decision-making
impairment is one of the traits specific for this pathology.
This point could be assessed by studying in depth the role
of the somatic changes during the administration of specific decision-making tests other than the gambling task.
The use of different decision-making tasks, such as, for
example, the gambling tasks proposed by Rogers (1999),
in which subjects choose between contingencies that are
presented in a readily comprehensive format, could facilitate the interpretation of how an individual patient’s
pattern of choices might change across a range of welldefined and clearly presented contingencies, instead of
condition in which the underlying contingencies relating
actions to relevant outcomes remain hidden.
It is important to realize that these types of investigations go beyond merely interesting research and are
very useful for a calibration of innovative behavioral and
clinical approaches that can bring relief from obsessive–
compulsive symptoms.
ACKNOWLEDGMENTS
The authors wish to thank Clementina Baraldi,
PsyD, Tommaso Bassi, MD, Monica Piccinni PsyD and
Claudia Zorzi, MD, at our University, for their hard work
on decision-making studies of obsessive–compulsive
spectrum disorders and for their invaluable cooperation
in discussing this review.
REFERENCES
Abbruzzese, M., Bellodi, L., Ferri, S., and Scarone, S. (1995a). Frontal
lobe dysfunction in schizophrenia and obsessive-compulsive disorder: A neuropsychological study. Brain Cogn. 27(2): 202–212.
Abbruzzese, M., Ferri, S., and Scarone, S. (1995b). Wisconsin Card
Sorting Test performance in obsessive-compulsive disorder: no
�Decision-Making in Obsessive–Compulsive Disorder
evidence for involvement of dorsolateral prefrontal cortex. Psychiatry
Res. 58(1): 37–43.
Adinoff, B., Devous, M. D., Sr., Cooper, D. B., Best, S. E.,
Chandler, P., Harris, T., Cervin, C. A., and Cullum, C. M. (2003).
Resting regional cerebral blood flow and gambling task performance
in cocaine-dependent subjects and healthy comparison subjects. Am.
J. Psychiatry 160(10): 1892–1894.
Alexander, G. E., DeLong, M. R., and Strick, P. L. (1986). Parallel
organization of functionally segregated circuits linking basal ganglia
and cortex. Annu. Rev. Neurosci. 9: 357–381.
American Psychiatric Association (2000). DSM-IV-TR. Diagnostic and
Statistical Manual of Mental Disorders. (4th ed.) Text Revision APA,
Washington, DC.
Andreasen, N. C. (1997). Linking mind and brain in the study of
mental illnesses: a project for a scientific psychopathology. Science
275(5306): 1586–1593.
Arnsten, A. F. (1997). Catecholamine regulation of the prefrontal cortex.
J. Psychopharmacol. 11(2): 151–162.
Bannon, S., Gonsalvez, C. J., Croft, R. J., and Boyce, P. M. (2002).
Response inhibition deficits in obsessive-compulsive disorder. Psychiatry Res. 110(2): 165–174.
Baxter, L. R., Jr., Phelps, M. E., Mazziotta, J. C., Guze, B. H., Schwartz,
J. M., and Selin, C. E. (1987). Local cerebral glucose metabolic
rates in obsessive-compulsive disorder. A comparison with rates in
unipolar depression and in normal controls. Arch. Gen. Psychiatry
44(3): 211–218.
Baxter, L. R., Jr., Schwartz, J. M., Bergman, K. S., Szuba, M. P., Guze,
B. H., Mazziotta, J. C., et al. (1992). Caudate glucose metabolic
rate changes with both drug and behavior therapy for obsessivecompulsive disorder. Arch. Gen. Psychiatry 49(9): 681–689.
Bechara, A. (2003). Risky business: Emotion, decision-making, and
addiction. J. Gambl. Stud. 19(1): 23–51.
Bechara, A., Damasio, H., and Damasio, A. R. (2001b). Manipulation
of dopamine and serotonin caused differents on covert and overt
decision-making. Society for Neuroscience Abstract, 27.
Bechara, A., Damasio, A. R., Damasio, H., and Anderson, S. W. (1994).
Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 50(1–3): 7–15.
Bechara, A., Damasio, H., Damasio, A. R., and Lee, G. P. (1999).
Different contributions of the human amygdala and ventromedial
prefrontal cortex to decision-making. J. Neurosci. 19(13): 5473–
5481.
Bechara, A., Damasio, H., Tranel, D., and Anderson, S. W. (1998).
Dissociation of working memory from decision making within the
human prefrontal cortex. J. Neurosci. 18(1): 428–437.
Bechara, A., Dolan, S., Denburg, N., Hindes, A., Anderson, S. W.,
and Nathan, P. E. (2001a). Decision-making deficits, linked to a
dysfunctional ventromedial prefrontal cortex, revealed in alcohol and
stimulant abusers. Neuropsychologia 39(4): 376–389.
Bechara, A., and Martin, E. M. (2004). Impaired decision making related
to working memory deficits in individuals with substance addictions.
Neuropsychology 18(1): 152–162.
Bechara, A., Tranel, D., and Damasio, H. (2000). Characterization of
the decision-making deficit of patients with ventromedial prefrontal
cortex lesions. Brain 123(Pt 11): 2189–2202.
Bechara, A., Tranel, D., Damasio, H., and Damasio, A. R. (1996). Failure
to respond autonomically to anticipated future outcomes following
damage to prefrontal cortex. Cereb. Cortex. 6(2): 215–225.
Benkelfat, C., Nordahl, T. E., Semple, W. E., King, A. C., Murphy, D. L.,
and Cohen, R. M. (1990). Local cerebral glucose metabolic rates in
obsessive-compulsive disorder. Patients treated with clomipramine.
Arch. Gen. Psychiatry 47(9): 840–848.
Best, M., Williams, J. M., and Coccaro, E. F. (2002). Evidence for a dysfunctional prefrontal circuit in patients with an impulsive aggressive
disorder. Proc. Natl. Acad. Sci. USA 99(12): 8448–8453.
Bolla, K. I., Eldreth, D. A., London, E. D., Kiehl, K. A., Mouratidis,
M., Contoreggi, C., et al. (2003). Orbitofrontal cortex dysfunction in
abstinent cocaine abusers performing a decision-making task. Neuroimage 19(3): 1085–1094.
13
Bowen, F. P., Kamienny, R. S., Burns, M. M., and Yahr, M. (1975).
Parkinsonism: Effects of levodopa treatment on concept formation.
Neurology 25(8): 701–704.
Brozoski, T. J., Brown, R. M., Rosvold, H. E., and Goldman, P. S.
(1979). Cognitive deficit caused by regional depletion of dopamine
in prefrontal cortex of rhesus monkey. Science 205(4409): 929–932.
Cavallaro, R., Cavedini, P., Mistretta, P., Bassi, T., Angelone, S. M., Ubbiali, A., et al. (2003). Basal-corticofrontal circuits in schizophrenia
and obsessive-compulsive disorder: A controlled, double dissociation
study. Biol. Psychiatry 54(4): 437–443.
Cavedini, P., Bassi, T., Ubbiali, A., Casolari, A., Giordani, S., and Zorzi,
C., et al. (in press). Neuropsychological investigation of decisionmaking in anorexia nervosa. Psychiatry Res 127(3): 259–266.
Cavedini, P., Bassi, T., Zorzi, C., and Bellodi, L. (2004). The advantages of choosing antiobsessive therapy according to decision-making
functioning. J. Clin. Psychopharmacol. 24(6): 628–631.
Cavedini, P., Cisima, M., Riboldi, G., D’Annucci, A., and Bellodi, L.
(2001). A neuropsychological study of dissociation in cortical and
subcortical functioning in obsessive-compulsive disorder by Tower
of Hanoi task. Brain Cogn. 46(3): 357–363.
Cavedini, P., D’Annucci, A., Riboldi, G., Cisima, M., and Bellodi, L. (2000). Neuropsychology of obsessive-compulsive disorder:
relationship to response. Paper presented at the 1st ECNP Workshop,
Nizza (France).
Cavedini, P., Ferri, S., Scarone, S., and Bellodi, L. (1998). Frontal lobe
dysfunction in obsessive-compulsive disorder and major depression:
A clinical-neuropsychological study. Psychiatry Res. 78(1-2): 21–28.
Cavedini, P., Riboldi, G., D’Annucci, A., Belotti, P., Cisima, M., and
Bellodi, L. (2002a). Decision-making heterogeneity in obsessivecompulsive disorder: Ventromedial prefrontal cortex function predicts different treatment outcomes. Neuropsychologia 40(2): 205–
211.
Cavedini, P., Riboldi, G., Keller, R., D’Annucci, A., and Bellodi, L.
(2002b). Frontal lobe dysfunction in pathological gambling patients.
Biol. Psychiatry 51(4): 334–341.
Cavedini, P., Zorzi, C., Giordani, S., D’Annucci, A., Bassi, T., and Di
Bella, D. (2002c). The role of HT-5 carrier genotype in decisionmaking impairment of OCD patients. Am. J. Med. Genet. 114(7):
224.
Cavedini, P., Zorzi, C., Ubbiali, A., Gorini, A., D’Annucci, A., Bassi, T.,
et al. (2003). The neurophysiology of decision-making in obsessivecompulsive disorder. Brain Cogn. 51(2): 236–237.
Chamberlin, S. R., Blackwell, A. D., Fineberg, N. A., Robbins, T. W.,
and Sahakian, B. J. (2005). The neuropsychology of obsessive compulsive disorder: the inhibition as candidate endophenotypic markers
importance of failures in cognitive and behavioural. Neurosci. Behav.
Reviews 29(3): 399–419.
Clark, L., Lversen, S. D., and Goodwin, G. M. (2001). A neuropsychological investigation of prefrontal cortex involvement in acute mania.
Am. J. Psychiatry. 158(10): 1605–1611.
Clark, L., Manes, F., Antoun, N., Sahakian, B. J., and Robbins, T. W.
(2003). The contributions of lesion laterality and lesion volume to
decision-making impairment following frontal lobe damage. Neuropsychologia 41(11): 1474–1483.
Damasio, A. R. (1994). Descartes’ Error : Emotion, Reason, and the
Human Brain, New York: G.P. Putnam’ s Sons.
Damasio, A. R. (1996). The somatic marker hypothesis and the possible
functions of the prefrontal cortex. Philos. Trans. R. Soc. Lond. B.
Biol. Sci. 351(1346): 1413–1420.
Damasio, A. R., Tranel, D., and Damasio, H. (1991). Somatic markers
and the guidance of behavior: Theory and preliminary testing. In
Levin, H. S., Eisemberg, H. M., and Benton A. L. (eds.), Frontal Lobe
Function and Dysfunction. Oxford University Press, New York.
Denys, D., van der Wee, N., Janssen, J., De Geus, F, and Westenberg,
H. G. (2004). Low level of dopaminergic D2 receptor binding in
obsessive-compulsive disorder. Biol. Psychiatry 55(10): 1041–1045.
Di Bella, D., Erzegovesi, S., Cavallini, M. C., and Bellodi, L. (2002).
Obsessive-compulsive disorder, 5-HTTLPR polymorphism and treatment response. Pharmacogenomics J. 2(3): 176–181.
�14
Di Russo, F., Zaccara, G., Ragazzoni, A., and Pallanti, S. (2000). Abnormal visual event-related potentials in obsessive-compulsive disorder
without panic disorder or depression comorbidity. J. Psychiatr Res.
34(1): 75–82.
Downes, J. J., Roberts, A. C., Sahakian, B. J., Evenden, J. L., Morris,
R. G., and Robbins, T. W. (1989). Impaired extra-dimensional shift
performance in medicated and unmedicated Parkinson’s disease: evidence for a specific attentional dysfunction. Neuropsychologia 27(1112): 1329–1343.
El-Sayegh, S., Bea, S., and Agelopoulos, A. (2003). Obsessivecompulsive disorder: unearthing a hidden problem. Cleve. Clin. J.
Med. 70(10): 824–825, 829–830, 832–823, passim.
Ersche, K. D., Fletcher, P. C., Lewis, S. J., Clark L., Stocks-Gee G.,
London M., Deakin J. B., Robbins T. W., and Sahakian B. J. (2005).
Abnormal frontal activations related to decision-making in current
and former amphetamine and opiate dependent individuals. Psychofarmacology 180(4): 612–623.
Eslinger, P. J., and Damasio, A. R. (1985). Severe disturbance of higher
cognition after bilateral frontal lobe ablation: Patient EVR. Neurology
35(12): 1731–1741.
Fernandez, A., Pino Alonso, M., Mataix-Cols, D., Roca, M., Vallejo, J.,
Puchal, R., et al. (2003). Neuroactivation of the Tower of Hanoi in
patients with obsessive-compulsive disorder and healthy volunteers.
Rev. Esp. Med. Nucl. 22(6): 376–385.
Grant, S., Contoreggi, C., and London, E. D. (2000). Drug abusers
show impaired performance in a laboratory test of decision making.
Neuropsychologia 38(8): 1180–1187.
Greisberg, S., and McKay, D. (2003). Neuropsychology of obsessivecompulsive disorder: A review and treatment implications. Clin. Psychol. Rev.. 23(1): 95–117.
Gross-Isseroff, R., Sasson, Y., Voet, H., Hendler, T., Luca-Haimovici, K.,
Kandel-Sussman, H., et al. (1996). Alternation learning in obsessivecompulsive disorder. Biol. Psychiatry 39(8): 733–738.
Hollander, E. (1998). Treatment of obsessive-compulsive spectrum disorders with SSRIs. Br. J. Psychiatry Suppl. (35): 7–12.
Hollander, E., Prohovnik, I., and Stein, D. J. (1995). Increased cerebral blood flow during m-CPP exacerbation of obsessive-compulsive
disorder. J. Neuropsychiatry Clin. Neurosci. 7(4): 485–490.
Hommer, D., Andreasen, P., Rio, D., Williams, W., Ruttimann, U., Momenan, R., et al. (1997). Effects of m-chlorophenylpiperazine on
regional brain glucose utilization: A positron emission tomographic
comparison of alcoholic and control subjects. J. Neurosci. 17(8):
2796–2806.
Jenike, M. A., Breiter, H. C., Baer, L., Kennedy, D. N., Savage, C. R.,
Olivares, M. J., et al. (1996). Cerebral structural abnormalities in obsessivecompulsive disorder. A quantitative morphometric magnetic
resonance imaging study. Arch. Gen. Psychiatry 53(7): 625– 632.
Kim, J. J., Lee, M. C., Kim, J., Kim, I. Y., Kim, S. I., Han, M., et al.
(2001). Grey matter abnormalities in obsessive-compulsive disorder:
Statistical parametric mapping of segmented magnetic resonance images. Br. J. Psychiatry 179: 330–334.
Kuelz, A. K., Hohagen, F., and Voderholzer, U. (2004). Neuropsychological performance in obsessive-compulsive disorder: A critical review.
Biol. Psychol. 65(3): 185–236.
Kwon, J. S., Kim, J. J., Lee, D. W., Lee, J. S., Lee, D. S., Kim, M.
S., et al. (2003). Neural correlates of clinical symptoms and cognitive dysfunctions in obsessive-compulsive disorder. Psychiatry Res.
122(1): 37–47.
Lacerda, A. L., Dalgalarrondo, P., Caetano, D., Haas, G. L., Camargo,
E. E., and Keshavan, M. S. (2003). Neuropsychological performance
and regional cerebral blood flow in obsessive-compulsive disorder.
Prog. Neuropsychopharmacol Biol. Psychiatry 27(4): 657–665.
Lange, K. W., Robbins, T. W., Marsden, C. D., James, M., Owen, A. M.,
and Paul, G. M. (1992). L-dopa withdrawal in Parkinson’s disease
selectively impairs cognitive performance in tests sensitive to frontal
lobe dysfunction. Psychopharmacology (Berl) 107(2-3): 394–404.
Lena, S., Fiocco, A., and Leynaar, J. (2004). The role of cognitive
deficits in the development of eating disorders. Neuropsychol Rev.
14(2): 99–113.
P. Cavedini, A. Gorini, and L. Bellodi
Leocani, L., Locatelli, M., Bellodi, L., Fornara, C., Henin, M., Magnani,
G., et al. (2001). Abnormal pattern of cortical activation associated
with voluntary movement in obsessive-compulsive disorder: An EEG
study. Am. J. Psychiatry 158(1): 140–142.
Machlin, S. R., Harris, G. J., Pearlson, G. D., Hoehn-Saric, R., Jeffery, P., and Camargo, E. E. (1991). Elevated medial-frontal cerebral
blood flow in obsessive-compulsive patients: a SPECT study. Am. J.
Psychiatry 148(9): 1240–1242.
Mataix-Cols, D., Junque, C., Sanchez-Turet, M., Vallejo, J., Verger, K.,
and Barrios, M. (1999). Neuropsychological functioning in a subclinical obsessive-compulsive sample. Biol. Psychiatry 45(7): 898–904.
Mataix-Cols, D., Rosario-Campos, M. C., and Leckman, J. F. (2005).
A multidimensional model of obsessive-compulsive disorder. Am. J.
Psychiatry 162(2): 228–238.
Mataix-Cols, D., Wooderson, S., Lawrence, N., Brammer, M. J., Speckens, A., and Phillips, M. L. (2004). Distinct neural correlates of
washing, checking, and hoarding symptom dimensions in obsessivecompulsive disorder. Arch. Gen. Psychiatry 61(6): 564–576.
Metz, C., and Kronman, H. (1987). Statistical significance test for the
binomial ROC curves. J. Math Psychol. 22: 218–243.
Mitchell, D. G., Colledge, E., Leonard, A., and Blair, R. J. (2002). Risky
decisions and response reversal: is there evidence of orbitofrontal
cortex dysfunction in psychopathic individuals? Neuropsychologia
40(12): 2013–2022.
Mora, F., Avrith, D. B., Phillips, A. G., and Rolls, E. T. (1979). Effects
of satiety on self-stimulation of the orbitofrontal cortex in the rhesus
monkey. Neurosci. Lett. 13(2): 141–145.
Mora, F., and Cobo, M. (1990). The neurobiological basis of prefrontal
cortex self-stimulation: a review and an integrative hypothesis. Prog.
Brain Res. 85: 419–431.
Murray, C. J., and Lopez, A. D. (1996). Global burden of disease: a
comprehensive assessment of mortality and morbidity from diseases,
injuries and risk factors in 1990 and projected to 2020 (Vol. 1),
WHO, Harvard.
Nakano, Y., Oomura, Y., Nishino, H., Aou, S., Yamamoto, T., and
Nemoto, S. (1984). Neuronal activity in the medial orbitofrontal
cortex of the behaving monkey: Modulation by glucose and satiety.
Brain Res. Bull. 12(4): 381–385.
Nielen, M. M., Veltman, D. J., de Jong, R., Mulder, G., and den Boer,
J. A. (2002). Decision making performance in obsessive compulsive
disorder. J. Affect Disord. 69(1-3): 257–260.
Perani, D., Colombo, C., Bressi, S., Bonfanti, A., Grassi, F., Scarone,
S., et al. (1995). [18F]FDG PET study in obsessive-compulsive disorder. A clinical/metabolic correlation study after treatment. Br. J.
Psychiatry 166(2): 244–250.
Phillips, M. L., Marks, I. M., Senior, C., Lythgoe, D., O’Dwyer, A. M.,
Meehan, O., Williams, S. C., Brammer, M. J., Bullmore, E. T., and
McGuire, P. K. (2000). A differential neural response in obsessivecompulsive disorder patient with washing compared checking symptoms to disgust. Psychological Medicine 30(5): 1037–1050.
Phillips, A. G., Mora, F., and Rolls, E. T. (1979). Intracranial selfstimulation in orbitofrontal cortex and caudate nucleus of rhesus
monkey: effects of apomorphine, pimozide, and spiroperidol. Psychopharmacology (Berl) 62(1): 79–82.
Pitman, R. K. (1982). Neurological aetiology of obsessive-compulsive
disorders? Am. J. Psychiatry 139(1): 139–140.
Pogarell, O., Hamann, C., Popperl, G., Juckel, G., Chouker, M., Zaudig,
M., et al. (2003). Elevated brain serotonin transporter availability in
patients with obsessive-compulsive disorder. Biol. Psychiatry 54(12):
1406–1413.
Rahman, S., Sahakian, B. J., Hodges, J. R., Rogers, R. D., and Robbins, T. W. (1999). Specific cognitive deficits in mild frontal variant
frontotemporal dementia. Brain 122(Pt 8): 1469–1493.
Rapoport, J. L., and Wise, S. P. (1988). Obsessive-compulsive disorder:
evidence for basal ganglia dysfunction. Psychopharmacol Bull 24(3):
380–384.
Rauch, S. L., Jenike, M. A., Alpert, N. M., Baer, L., Breiter, H. C.,
Savage, C. R., et al. (1994). Regional cerebral blood flow measured
during symptom provocation in obsessive-compulsive disorder using
�Decision-Making in Obsessive–Compulsive Disorder
oxygen 15-labeled carbon dioxide and positron emission tomography.
Arch. Gen. Psychiatry 51(1): 62–70.
Ritter, L. M., Meador-Woodruff, J. H., and Dalack, G. W. (2004). Neurocognitive measures of prefrontal cortical dysfunction in schizophrenia. Schizphr Res. 68(1): 65–73.
Rogers, R. D., Everitt, B. J., Baldacchino, A., Blackshaw, A. J.,
Swainson, R., Wynne, K., et al. (1999). Dissociable deficits in
the decision-making cognition of chronic amphetamine abusers,
opiate abusers, patients with focal damage to prefrontal cortex, and
tryptophan-depleted normal volunteers: Evidence for monoaminergic mechanisms. Neuropsychopharmacology 20(4): 322–
339.
Rolls, E. T. (2000). The orbitofrontal cortex and reward. Cereb. Cortex.
10(3): 284–294.
Rubin, R. T., Ananth, J., Villanueva-Meyer, J., Trajmar, P. G., and
Mena, I. (1995). Regional 133-xenon cerebral blood flow and cerebral 99mTc-HMPAO uptake in patients with obsessive-compulsive
disorder before and during treatment. Biol. Psychiatry 38(7): 429–
437.
Sawaguchi, T., and Goldman-Rakic, P. S. (1991). D1 dopamine receptors in prefrontal cortex: Involvement in working memory. Science
251(4996): 947–950.
Saxena, S., Brody, A. L., Maidment, K. M., Dunkin, J. J., Colgan, M.,
Alborzian, S., et al. (1999). Localized orbitofrontal and subcortical
metabolic changes and predictors of response to paroxetine treatment
in obsessive-compulsive disorder. Neuropsychopharmacology 21(6):
683-693.
Saxena, S., Brody, A. L., Schwartz, J. M., and Baxter, L. R. (1998). Neuroimaging and frontal-subcortical circuitry in obsessive-compulsive
disorder. Br. J. Psychiatry Suppl. (35): 26–37.
Scarone, S., Colombo, C., Livian, S., Abbruzzese, M., Ronchi, P.,
Locatelli, M., et al. (1992). Increased right caudate nucleus size in
obsessive-compulsive disorder: detection with magnetic resonance
imaging. Psychiatry Res. 45(2): 115–121.
Simpson, H. B., Lombardo, I., Slifstein, M., Huang, H. Y., Hwang,
D. R., Abi-Dargham, A., et al. (2003). Serotonin transporters
in obsessive-compulsive disorder: A positron emission tomography study with [(11)C]McN 5652. Biol. Psychiatry 54(12): 1414–
1421.
View publication stats
15
Stein, D. J., Hollander, E., Chan, S., DeCaria, C. M., Hilal, S., Liebowitz,
M. R., et al.(1993). Computed tomography and neurological soft
signs in obsessive-compulsive disorder. Psychiatry Res. 50(3): 143–
150.
Swedo, S. E., Schapiro, M. B., Grady, C. L., Cheslow, D. L., Leonard,
H. L., Kumar, A., et al. (1989). Cerebral glucose metabolism in
childhood-onset obsessive-compulsive disorder. Arch. Gen. Psychiatry 46(6): 518–523.
Szeszko, P. R., McMillan, S., McMeniman, M., Chen, S., Baribault, K.,
Lim, K. O., Lvey, J., Rose, M., Banerjee, S. P., Bhandari, R., Moore,
G. J., and Rosenberg, D. R. (2004). Brain structural abnormalities in
psychotropic drugnaive pediatric patients with obsessive-compulsive
disorder. Am. J. Psychiatry. 161(6): 1049–1056.
Tataranni, P. A., Gautier, J. F., Chen, K., Uecker, A., Bandy, D., Salbe,
A. D., et al. (1999). Neuroanatomical correlates of hunger and satiation in humans using positron emission tomography. Proc. Natl.
Acad. Sci. USA 96(8): 4569–4574.
van den Heuvel, O. A., Veltman, D. J., Groenewegen, H. J., Cath, D. C.,
van Balkom, A. J. L. M., van Hartskamp, J., et al. (2005). Frontalstriatal dysfunction during planning in obsessive-compulsive disorder. Arch. Gen. Psychiatry 62(3): 301–309.
Volkow, N. D., and Fowler, J. S. (2000). Addiction, a disease of compulsion and drive: Involvement of the orbitofrontal cortex. Cereb. Cortex
10(3): 318–325.
Volkow, N. D., Fowler, J. S., Wolf, A. P., Hitzemann, R., Dewey, S.,
Bendriem, B., et al. (1991). Changes in brain glucose metabolism
in cocaine dependence and withdrawal. Am. J. Psychiatry 148(5):
621–626.
Wilder, K. E., Weinberger, D. R., and Goldberg, T. E. (1998). Operant
conditioning and the orbitofrontal cortex in schizophrenic patients:
Unexpected evidence for intact functioning. Schizophr Res. 30(2):
169–174.
Zinbarg, R. E., and Mohlman, J. (1998). Individual differences in the
acquisition of affectively valenced associations. J. Pers. Soc. Psychol
74(4): 1024–1040.
Zorzi, C. (2004). Neuropsychology of obsessive-compulsive disorder:
Presented at “neuropsychological function in psychopathology” at
The 8th Nordic Meeting in Neuropsychology, Turku, Finland, August
26–29.
�
 Melissa Allen Heath
Melissa Allen Heath